
Abstract
Tailgut cysts, also known as retrorectal cystic hamartomas, are congenital lesions derived by an abnormal remnant of the postanal primitive hindgut, consisting of unilocular or multilocular cysts usually lined by squamous, transitional, or glandular epithelium. Malignant transformation is an uncommon event, and it mainly involves the neuroendocrine or glandular epithelium; other histotypes are sporadic. Here, we report, for the first time, the clinicopathological features of a transitional cell carcinoma that arose in a tailgut cyst.
Introduction
Tailgut cysts are a rare congenital malformations arising from the embryonic hindgut. 1 In the course of normal development, the embryo forms a true tail, which exists, approximately, from the 35th through the 56th day of gestation. This tail contains the distal portion of the primitive hindgut, constituting the tailgut or postanal gut that extends beyond the point at which the anus develops. 2 As the embryonic tail and its contained tailgut normally regress by the 56th day of gestation, it is hypothesized that vestiges of the tailgut may remain and results in formation of a tailgut cyst, or retrorectal cystic hamartoma, in the retrorectal/presacral space. This is a virtual space bounded anteriorly by the rectum, posteriorly by the sacrum, superiorly by the peritoneal reflection at the S2-S3 level, inferiorly by the levator ani and coccygeus muscles, and laterally by the lateral rectal ligaments, ureters, and iliac vessels.1,2
Tailgut cysts usually present in adult life, even if some cases have been also described in infants.1,3,4 The reason why these lesions occur more commonly in females (between 75% and 90% of cases) is still unclear. 2 Clinically, the tailgut cyst appears as a well-defined palpable mass during digital rectal examination. Imaging studies reveal a uniloculated or multiloculated cyst in the retrorectal/presacral area. 2 Grossly, the lesion is soft, well-circumscribed when the surgical excision preserves the integrity of the cyst, usually composed of multilocular cysts ranging in size from 1 cm to 15 cm (average diameter 3.9 cm) and having a clear to thick mucoid or opaque greenish yellow fluid.2,5 Histologically, a wide range of lining epithelia may be present, such as squamous, columnar, cuboidal, ciliated columnar, mucinous, gastric, and transitional.5,6 Scattered bundles of smooth muscle fibers are invariably present in the wall, separated from the lining by a thin layer of fibrous tissue. These characteristics are very important to distinguish the tailgut cysts from other lesions.
Here we describe a case of transitional cell carcinoma arisen in a tailgut cyst of the presacral space and a review of pertinent literature.
Clinical Data
A 68-year-old woman, with a 3-month history of persisting diarrhea, pelvic pain, and hematochezia, was admitted to our hospital with an abdominal ultrasound diagnosis of a pelvic mass. Physiological examination on admission did not reveal any unusual signs. CA19-9 and CEA dosage were negative. Computed tomography scan revealed a mass located in the posterior pelvis, involving the entire retrorectal space, surrounding and compressing the rectum (Figure 1A). A complete colonoscopy was performed and documented a compression of the posterior medium and low rectum, with ulceration of the rectal wall (Figure 1B).
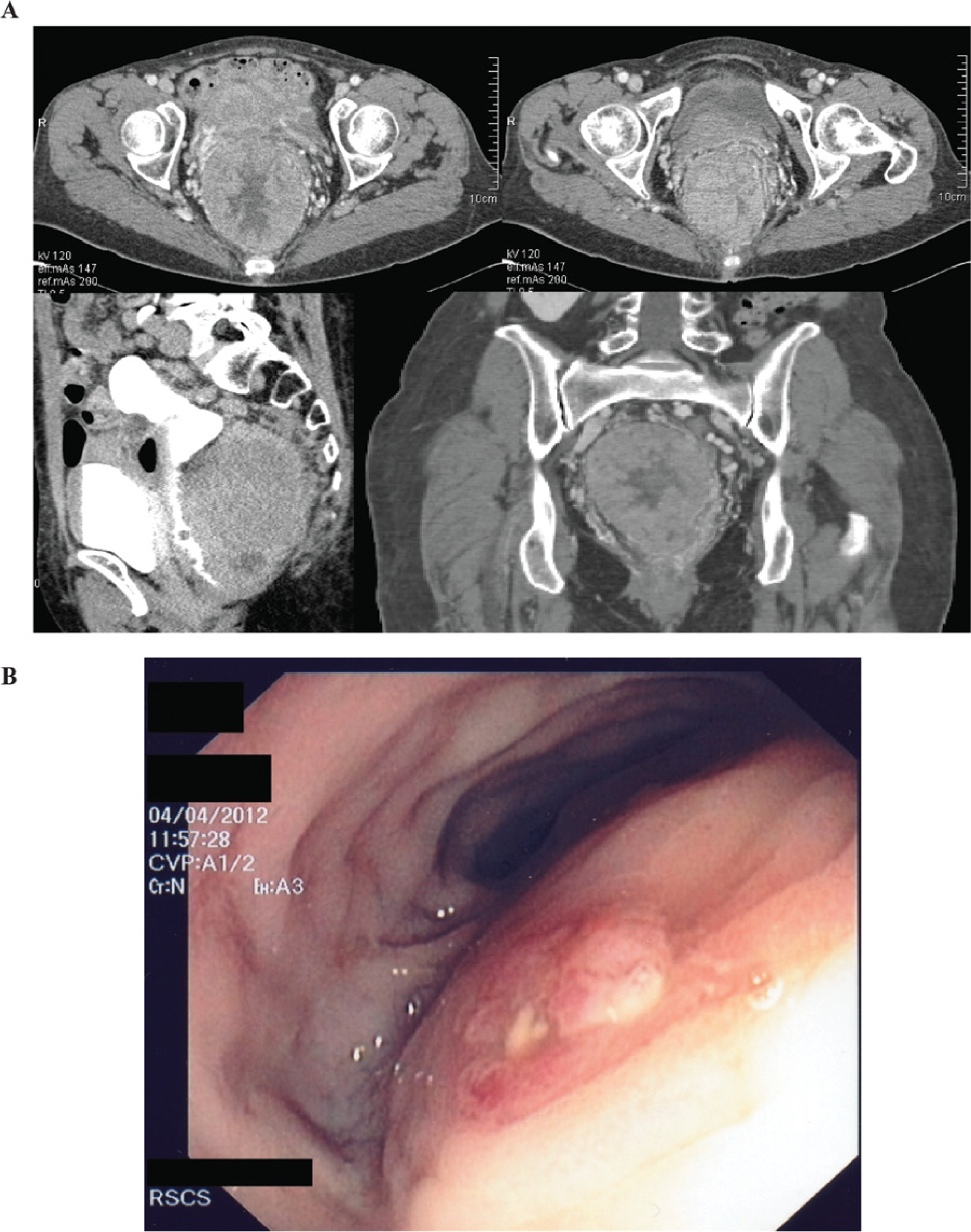
A, Computed tomography showing the pelvic retrorectal and presacral mass. B, Colonoscopy showing the rectal posterior compression and the rectal ulceration.
Pathologic Features
Transanal and transrectal biopsies of the mass were performed and revealed fragments of transitional carcinoma (Figure 2A and B). Immunohistochemical analysis showed positivity of the neoplastic cells for CK-7 and negativity for CK-20, TTF-1, P63, and PAX-8 (Figure 2C and D).
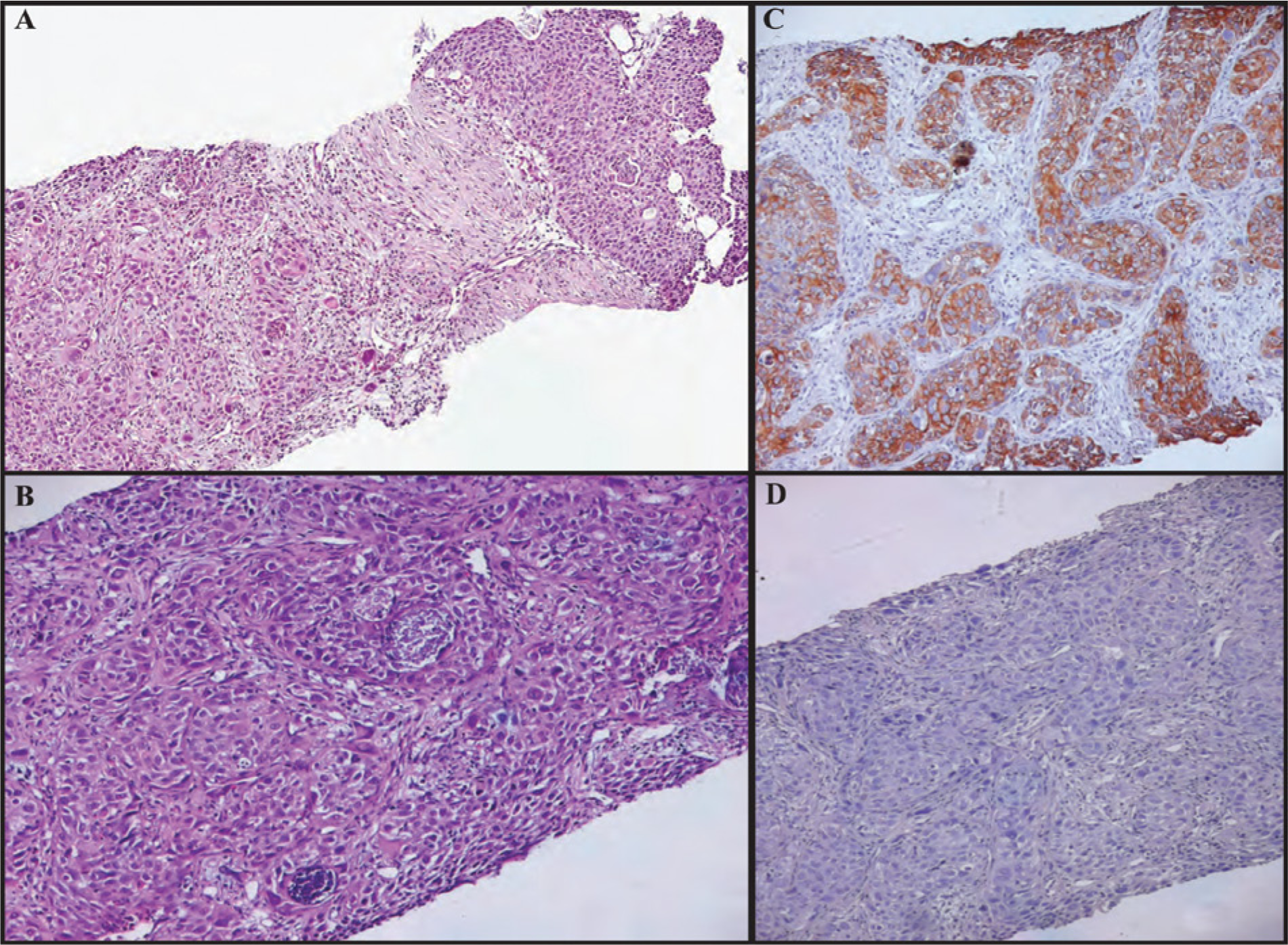
A, Biopsy of the mass revealing a transitional carcinoma (100×). B. Same as in A at higher magnification (200×). Hematoxylin/eosin staining is shown. C, Immunohistochemical analysis showing positivity of the neoplastic cells for CK7, and D, negativity for CK20.
In accordance with the oncologist and the patient, we decided to perform an abdominal exploration. At laparotomy no endoperitoneal lesions were identified, and the solid organs exploration was negative. The pelvic mass was identified on the para- and mesorectal space, located on the presacral space. A low anterior rectal resection with total mesorectal excision followed by loop ileostomy and bilateral hysteroannessectomy were performed.
On gross examination, the surgical specimen was composed of a large bowel segment of 11 cm in adherence with an apparently well-capsulated mass of 18 × 14 cm. Opening the large bowel, a mucosal ulceration was observed in continuity with the external mass. On the cutting surface the mass appeared as a unilocular cyst, and the internal surface was hemorrhagic with a papillary appearance. No obvious necrosis was present.
Microscopically, the mass consisted of a cyst lined by transitional epithelium with both papillary and flat architecture with severe atypia, from which developed a poorly differentiated transitional cells carcinoma (Figure 3A and B). The neoplasia penetrated the entire thickness of the cyst and infiltrated the colic wall ulcerating the mucosal layer (Figure 3C).
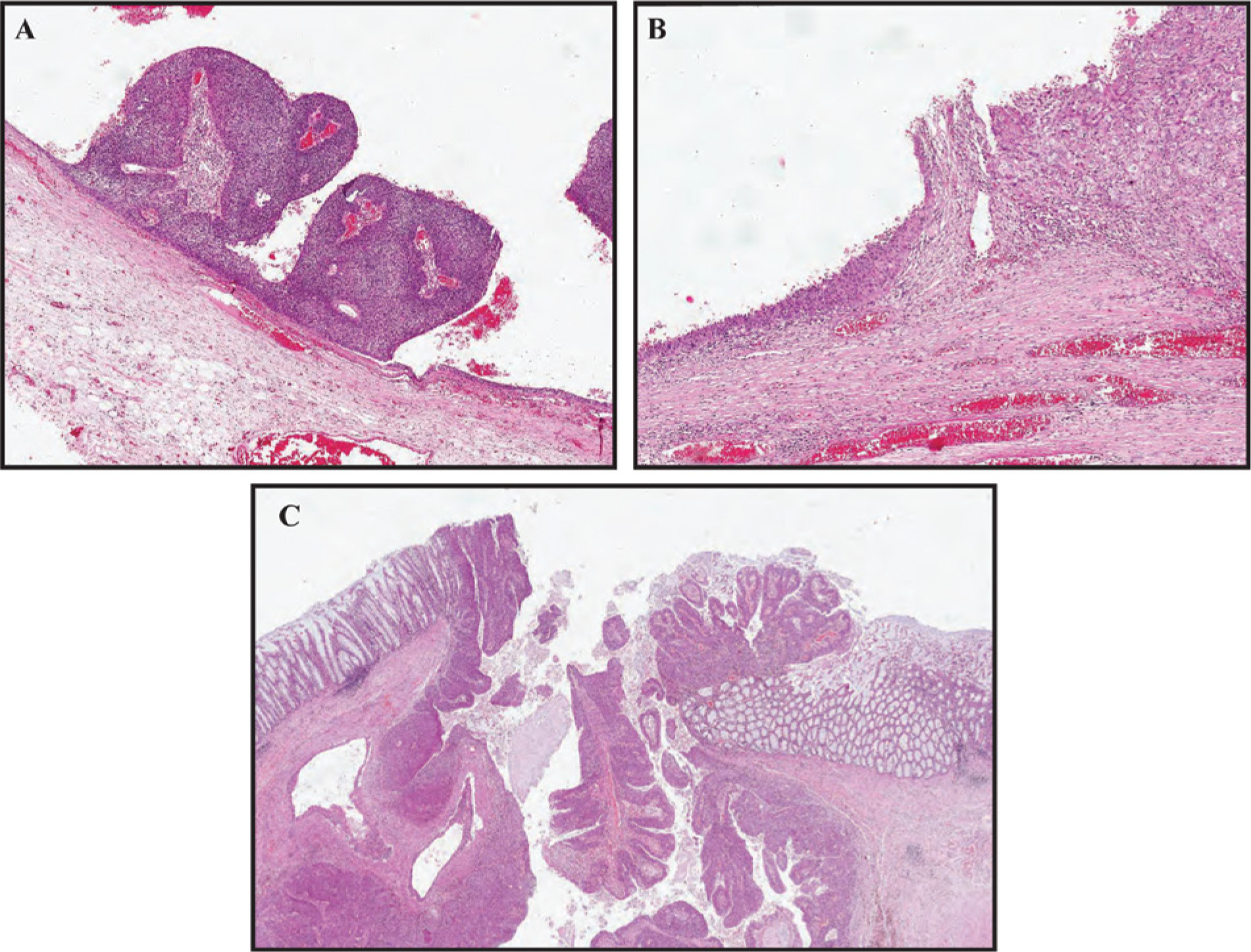
A and B, Hematoxylin/eosin staining (100×) showing the cyst wall lined by transitional epithelium with both papillary and flat architecture with severe atypia, from which developed an invasive carcinoma (B, right corner). C, Hematoxylin/eosin staining (100×) showing ab estrinseco infiltration of the colic wall and mucosae.
The macroscopical and microscopical examination of the hysteroannessectomy specimen did not reveal any pathological alterations, excluding a possible origin of the neoplasia from the Walthard’s cell rest.
The postoperative course was complicated by a urinary retention treated with urinary catheterization and spontaneously resolved. The patient was discharged on the 15th postoperative day.
Discussion
Tailgut cysts, also known as retrorectal cyst hamartomas, are rare congenital abnormalities and are thought to derive by the postanal gut. 5
Almost half of the patients presenting a tailgut cyst remain asymptomatic, and the cysts are usually diagnosed only as an incidental finding during routine examinations; the remaining patients generally present low back pain or symptoms due to a mass effect. 7 Malignant change is an extremely rare complication; in fact, an extensive search of the literature showed that malignant transformation mainly occurred in cyst lined by either neuroendocrine or glandular tissue and sporadically other histotypes.5,7-12
In the largest series reported of 53 patients with tailgut cyst, only a single case of a transformation in poorly differentiated adenocarcinoma was described. 5
Recently, Tampi and colleagues found 16 cases of tailgut cysts with transformation in adenocarcinomas. 8 Occasionally, some authors have reported other histotypes, including endometrioid carcinoma, adenosquamous carcinoma, squamous cell carcinoma, and sarcoma.10,13
Frequently, these cases were initially misdiagnosed. Pathologists had to distinguish between tailgut cyst and other more common pathological entities, such as teratomas, epidermoid, dermoid, and rectal duplication cysts. 12
For these reasons, histological diagnostic criteria were established to distinguish between tailgut cyst and all the other lesions.
A rectal duplication cyst is composed of an intestinal mucosa in which cells are arranged to form villi and crypts and a well-defined muscular layer, often with a myoenteric plexus, that surrounds the cavity. In a tailgut cyst coexist different types of epithelia, and the smooth muscle fibers are haphazardly scattered. Also dermoid cysts, which are formed by stratified squamous epithelium with skin adenxa, and epidermoid cysts, which are formed by stratified epithelium only, do not have the wide range of epithelia that normally may be appreciated in tailgut cysts.5,12,15
The differences between teratomas and tailgut cysts involve also epidemiologic aspects, taking into account that tailgut cysts occur mostly in middle-aged women and teratomas are more frequent in neonates. Moreover, teratomas frequently demonstrate intralesional calcifications, fat, and bony destruction of coccyx or sacrum, features that are usually absent in tailgut cysts. The main criterion to distinguish those lesions is the presence in teratomas of cells originating from all 3 germ cell layers, endoderm, mesoderm, and ectoderm, that are absent in tailgut cysts.1,3,5 Despite these criteria, distinguishing between teratoma and tailgut cyst may be challenging. In fact, some authors have described few cases of teratomas occurring in adult females 15 and tailgut cysts occurring in infants. 4 Moreover, a case of tailgut cyst with meningothelial proliferation and thyroid tissue induced the authors to hypothesize the absence of a strict distinction between these 2 pathological entities. 2
For the first time, we described a transitional cell carcinoma associated with tailgut cyst.
Taking into account the rarity of the association that we describe, the tailgut cyst malignant transformation could be misdiagnosed not only with lesions that represent the classical differential diagnosis but also with a transitional cell carcinoma arisen in the ureters that bound laterally the presacral space or even with an ovarian Brenner’s tumor. Moreover, it can be very challenging to distinguish between a transitional cell carcinoma, which arises in a tailgut cyst, and one deriving from the urinary tracts, especially if we consider that perirenal tailgut cysts have been already described in literature.16,17
Preoperative imaging along with biopsies of the lesion can be helpful to hypothesize the diagnosis of tailgut cyst, but the diagnostic gold standard is still histological gross examination. In our case, the examination of the uterus and its adnexa permitted to exclude a Brenner’s tumor; the presence of transitional cell carcinoma in situ lining the cyst cavity in continuity with the transitional cell carcinoma was crucial to confirm the origin of the neoplasia.
Our work and those of others suggest that patients with suspected presacral tailgut cyst should be offered surgery when the lesion is identified because of the risk of malignant transformation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was partially supported by a grant from Associazione Italiana per la ricercasulcancro (AIRC IG 11561 to AV).