
Abstract
Background. Mesenchymal colorectal polyps are uncommon lesions, particularly those of neurogenic origin. We describe a mucosal Schwann cell hamartoma of the colon with tactoid features, so far reported in peripheral nerve sheath tumours, and address its differential diagnosis and clinical implications. Case presentation. A 72-year-old man underwent screening colonoscopy that presented a 5-mm polyp on distal sigmoid. Histologically, it displayed a lesion in the lamina propria comprising oval structures with tactoid features and bland spindle cells, entrapping adjacent crypts. No ganglion cells were seen. Spindle cells expressed only S-100 protein and vimentin. Discussion. Mucosal Schwann cell hamartoma was recently recognized as distinct from common (submucosal) colorectal Schwannomas and so far not associated to inherited syndromes. Thus, it should be considered in the differential diagnosis of look-alike lesions (eg, ganglioneuroma, neuroma, and neurofibroma) that may occur in the setting of inherited syndromes such as Cowden syndrome, multiple endocrine neoplasia-2B, and type 1 neurofibromatosis.
Background
Colorectal polyps with a mesenchymal origin are uncommon lesions diagnosed in routine colorectal biopsy specimens. Many of these lesions are benign and some authors even group them together as benign unclassified mucosal polyps or BUMPs. 1 The differential diagnosis classically includes neoplasms of neural and smooth muscle origin, gastrointestinal stromal tumors (GISTs), and fibrous lesions. 2 Of these, the lesions presenting as small polyps and with neural origin are an even rarer group, many associated with inherited syndromes such as type 1 neurofibromatosis (NF-1) 3 and Cowden’s syndrome. 4 Other lesions in this group appear to occur in a sporadic setting not associated with any known syndrome. 5
Recently, in a series of colorectal polypoid lesions composed by Schwann cell proliferation, a new lesion named mucosal Schwann cell hamartoma was described. 5 This is a lesion that while composed of Schwann cells, is morphologically distinct from gastrointestinal (GI) Schwannoma namely because GI Schwannoma occur rarely in the colon and display intramural extension and distinctive peripheral lymphoid cuffs. 6
Mucosal Schwann cell hamartoma were described as Schwann cell proliferations, limited to the lamina propria, comprising uniform, bland spindle cells with elongated nuclei and abundant dense cytoplasm. 5 By immunohistochemistry, the cells express S-100 protein with very week and rare expression of neurofilaments, in the absence of glial fibrillary acidic protein (GFAP), CD34, smooth muscle actin, and KIT expression.5,7 So far, only 3 reports about this type of hamartoma have been published in the English literature.5,7,8
Here, we describe a case with morphological and immunohistochemical features of mucosal Schwann cell hamartoma, together with tactile corpuscle-like structures or tactoid bodies, so far reported in peripheral nerve sheath tumors such as Schwannoma, neurofibroma, 9 and neuroid intradermal melanocytic nevi. 10
Materials and Methods
A 72-year-old man underwent routine screening colonoscopy. The patient had no relevant medical history, that is, no history of previous colonic polyps and no family history of any inherited syndrome such as Cowden syndrome, NF-1, or multiple endocrine neoplasia-2B (MEN-2B). The endoscopic examination revealed a 5-mm polypoid lesion in distal sigmoid mucosa (Figure 1), which was biopsied.

Endoscopic appearance of distal colon sigmoid.
Results
On hematoxylin and eosin examination, the lamina propria disclosed multiple small round to oval structures, well-delimitated and composed of uniform and bland spindle cells with indistinct cell borders (Figure 2A). The cytoplasm was dense and eosinophilic. The nuclei contained fine chromatin and occasional inconspicuous nucleoli (Figure 2B). The colonic epithelium displayed some glandular hyperplasia, without ulceration or dysplasia.
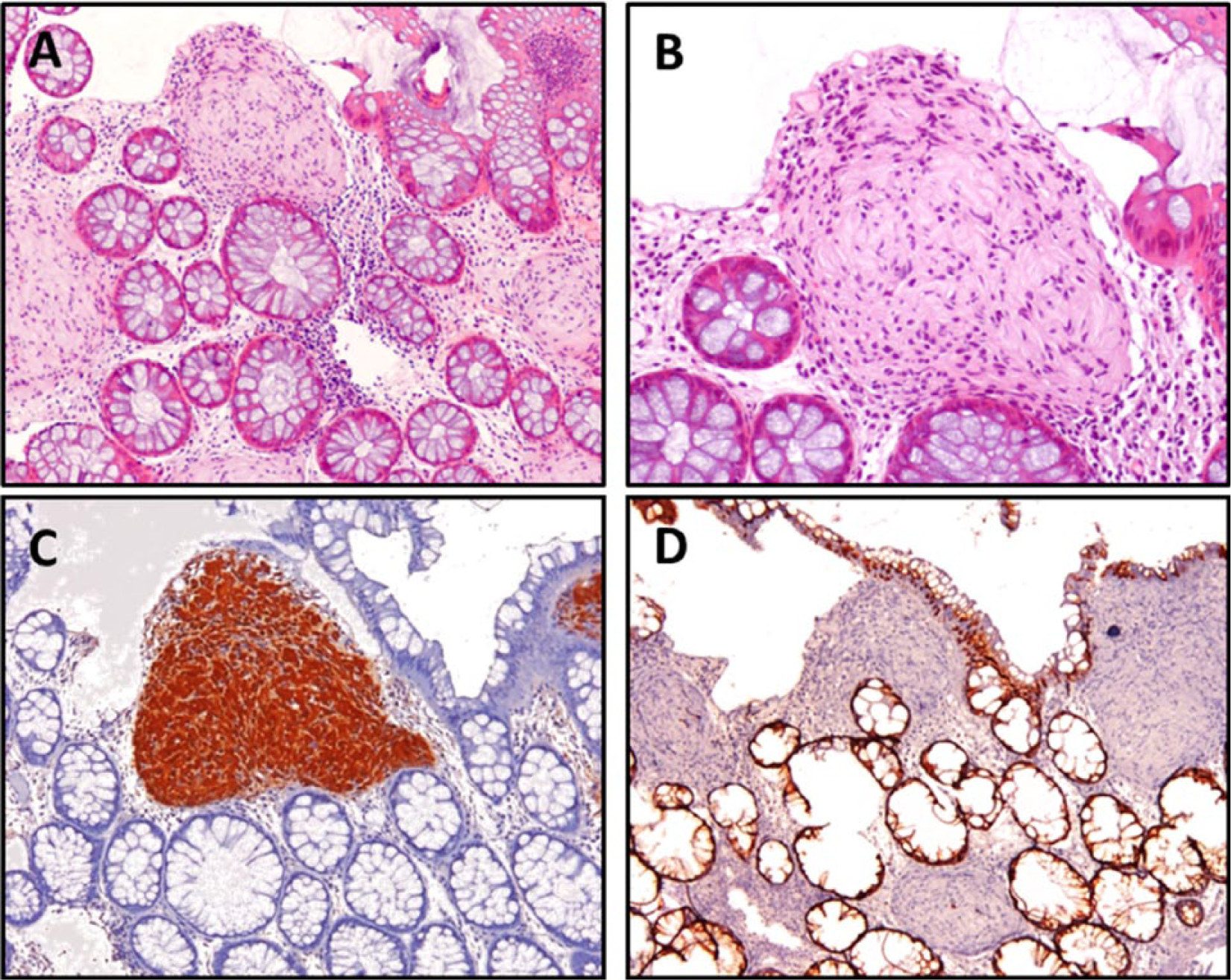
Histological features of colonic mucosa with diffuse Schwann cell proliferation within the lamina propria. Spindle cells with elongated nuclei, without cytological atypia, display tactoid body features; low-power magnification, hematoxylin and eosin (H&E) staining (A), high-power magnification, H&E (B); spindle cells expression of S-100 protein (C) in the absence of epithelial membrane antigen (D).
By immunohistochemistry, there was strong and diffuse expression of S-100 protein in the spindle cells (Figure 2C), without expression of any of the other markers tested, namely epithelial membrane antigen (EMA), synaptophysin, CD117 (KIT), and smooth muscle actin (Figure 2D).
Discussion
Tactile corpuscle-like structures or tactoid bodies are lamellate structures almost exclusively associated with specific types of nerve sheath tumors and intradermal nevi. 9 To our knowledge, this is the first report of a mucosal Schwann cell hamartoma with tactoid bodies.
Of note, mucosal Schwann cell hamartoma with tactoid bodies is not at all a new described entity. Interestingly, there are 2 previous reported cases11,12 describing lesions that, according to Gibson and Hornick, 5 displayed morphological and immunohistochemical features consistent with mucosal Schwann cell hamartoma, very similar to our case; in fact, in both cases tactoid body features were observed.11,12 (Table 1). Moreover, surface caveolae of the cell processes and rudimentary intercellular junctions characteristic of tactoid bodies were observed in the ultrastructural study of both cases. The authors claim that tactoid bodies may represent visceral embryonic remnants of sensory system.11,12 In addition, in a report of 7 mucosal benign epithelioid nerve sheath tumours, all lesions displayed, to some extent, features similar to mucosal Schwann cell hamartoma, albeit none depicted tactile-like corpuscles or tactoid body features. 13
Descriptions of tactile-like corpuscles or tactoid body features in GI mucosa.
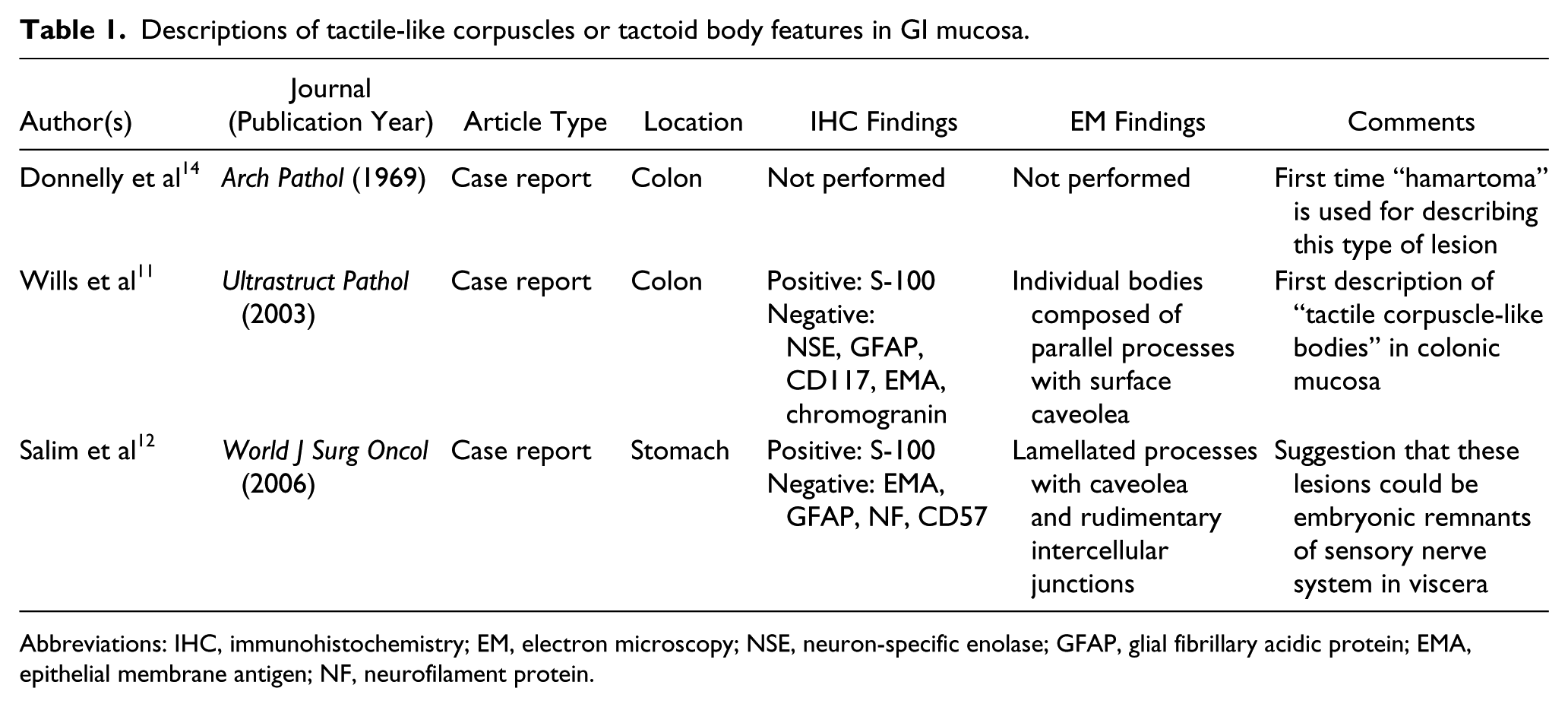
Abbreviations: IHC, immunohistochemistry; EM, electron microscopy; NSE, neuron-specific enolase; GFAP, glial fibrillary acidic protein; EMA, epithelial membrane antigen; NF, neurofilament protein.
Despite its characteristic features, the main concern for pathologists should be focused on the differential diagnosis between mucosal Schwann cell hamartoma and similar spindle cell proliferations of neural origin that may be associated with inherited syndromes, namely Cowden syndrome, MEN-2B or NF-1. 15 Remarkably, it seems from the available evidence in the literature that mucosal Schwann cell hamartoma does not associate with known inherited syndromes. Regarding ganglioneuromas, neurofibromas, and mucosal neuromas, their differential diagnosis is based on hematoxylin and eosin since these lesions usually display recognizable axons and/or ganglion cells. For the differential diagnosis with intramucosal perineuroma, an immunohistochemical study is usually necessary since this lesion is morphologically similar to mucosal cell Schwannoma, but its cells usually lack S-100 protein and express EMA, at variance with Schwann cells. 16
The diagnosis of GIST should always be considered because of its potential risk behavior. Different from mucosal Schwann cell hamartomas, GISTs are more frequent in the stomach and the small intestine and usually express C-Kit/CD117 and DOG-1.17,18
To conclude, here, we report a case of a mucosal Schwann cell hamartoma with tactoid bodies, a peculiar feature of a rare tumor that the pathologist should be aware of when dealing with polypoid spindle cell lesions in the colonic mucosa. Our report highlights tactoid body features in mucosal Schwann cell hamartoma that should not be misinterpreted as ganglioneuroma in small biopsies. Mucosal Schwann cell hamartoma diagnosis should be achieved with careful morphological and immunohistichemical assessment to avoid mislabeling the patient within the spectrum of mimicking lesions that may imply an inherited syndrome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Institute of Molecular Pathology and Immunology of Porto University (IPATIMUP) is an Associate Laboratory of the Portuguese Ministry of Science, Technology and Higher Education and is partially supported by Fundação para a Ciência e Tecnologia (FCT). Although this work did not receive any specific funding, by the time of publication of the manuscript, Francisco F. de Beca was supported by the FCT grant (HMSP-ICJ/0006/2012) and was affiliated with the Department of Medical Oncology, Dana-Farber Cancer Institute/Harvard Medical School., Boston, MA, USA.