
Abstract
Morphology still remains the cornerstone in lung cancer classification and cytology and small biopsy samples should be interpreted by morphology, whenever feasible, according to shared and widely agreed-upon diagnostic schemes. However, as novel therapy strategies are being offered on the basis of the diverse tumor characteristics, pathologists are now challenged by the need to offer clinicians more detailed typing of non–small cell lung cancer, not otherwise specified (NSCLC-NOS), especially when dealing with limited diagnostic material or poorly differentiated tumors. Close integration of morphology, immunohistochemistry, and clinical data is highly warranted according to a multidisciplinary approach to limit the category of NSCLC-NOS as much as possible or exclude unsuspected metastases, so rendering more definite and clinically useful diagnoses. Among the many proposed immunohistochemical markers, which as a whole are more practical and diagnostically useful than cumbersome and expensive molecular assays, a 2-hit model including thyroid transcription factor-1 (TTF-1) and p40 (the latter more specific for squamous differentiation than p63) seems to be the most effective to basically highlight adenocarcinoma (positivity for TTF-1 regardless of p63) and squamous (always strongly and diffusely positive for p40 or p63 and negative for TTF-1) differentiation. This minimalist 2-hit diagnostic approach paves the way to novel perspectives in clinical trials on lung cancer, and it is also in keeping with the need of strategically preserving diagnostic material for molecular assays that are essential for personalizing therapies.
Introduction
The introduction of new effective chemotherapeutic agents and targeted therapies in the management of non–small cell lung cancer (NSCLC) has widened the spectrum of therapeutic choices in the oncologists’ hands.1-14 However, adoption of these new pharmaceutical agents requires predefinition of molecular features (ie, epidermal growth factor receptor [EGFR] mutations or anaplastic lymphoma kinase [ALK] translocation)15,16 or precise subtyping of NSCLC,17-20 at least dichotomizing squamous from nonsquamous cell carcinoma for clinical informed decisions to take. In addition, recent investigations have suggested that adenocarcinoma tends to metastasize to the lymph nodes and central nervous system with a significantly higher frequency than squamous cell carcinoma.21-23 Adenocarcinoma is also statistically associated with a better median survival time when brain metastases are radiotherapy treated or when radiotherapy is intended with a curative intent in NSCLC. 23
As highlighted for chemotherapy in the treatment of lung cancer, 24 even conventional morphology has reached a plateau in NSCLC subtyping. The most careful examination of microscopic features on cytology and small biopsies leave a substantial rate of NSCLC not otherwise specified (NOS; ranging from 10% to 30%), even in the hands of expert pulmonary pathologists.25-28 This is mainly because of the difficulty in translating all the morphologic findings observed at a cytology/biopsy level, particularly in poorly differentiated tumors,25-27 also because lung cancer classification has been constructed on resection specimens and only recently the issues of cytology and small biopsy specimens have been pointed out.27,29,30 Other sources of inconsistency may derive from the inherent heterogeneity of adenocarcinoma and interobserver variability because of the many histological subtypes and variants existing, 31 so the eventual subtyping of NSCLC may be affected according to the axiom “the more the tumor categories, the more the difficulties in diagnosis.” 32
In this frame of mind, immunohistochemistry (IHC) has been representing the ancillary technique with the best cost/benefit ratio in the distinction of NSCLC histotypes,27,34 whereas molecular methods, namely micro-RNA expression analysis, which have recently been proposed, are unlikely to be directly transferred into the everyday diagnostic workflow.35-38 Based on an extensive literature review and our own experience, in June 2009 we first suggested in this journal the adoption of an algorithm comprising the best antibodies at that time able to identify glandular (thyroid transcription factor-1 [TTF-1] and CK7) and squamous cell (p63 and CK5/6) differentiation in the setting of NSCLC. 34 Needless to say that IHC is not a perfect mathematic model, since there is a small subset of NSCLC (hopefully <5%) with ambiguous co-expression of glandular and squamous cell differentiation markers or negative reaction for any marker, which an unchanged eventual diagnosis of NSCLC-NOS may really be justified for, as pointed out in the recent International Association for the Study of Lung Cancer/European Respiratory Society/American Thoracic Society (IASLC/ERS/ATS) adenocarcinoma classification. 29 Presently, these tumor patients should undergo molecular assays for EGFR mutations or ALK translocation or be candidates for pemetrexed or bevacizumab therapy just like adenocarcinoma. 27
This review was aimed at critically summarizing the results of several published articles on NSCLC subtyping in the past 3 years, issuing some practical key messages to address the most limited panel of antibodies, including recently introduced markers (ideally 1 marker for adenocarcinoma and 1 marker for squamous cell carcinoma), compare older and newer diagnostic profiles, and provide some operational rules to follow in the routine practice for the most reliable diagnoses to render.
Morphologic Yield of Cytology and Biopsy Specimen Examination
The rate of NSCLC-NOS was very high in the past when there was no clinical reason for subtyping. 26 A systematic review by Paech et al 39 evidenced that the agreement between pathologists in discriminating squamous cell carcinoma from nonsquamous cell carcinoma on morphology alone was moderate to high (k = 0.48-0.84). Rekhtman et al 40 were able to perform a definitive diagnosis of NSCLC subtype in 169 out of 196 (88%) preoperative cytology samples by morphologic criteria alone. In addition, a diagnosis of favored histologic type was made in 8%, then leaving unclassified NSCLC-NOS in 4% of cases. Concordance between cytology and histology was of 93%. In 165 tumors with surgical diagnosis of squamous cell carcinoma or adenocarcinoma, preoperative cytology had an accuracy of 96%, reaching 100% when IHC stains were added. Nizzoli et al 41 claimed that cytology was able to subtype NSCLC in 85% of cases (158 out of 183), whereas only 2% of NSCLC (3 cases out of 183) were not classified at histology. The concordance between cytology and histology was consistently high (88% of cases, with k concordance value being 0.75). In both studies,40,41 squamous cell carcinoma histology had a lower accuracy rate when compared with adenocarcinoma. Comparing diagnosis on cytomorphology and surgical resection specimens in 53 cases, Khayyata et al 42 reported 66% accuracy for adenocarcinoma and 53% for squamous cell carcinoma, with combined accuracy for either diagnosis being 60%. Sigel et al 43 demonstrated that small biopsy and cytology have a similar rate of accuracy in NSCLC subtyping with a concordance value of 93% leading to a NSCLC-NOS rate of 4%. This excellent result clearly depends on the different expertise of pathologists in lung cancer recognition as recently evidenced by Pelosi et al. 44 The authors showed that the correct morphologic diagnoses on small biopsies of NSCLC arose from 67% to 84% when expert pathologists reviewed slides. 44 Finally, da Cunha Santos et al 45 confirmed the high agreement between fine-needle aspiration cytology and histology on surgical resections with an accuracy rate ranging from 96% to 85% in the diagnosis of adenocarcinoma and squamous cell carcinoma, respectively. Of note, the percentage of NSCLC-NOS significantly decreased from 35% to 24% for the clinical purposes of targeted therapies (P = .01) to reach 17% rate when exploiting IHC methods. 45
Relevant points to morphology: At least 70% of lung cancer patients are diagnosed in cytology and biopsy specimens by using only light microscope without attaining special stains.
What’s New From Immunohistochemical Studies
Several articles have investigated the value of IHC in NSCLC subtyping using different combinations/panel of antibodies.46-73 Overall, there is agreement in limiting the use of immunostains to preserve as much tissue as possible for molecular analyses, then performing 1 adenocarcinoma and 1 squamous marker, as also recommended in the new classification of adenocarcinoma.29,74
At the end, the coordinated expression for TTF-1 or napsin-A for adenocarcinoma and p63 or p40 for squamous cell carcinoma represents the most reasonable panel in terms of sensitivity and specificity.27,29,30 Detailing on few important articles, Downey et al 53 found that all squamous cell carcinomas (21 cases) were strongly positive for CK5/6 and negative for TTF-1, whereas some adenocarcinomas (2 out of 24) stained with CK5/6. More recently, Loo et al 57 evidenced that Alcian blue/periodic acid Schiff (AB/PAS) plus p63 and TTF-1 constituted the best panel in subtyping NSCLC with 86% of diagnostic accuracy. When prospectively applied to 82 biopsies, the concordance between the immunohistochemical panel results and morphologic subtype was complete (100%). The category of NSCLC-NOS was then downrated to 7%. Nicholson et al 58 demonstrated a NSCLC refinement in 65% of cases using a panel of stains, including TTF-1, p63, CK5/6, and PAS-diastase. The authors also underlined that high-molecular-weight cytokeratins cocktail 34βE12 showed consistent staining even in adenocarcinomas, then suggesting a limited role for this antibody. Khayyata et al 42 did not report immunoexpression for TTF-1 in squamous cell carcinoma, whereas reactivity for p63 and CK5/6 was not found in adenocarcinomas.
Pelosi et al 44 matched the immunoprofiles of small biopsies and surgical resections of 63 cases using a panel of markers comprising TTF-1, CK7, CK5/6, p63, and vimentin. Revised morphology recognized 84% of corrected cases, whereas 94% (59 out of 63) were correctly diagnosed on small biopsies using the aforementioned immunopanel. Squamous cell carcinomas did not stain for TTF-1, whereas 9 out of 31 expressed CK7. One and 7 out of 22 adenocarcinomas showed some staining with CK5/6 and p63, respectively. Hierarchic clustering analysis showed a nonrandom distribution of immunoprofiles both in surgical specimens and biopsies, this supporting the notion that IHC-assessed small biopsies by using TTF1, CK5/6 and CK7, p63, and vimentin could effectively parallel the corresponding profiling and hence eventual diagnoses on surgical specimens. Mukhopadhyay and Katzenstein 62 claimed the usefulness of an antibody panel comprising TTF-1, napsin-A, p63, and CK5/6 as the best combination in NSCLC subtyping examining a series of 20 adenocarcinomas, 15 squamous cell carcinomas, and 4 large cell carcinomas. In their series, TTF-1 and napsin-A selectively stained adenocarcinomas (80% and 58%, respectively) or large cell carcinomas (50% and none, respectively), but none of these markers was detected in squamous cell carcinomas. By contrast, p63 and CK5/6 stained 20% and 0% of adenocarcinomas, respectively. Of interest, the final suggested algorithm for NSCLC subclassification showed that squamous cell carcinoma was favored only when diffuse and strong immunostaining for p63 was observed in absence of TTF-1 and/or napsin-A expression. Otherwise, any staining for TTF-1 and/or napsin-A significantly featured adenocarcinoma. Since focal staining for p63 can be observed in TTF-1 negative/napsin-A negative adenocarcinomas, but never in squamous cell carcinoma, a diagnosis of poorly differentiated nonsquamous cell carcinoma seems to be reasonable in this occurrence. 62
Righi et al 59 recently tested several antibodies, including CK7, CK5, TTF-1, and p63 in a series of cellblocks from 103 fine-needle aspiration cytology samples. In addition, p63, p40, napsin-A, and desmocollin-3 were tested when discordant results were obtained using the first panel. In all cases, a correlation with the relevant surgical specimens was performed. Forty-six cases (44.7%) had a conventional immunoprofile (TTF-1/CK7 positive and p63/CK5 negative profile for adenocarcinoma and the opposite for squamous cell carcinomas). Fifty-seven cases had an ambiguous phenotype. In these cases, TTF-1 had the strongest predictive value in confirming adenocarcinoma, even when p63 was positive. Squamous cell carcinoma was favored when tumors were strongly positive for p63 and negative for TTF-1, whatever the immunostaining was for CK5 and CK7. Again, adenocarcinoma was favored in the presence of CK7 alone. At the end, only 14% of poorly differentiated tumors remained NSCLC-NOS in this series of cytologic samples. Of note, desmocollin-3 and p40 (the truncated variant of p63) consistently confirmed squamous cell carcinoma phenotype, whereas napsin-A was selectively expressed in adenocarcinomas. 59
In agreement with the majority of published works on this topic and previous gene expression profiling studies, Conde et al 60 found that p63 expression was strikingly and significantly associated with squamous cell carcinoma, whereas 2 cases of NSCLC-NOS co-expressing TTF-1 and p63 were considered to be squamous cell carcinoma. Disowning the work by Conde et al, 60 it is common opinion, as also recently reported by Bishop et al, 38 that NSCLC-NOS co-expressing TTF-1 and p63 should be considered as being poorly differentiated adenocarcinomas.
In the group of promising biomarkers to subtype NSCLC, napsin-A for adenocarcinoma75-78 and p40 and desmocollin-3 for squamous cell carcinoma have been recently proposed.55,56,59,79-81 Of note, napsin-A seem to be never expressed in squamous cell carcinoma and have higher sensitivity than TTF-1 in poorly differentiated adenocarcinoma. Desmocollin-3 has been recently proposed by Monica et al 82 on a series of large cell carcinomas, which appears to have high specificity rate for squamous cell carcinoma. Desmocollin-3 was never expressed in adenocarcinoma and neuroendocrine tumors and was mutually exclusive with TTF-1.81,82
Despite a limited number of studies, p40 (an antibody reacting only with truncated dominant-negative isoforms of p63 gene, also named as deltaN-p63) seems to have an higher specificity than conventional transactivated p63 in distinguishing squamous cell carcinoma, and p63-positive adenocarcinomas turned-out negative when using p40.64-67 Pelosi et al 66 and Bishop et al 67 robustly demonstrated that p40 may be considered equivalent to p63 in terms of sensitivity for squamous cell carcinoma, but it is significantly superior in terms of specificity, since only rare adenocarcinomas may show p40 labeling in no more than 5% of tumor cells if compared with p63 (3% vs 31%, respectively). 67 Therefore, we have recently recommended that p40 may stably enter the diagnostic repertoire of every pathologist to pave the way to a driver, holistic, biomarker approach to lung cancer characterization for clinical purposes, where a p40-based scoring system sharply separated adenocarcinoma from squamous carcinoma according to the axiom “no p40, no squamous.” 81 At variance with TTF1, however, p40 was diagnostically powerful and meaningful when looking at either positive or negative profiles, whereas TTF1 was diagnostically useful especially if positive, since whenever negative in the setting of poorly differentiated tumors could underline diverse tumor subtypes, such as squamous cell carcinoma, adenocarcinoma, adenosquamous carcinoma, sarcomatoid carcinoma, and even salivary gland–type tumors.66,81
Finally, an old and apparently useless marker, namely vimentin, has recently been reappraised for diagnosing challenging NSCLC subtypes, such as sarcomatoid carcinoma, more reliably, even on small biopsy samples, whether a strong and diffuse cytoplasmic immunoreactivity was seen in most tumor cells.44,82
Nuclear markers are more reliably and easily interpretable than cytoplasmic markers especially when dealing with limited diagnostic material, crush artifacts, and passive diffusion of cytoplasmic proteins. Although mixing diverse biomarkers, whether nuclear or cytoplasmic, into different antibody cocktails (eg, TTF-1/desmocollin-3, p63/napsin-A, or p40/TTF-1) could be an adequate answer in term of sensitivity and specificity of reaction to get valuable diagnostic results,33,59 these combinations however need further evaluation.
The distribution of the main markers thus far proposed for lung cancer subtyping and the relevant combinations aimed at addressing the main differential diagnoses are shown in Tables 1 and 2, respectively. Representative pictures featuring diagnostic profiles according to TTF-1, napsin-A, p63, and chromogranin immunoreactivity are shown in Figure 1.
Distribution of Immunomarker Expression Along the 3 Main Cell Differentiation Lineages of Epithelial Lung Tumors.
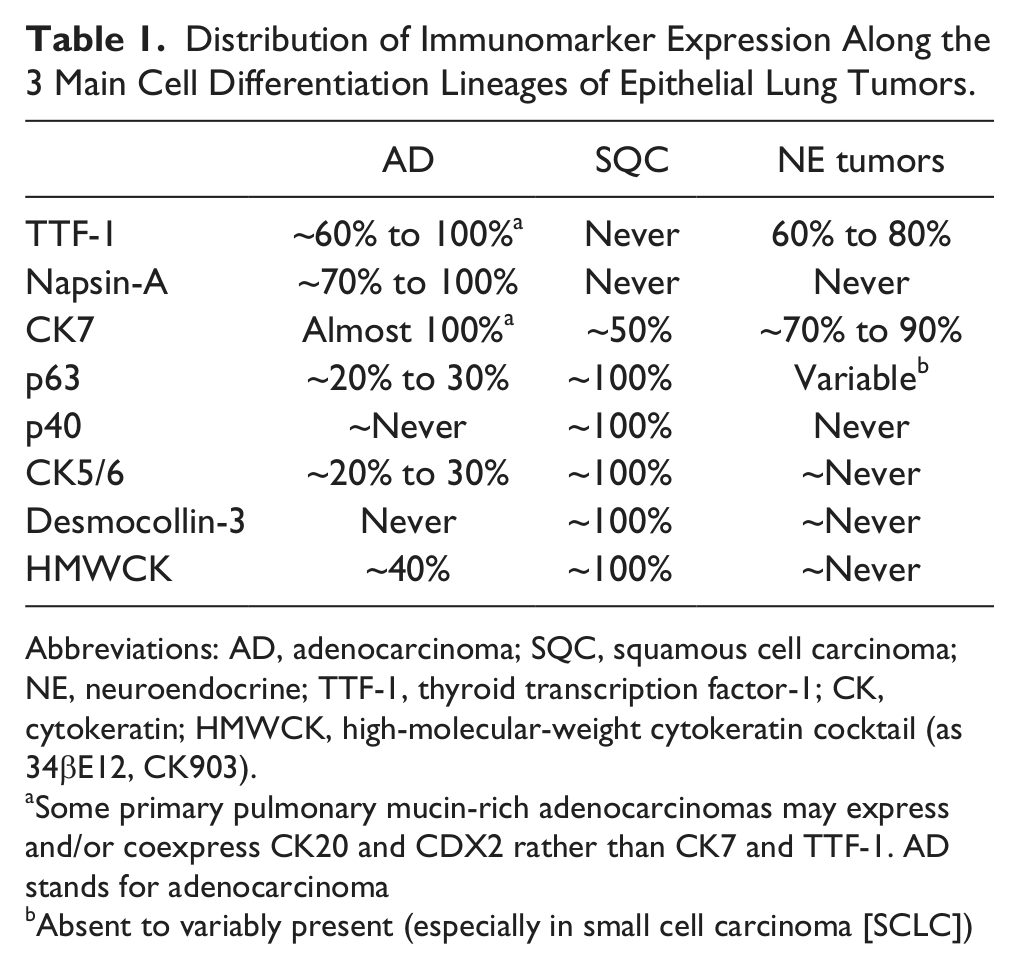
Abbreviations: AD, adenocarcinoma; SQC, squamous cell carcinoma; NE, neuroendocrine; TTF-1, thyroid transcription factor-1; CK, cytokeratin; HMWCK, high-molecular-weight cytokeratin cocktail (as 34βE12, CK903).
Some primary pulmonary mucin-rich adenocarcinomas may express and/or coexpress CK20 and CDX2 rather than CK7 and TTF-1. AD stands for adenocarcinoma
Absent to variably present (especially in small cell carcinoma [SCLC])
Immunostains in the Most Common Differential Diagnoses of Lung Cancer a .
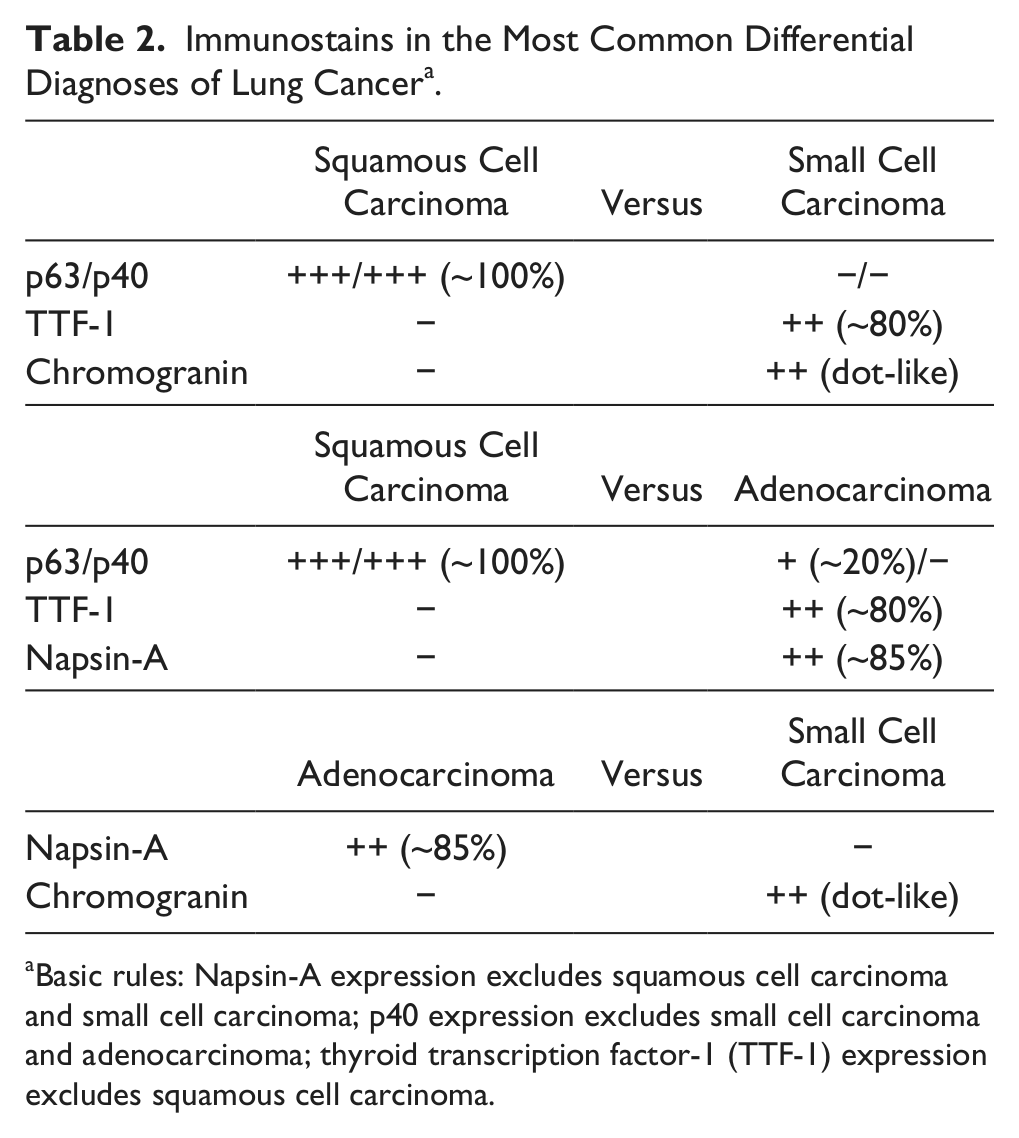
Basic rules: Napsin-A expression excludes squamous cell carcinoma and small cell carcinoma; p40 expression excludes small cell carcinoma and adenocarcinoma; thyroid transcription factor-1 (TTF-1) expression excludes squamous cell carcinoma.
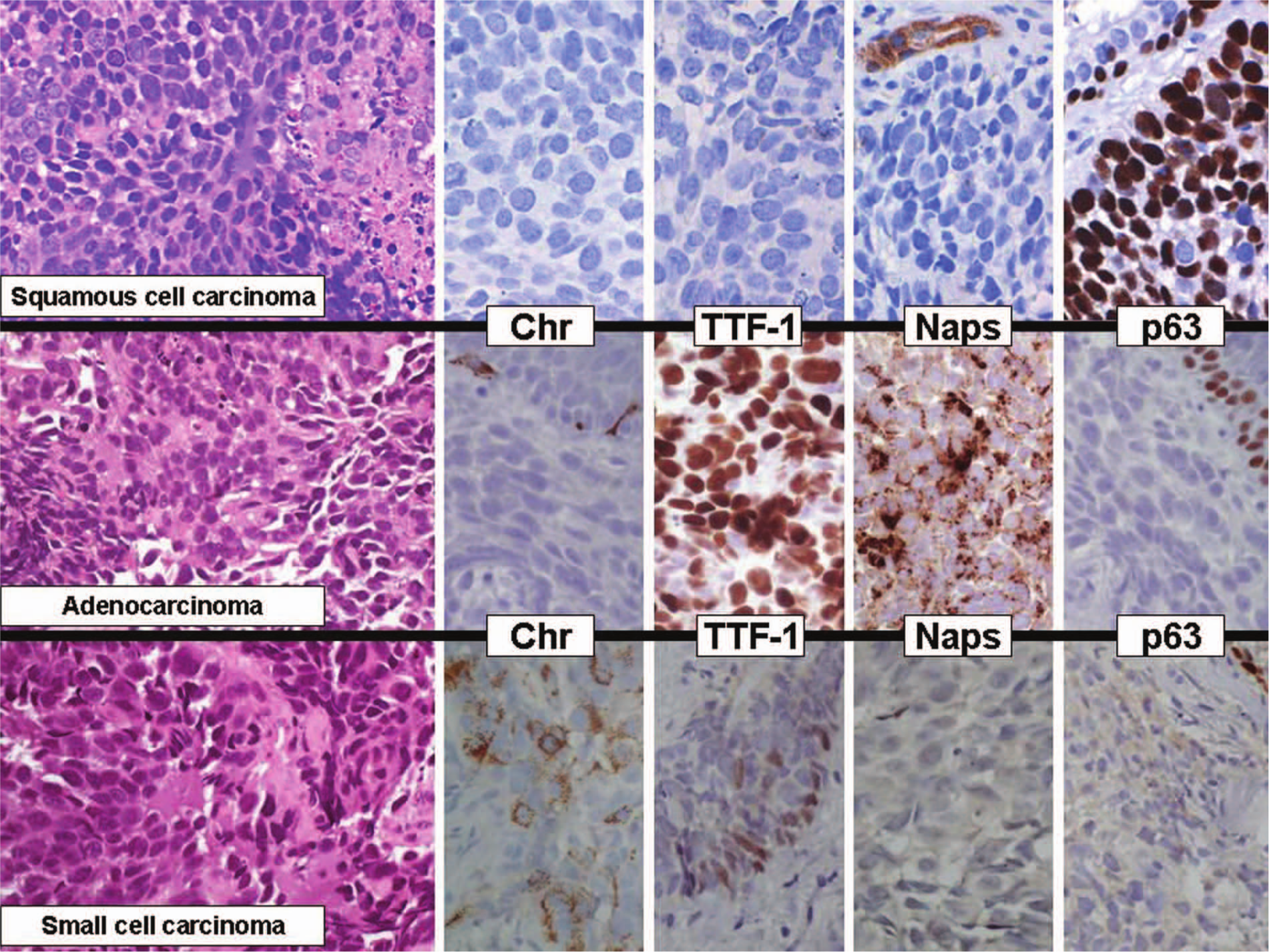
The distribution of chromogranin (Chr), thyroid transcription factor-1 (TTF-1), napsin-A (Naps), and p63 immunoreactivity is shown as a function of the 3 main subtypes of lung cancer, namely, squamous cell carcinoma (Chr−/TTF-1−/Naps−/p63+), adenocarcinoma (Chr−/TTF-1+/Naps+/p63±), and small cell carcinoma (Chr±/TTF-1+/Naps−/p63−).
Relevant points to immunohistochemistry: A limited use of IHC markers is recommended for NSCLC-NOS to subtype. The best single marker for adenocarcinoma is TTF-1 and the best single marker for squamous cell carcinoma is p40, realizing a 2-hit, sparing material algorithm suitable for both cytology and small biopsy specimens.
Be Aware of Antibodies Clones and Other Technical Issues
When using immunohistochemistry for NSCLC subtyping, pathologists should be aware of some technical tricks that can cause discordant or ambiguous results to occur. In particular, Matoso et al 83 evidenced that some commercially available antibodies recognizing TTF-1 may show different results. The monoclonal antibody 8G7G3/1 seems to be more specific than the clone SPT24, this latter staining several pulmonary non–small cell carcinomas of all histotypes. By contrast, the majority of published works revealed that the monoclonal antibody 8G7G3/1 is quite specific for adenocarcinoma and neuroendocrine tumors, whereas squamous cell carcinomas are negative. Some caveats should be taken into account when using TTF-1, since different papers have observed a consistent expression also in nonpulmonary adenocarcinomas, mainly from the gynecologic tract (particularly from endometrium) and breast.84,85 Another important concern is the dilution at which TTF-1 antibody is employed. In our own experience it is preferable to adopt a dilution higher than 1:500, since immunostaining is well maintained preventing nonspecific results, such as cytoplasmic positivity or background staining (Pelosi G, personal observation).
Two recent works by Ordonez86,87 have consistently demonstrated that squamous cell carcinomas of the lung do not exhibit napsin-A and TTF-1 positivity. Of note, the same author underlines the need to be aware when evaluating reactivity of napsin-A and TTF-1, since some apparent discrepant results in squamous cell carcinoma are related to an erroneous interpretation of the strong expression of these markers in tumor-entrapped hyperplastic type II pneumocytes. The strong reactivity of napsin-A in intra-alveolar macrophages should also alert, particularly in small biopsies, cytology, or even tissue microarrays.86,87 Also, it is important to note that monoclonal napsin-A is less sensitive, but more specific than polyclonal napsin-A antiserum, whenever this antibody is used in discriminating lung origin of adenocarcinomas. 75
Currently, the single best marker of squamous cell carcinoma is a polyclonal rabbit antiserum against p40,62,63 which works well in paraffin sections with strong specific nuclear decoration and no significant background staining if the antibody is particularly diluted (at least 1:2000/1:3000), made react with short incubation and developed with a highly sensitive detection system to avoid unspecific cytoplasmic background or inconsistent nuclear decoration.44,66,81 Worth noting is that nonneoplastic lung tissue always is devoid of p40 nuclear staining apart from the basal cell layer of the bronchial epithelium, with no specific nuclear staining in type II pneumocytes unlike p63.66,81
Relevant points to technical issues: The accurate choice of the reagent types and the staining procedures are particularly crucial in the IHC characterization of lung cancer because false results of staining, whether positive or negative, may seriously affect the obtaining of reliable final results.
Immunohistochemistry Versus miRNA
MicroRNA (miRNA) are short noncoding genes playing a regulatory role in gene expression. These biomarkers are essential in tissue differentiation and some miRNA are tissue specific. 35 Lebanony et al 36 recently demonstrated that expression of miRNA-205 by quantitative real-time polymerase chain reaction on formalin-fixed, paraffin-embedded samples of NSCLC were significantly higher in squamous cell carcinomas than in adenocarcinomas, reaching a sensitivity of 96% and specificity of 90%. Similar results were subsequently observed by Del Vescovo et al 37 and Bishop et al 38 confirming high sensitivity and specificity of miRNA levels in distinguishing squamous cell carcinoma from adenocarcinoma, even if with a few notes of caution. 88 In fact, miRNA-205 expression parallel results obtained by conventional morphology and/or immunohistochemistry. Considering the high cost and the laboratory equipment required for miRNA-205 determinations, the expression of miRNAs represents an accurate diagnostic adjunct rather than a true improvement over more conventional characterization of NSCLC. 89
Relevant points to miRNA assessment: Although miRNA assessment is appealing in lung cancer for its biological implications, morphology and a limited number of IHC markers still remain the best choice to efficiently subtype NSCLC.
Practical Hints for Surgical Pathologists
As recently underlined by the IASLC/ATS/ERS recommendations, knowledge of clinical data may be essential in lung cancer diagnosis, such as smoking habit, tumor location and escavation, imaging appearance or laboratory tests, and history of previous malignancies. 29 Pathologists should be aware that it is not infrequent to deal with primary lung adenocarcinomas that may express some markers commonly considered for extrapulmonary differentiation and vice versa, such as CDX-2 and enteric differentiation.90,91
Pathologists should always consider the possibility to share difficult cases with other colleagues and more expert pathologists. This is good practice behavior, since it does not cause delay in patient management and obviates the need for complicated diagnoses due to exaggerated IHC that not necessarily provide an advantage over routine light microscopy, according to the axiom “the more the immunostains, the more complicated the diagnoses.”
Pathologists should also consider that a minority of NSCLC (hopefully <5%) remains hard to be subtyped on cytology and small biopsies. In addition, it is paramount to put great consideration on proper tissue handling in order to optimize therapeutic strategies. Once morphology and a couple of immunostains have failed in NSCLC subtyping, remaining tumor cells should be tested for molecular analyses, in particular EGFR and ALK testing.
Of note, TTF-1 and p63 seem to represent the most widely used and tested panel of antibodies in NSCLC subtyping. Unfortunately, these markers are not completely mutually exclusive and ambiguous results showing double positivity or negativity or other combinations (ie, focal p63 positivity in absence of TTF-1 staining) may occur. On the premise that we are still waiting for perfect immunomarkers, if any, the adoption of some basic and easy-to-use rules are necessary and quite helpful when approaching TTF-1 and p63 to discriminate adenocarcinoma from squamous cell carcinoma (Figure 2).
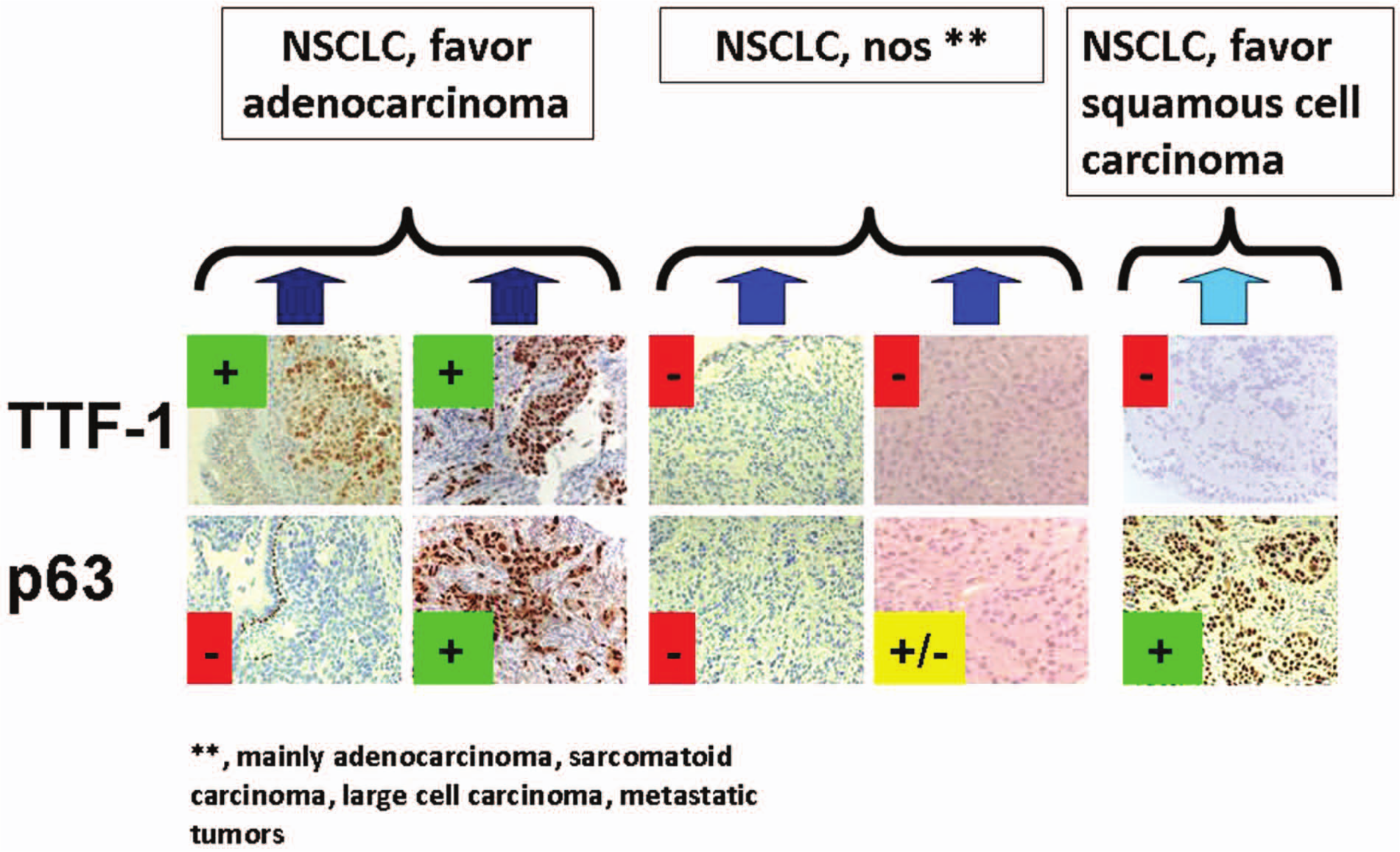
The diagnostic categories resulting from non–small cell lung cancer, not otherwise specified (NSCLC-NOS) after typing by immunohistochemistry according to thyroid transcription factor-1 (TTF-1) and p63 are shown: NSCLC, favor adenocarcinoma (TTF-1+/p63±), NSCLC, favor squamous cell carcinoma (TTF-1−/p63+), and NSCLC-NOS (TTF-1−/p63±), the latter profile including poorly differentiated adenocarcinoma, sarcomatoid carcinoma, neuroendocrine (NE) tumors, large cell carcinoma (only on surgical specimens), or metastatic tumors.
Basically, all poorly differentiated NSCLC (or alternatively, NSCLC-NOS) with some TTF-1 positivity should be equated to poorly differentiated adenocarcinomas whatever results are observed with p63. NSCLC showing double negativity or only focal immunostaining for p63 in absence of TTF-1 should be considered as poorly differentiated nonsquamous cell carcinomas, keeping in mind that this immunophenotype can characterize poorly differentiated adenocarcinoma, sarcomatoid carcinomas, NE tumors and even metastatic tumors to the lungs. Poorly differentiated squamous cell carcinomas are instead evidenced by strong and diffuse p63 expression and TTF-1 negativity, hence negativity for p63 exclude by definition this tumor type. Nevertheless, napsin-A for adenocarcinoma and p40, CK5/6 or desmocollin-3 for squamous cell carcinoma seem to represent further alternatives, even though the reason for using minimal stains is to spare tissue for molecular studies. To this regard, the doublet TTF-1 and p40 is currently deemed the best combination for typing NSCLC in every type of material (Figure 3).27,66,80
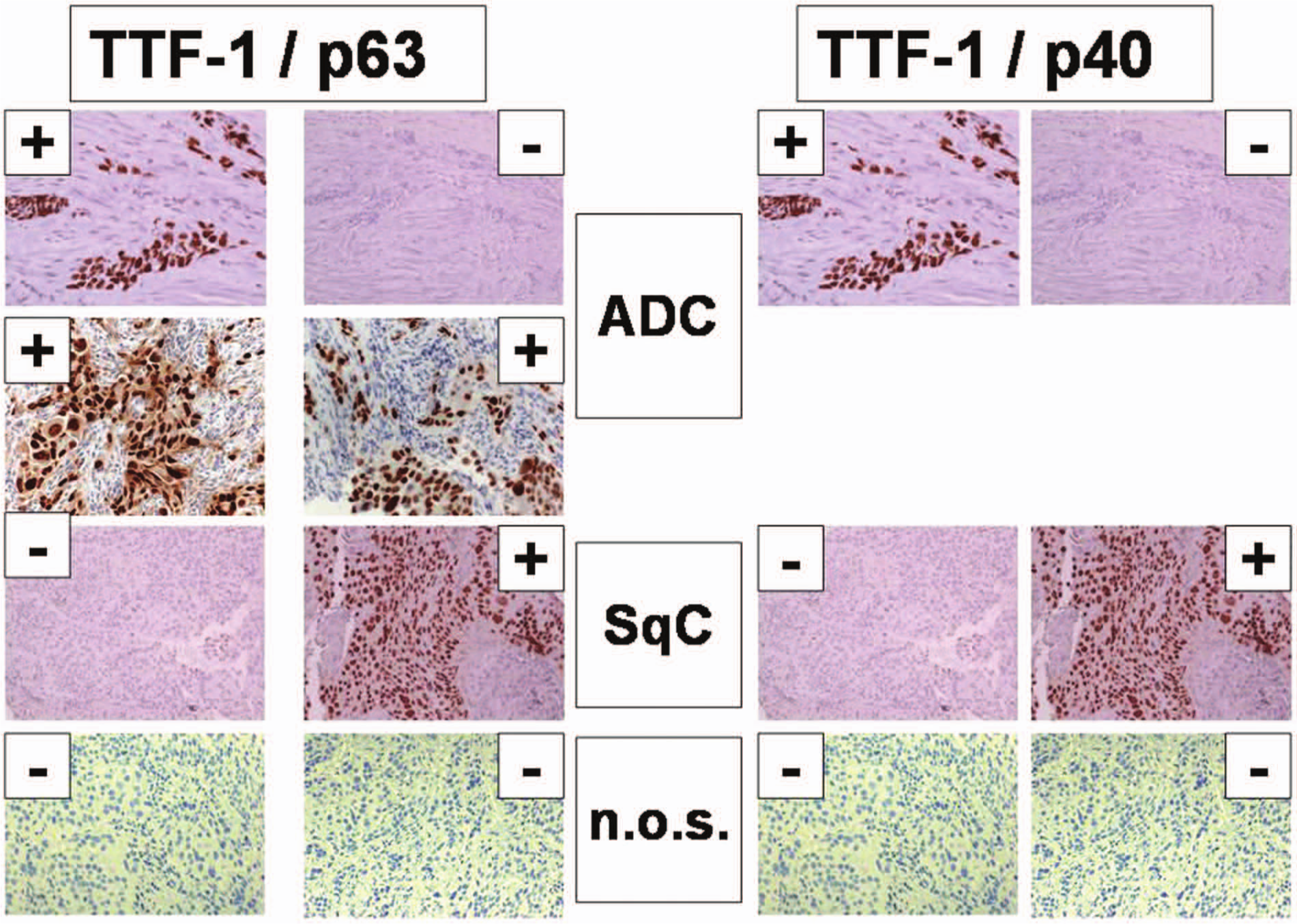
A comparison between p63 and p40 as identifiers of adenocarcinoma (TTF-1±/p63±/p40−), squamous cell carcinoma (TTF-1−/p63+/p40+), and NSCLC-NOS (TTF1−/p63±/p40−) is shown.
Relevant points to surgical pathologists: A multidisciplinary approach also including imaging and clinical information has been recommended applying to the diagnosis-making process of lung cancer especially in cytology and small sized biopsy specimens, as well as using a minimalist approach by mean a couple of well-defined and specific biomarkers (eg, TTF-1 and p40) whenever light microscope or mucin stain fails to give ultimate answers.
Conclusive Remarks for the Best Pathology Practice
Diagnosis of lung cancer, according to the recent IASLC/ATS/ERS recommendations, is often a complex puzzle requiring step-wise integration of clinical and radiologic data with pathologic features (morphology and immunohistochemistry).
NSCLC subtyping is a key point in tailoring novel treatments and guiding molecular investigations. Such a diagnosis can be performed on morphology in about 2/3 of NSCLC, but 30% of NSCLC require ancillary techniques (basically immunohistochemistry) because of scarce material, artifacts, or poor differentiation.
TTF-1 plus p40 is the best panel to limit the need for further immunostains and preserving tissue for molecular tests. Napsin-A for adenocarcinoma and CK5/6 and desmocollin-3 for squamous cell carcinoma are the best choices if further stains are necessary. Other markers (CK7, SOX2, clone 34βE12) seem to be nonspecific.
Finally, in case of a clear-cut morphology, IHC should be used only to exclude metastatic extrapulmonary adenocarcinoma. In general, the more stains you demand the more complicated become the case, considering that some overt pulmonary adenocarcinomas may express puzzling combinations of diverse markers. Suffice it to say that TTF-1 is the “queen” and p40 is the “king” when operatively used according to appropriate diagnostic algorithms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.