
Abstract
In keeping with the stated goal of providing the surgical pathologist with tools to recognize abnormalities of the gastrointestinal (GI) tract due to drugs (AGIDS), in part II of this review we embark in a more organ-based description of AGIDS. Adequate space is given to the numerous adverse gastrointestinal effects of nonsteroidal anti-inflammatory drugs. Pill esophagitis, esophagitis dissecans, proton pump inhibitors’ effects, diaphragm disease, and the recently described effects of drugs such as olmesartan, mycophenolate, and of compounds such as yttrium-90 are highlighted among several others. The inclusion of drug effects in the differential diagnosis of “conventional” diseases (such as gastric antral vascular ectasia, graft-versus-host disease, ischemic colitis, acute colitis, collagenous enteritis, inflammatory bowel disease) is underscored to avoid sometimes significant diagnostic pitfalls. We reiterate the message of the necessary collaboration between pathologist and clinician in the recognition of these entities to provide the best patient care.
Keywords
Selected Drug-Induced Histological Effects in the Various Portions of the Gastrointestinal Tract
Esophagus
More than 100 drugs to date have been reported to cause esophageal injury (rather than listing these drugs, we refer to comprehensive reviews in the literature). 1 The medications most frequently linked to esophageal injury are antibiotics (in particular tetracyclines, especially doxycycline, and clindamycin), nonsteroidal anti-inflammatory drugs (NSAIDs), slow-release potassium, ferrous salts, and bisphosphonates.
The rapid transit of luminal contents through the esophagus is a defense mechanism to prevent direct and prolonged contact of the mucosa with a drug that may cause an acid-based or hyperosmolar burn. The protection provided by swift transport of esophageal contents is affected by stenosis (intrinsic to esophagus or extrinsic due, for example, to enlarged left atrium or postsurgical adhesions), disorders of motility (occasionally due to other drugs concomitantly taken such as anticholinergic agents), or concomitant pathologies (eosinophilic esophagitis, reflux, Parkinson’s disease, and scleroderma, for example, increase susceptibility to injury in the esophagus). Lack of sufficient water intake with pills and reclined position while taking the pill are associated with higher risk of esophageal injury. Women appear affected twice as often as men.
Symptoms of “pill” esophagitis include dysphagia, odynophagia, and retrosternal pain that resolve after cessation of the drug.
Endoscopic findings are erosions, ulcers, sloughed mucosa, and hemorrhages. The endoscopist will sometimes consider the ulcers worrisome enough to propose the diagnosis of carcinoma.
The ulcers can be multiple, confluent, and of various size, shape, and depth and are commonly found at the junction of upper third and middle third in correspondence to the aortic arch imprint on the esophagus. Death following esophageal perforation has been reported after use of NSAIDs, ferrous sulfate, and sodium valproate sustained release.
Endoscopy revealing pill fragments in an ulcer is considered diagnostic but the finding is uncommon. The inflammation is usually mild; spongiosis, necrosis of epithelium, and marked eosinophilic or occasionally neutrophilic intraepithelial inflammation can occur and evoke the differential diagnosis of reflux esophagitis and eosinophilic esophagitis. Lichen planus is a mimicker of drug-induced esophageal injuries and should be considered in the differential diagnosis. Esophageal lichen planus is the primary manifestation of the disease in 50% of the patients with esophageal involvement; lichen planus affects preferentially the proximal esophagus and can cause proximal stenosis. 2
Esophagitis dissecans superficialis (EDS; also known as sloughing esophagitis) is a dramatic endoscopic finding in patients complaining of dysphagia. EDS can be encountered in cases of bullous diseases affecting the esophagus or after chemical or thermal esophageal injury. EDS is defined by the presence of tubular or large epithelial casts sloughing off the wall of the squamous epithelium-lined esophagus, more often in the distal esophagus. The sloughed epithelium results from a split occurring at the same level above the basal layers of the epithelium. Sloughed epithelium may show yeasts or bacterial colonies. Hyperparakeratosis and necrosis of the sloughing squamous epithelium without associated inflammation is typical, sometimes seen associated with bullae and fluid-filled cysts in the underlying layers of epithelium. The underlying squamous epithelium can assume markedly reactive features or, on the other hand, be quite pale and with edematous swollen cells and impart a 2-toned appearance to the mucosa (Figure 1).
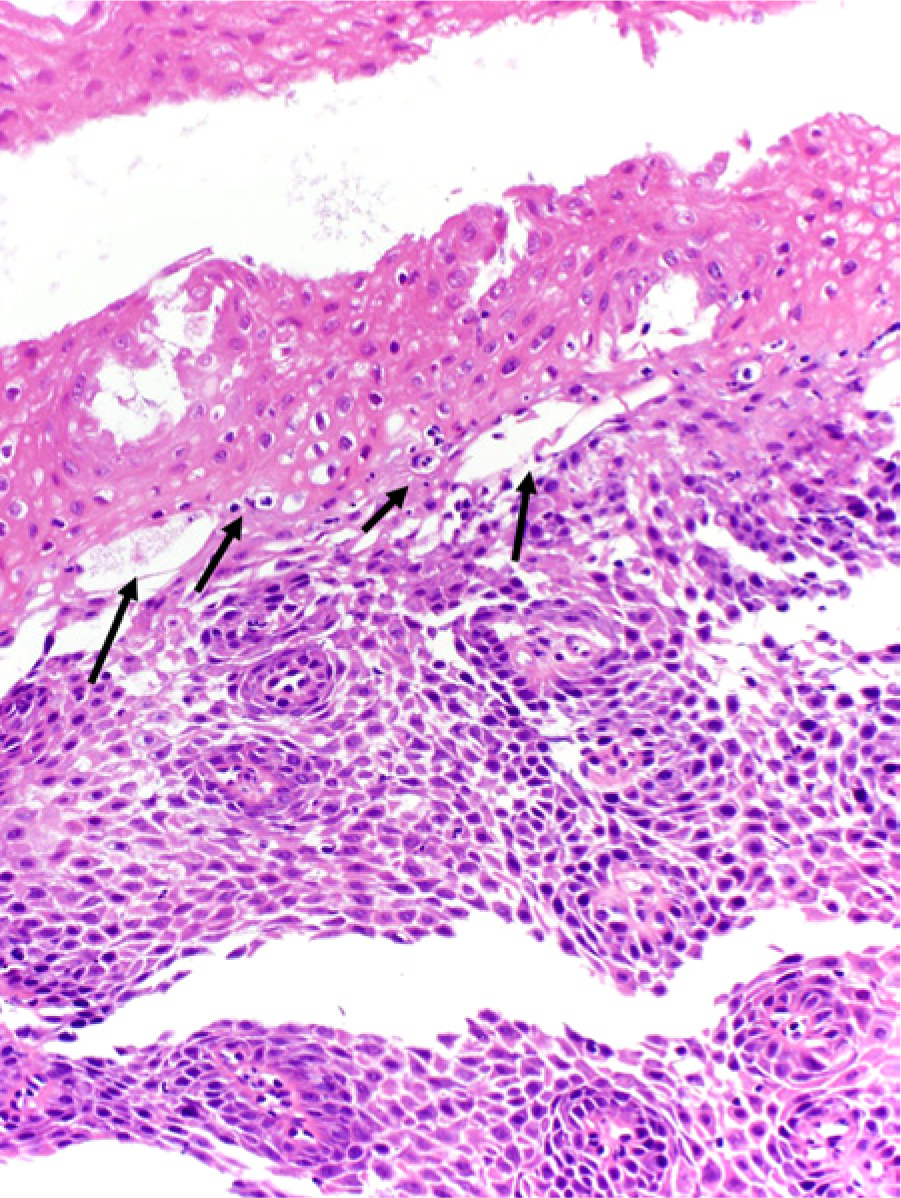
Esophagitis dissecans superficialis (EDS) in a patient taking naproxen. The arrows point to fluid microcysts/bullae with scattered inflammatory cells, all located at the same level in the squamous epithelium. The intraepithelial bullae separate the upper eosinophilic layer of squamous epithelium (the sloughing layer) from the reactive, basophilic, lower layers of the squamous epithelium (2-toned mucosa of EDS) (hematoxylin–eosin stain, 100×).
EDS has been associated with use of multiple drugs in debilitated patients, in particular bisphosphonates, 3 and, more recently, NSAIDs and central nervous system depressants.4,5 EDS resolves completely in the majority of cases.
Stomach
NSAIDs, even at low doses, can cause erosions, ulcers, or necrosis of the gastric mucosa in a high number of users (up to 20% of regular NSAIDs users). 6
Eosinophilia, increase in apoptosis, and reactive gastropathy (RG) may suggest the diagnosis of NSAID-induced gastric injury. Stolte and colleagues 7 have described the histological features of gastric superficial mucosal necrosis due to NSAID as follows: “a homogeneous eosinophilic ischemic necrosis within the area of erosion that blends with the adjacent lamina propria.” Helicobacter-induced erosion instead is covered with “inhomogeneous fibrinoid necrosis” that does not blend “with adjacent lamina propria, containing cell debris and granulocytes.” 8 Erosions due to NSAIDs favor the fundic mucosa, whereas NSAID ulcers favor the antrum, are often chronic, and are prone to complications. 7
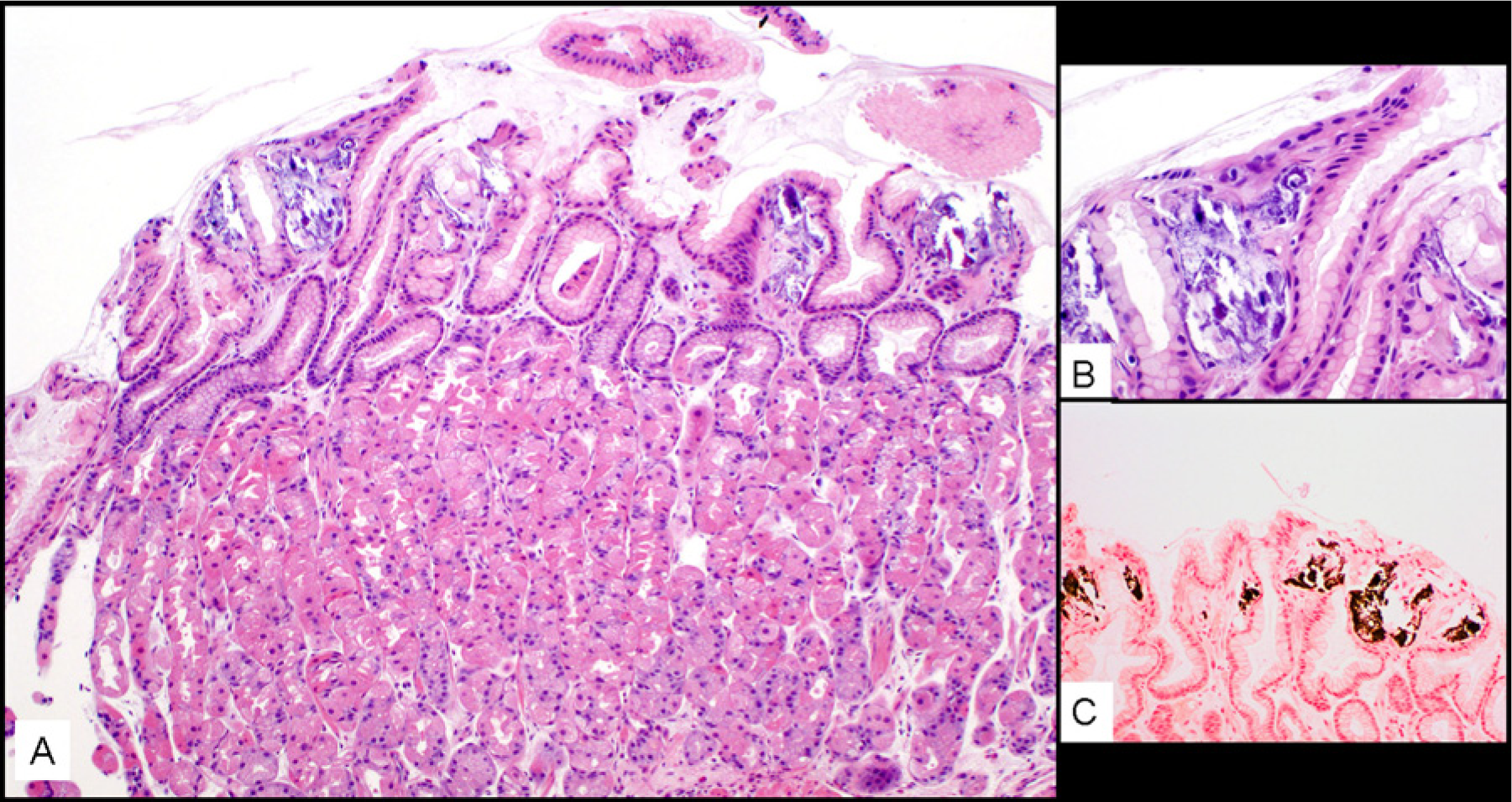
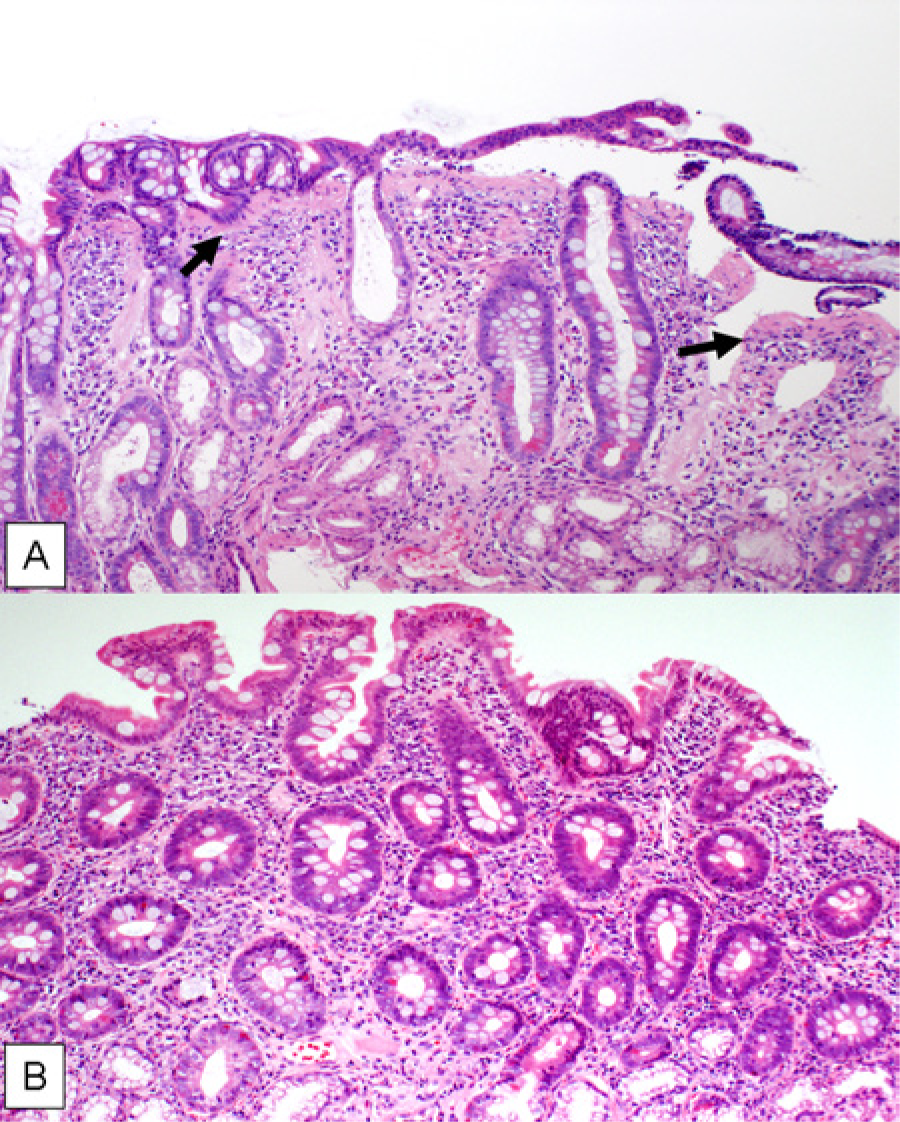
RG is one of the most frequent diagnoses rendered on biopsies of the stomach. 9 It is more frequent in the antrum and is characterized by foveolar hyperplasia with corkscrew-shaped foveolar glands, edema of lamina propria with teleangectasia, increase in smooth muscle fibers in the lamina propria, loss of mucin in foveolar epithelium, lack of inflammation, and exceptional presence of Helicobacter species microorganisms (Figure 2A). While several other conditions can cause RG (eg, bile reflux) the most common cause of RG is NSAID intake. RG is found in 35% to 45% of regular users of NSAIDs.
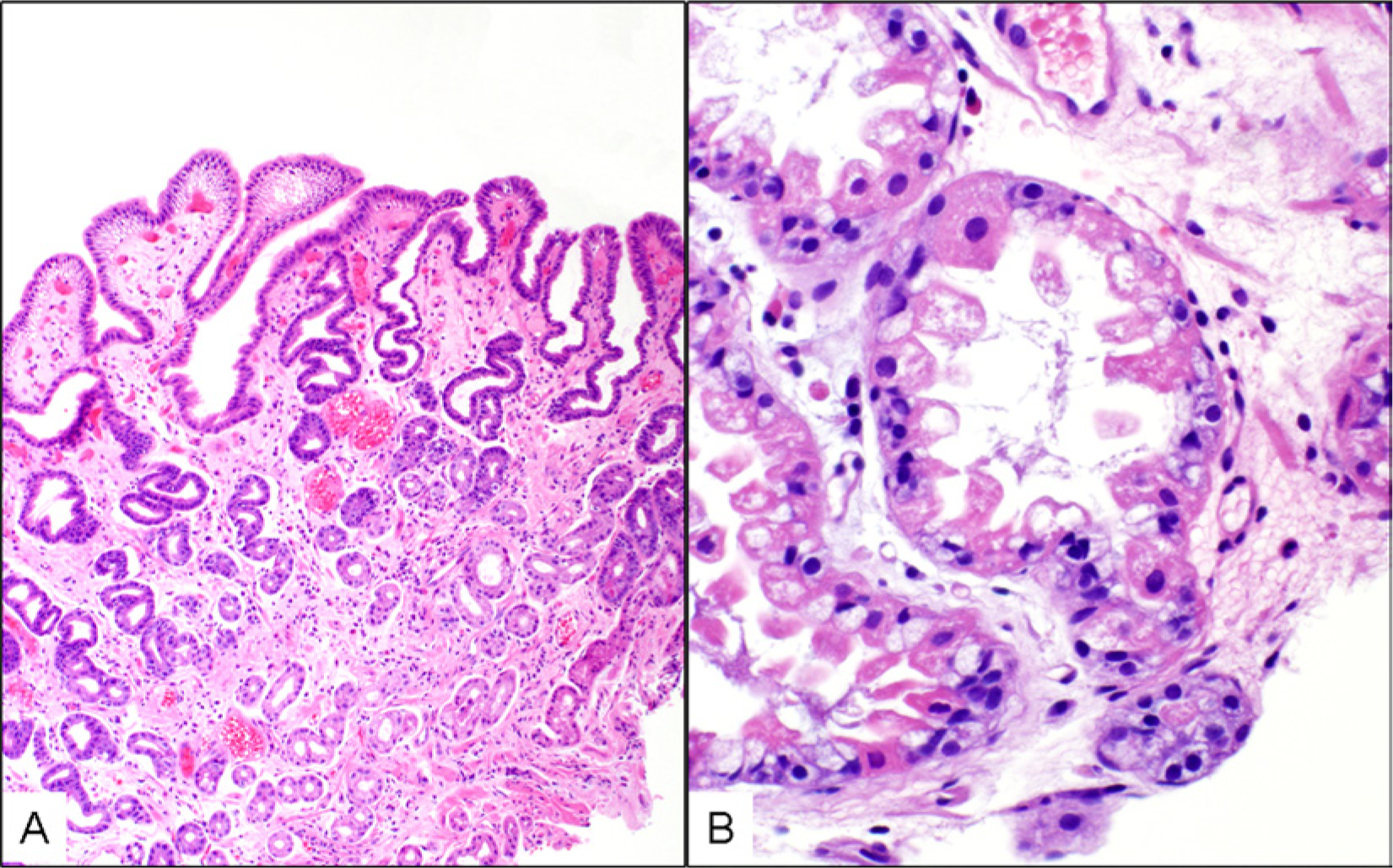
Two of the most common findings in upper GI pathology that are due to drugs: “A” depicts reactive gastropathy (“pale” biopsy due to absence of inflammatory cells and erosion, elongated crypts with corkscrew appearance, reactive, thin, foveolar epithelium). In “B,” the proton pump inhibitor effect in oxyntic glands is shown: dilated fundic glands lumen with frayed edges, protruding parietal cells, prominent vacuolization of cytoplasm.
Tetracyclines are better known as esophago-toxic agents. It has been suggested recently that doxycycline can cause a peculiar variant of RG in which capillary vascular degeneration and microthrombi are observed (Figure 3). 10 The histological abnormalities are therefore similar to gastric antral vascular ectasia (GAVE). In the cases of doxycycline toxicity reported by Xiao et al, 10 the distinction from GAVE was possible because GAVE “watermelon” stomach appearance was not found and because white adherent gastric exudate was seen extending beyond the antrum.
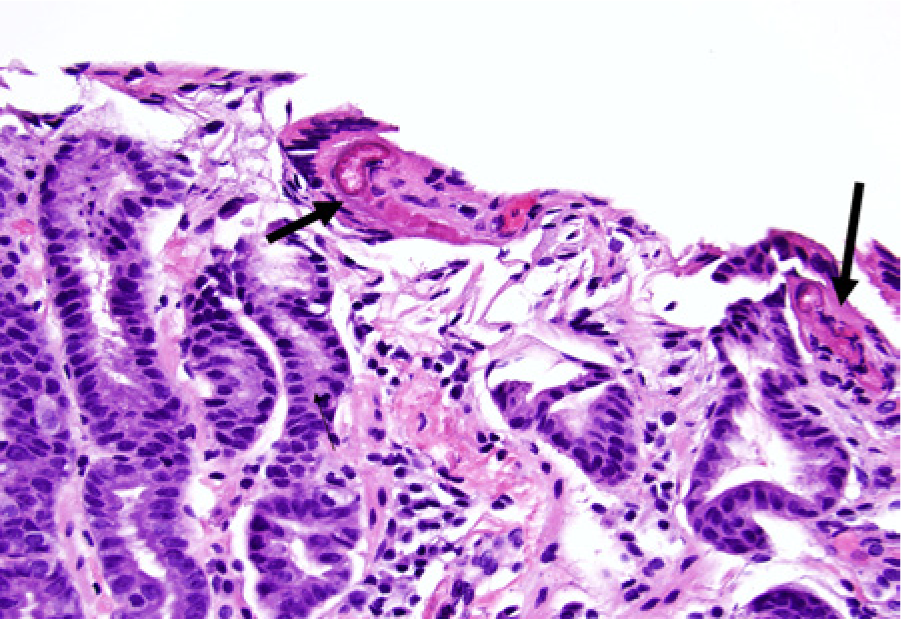
A 65-year-old woman with rosacea, chronic user of doxycycline, complained of abdominal pain. Gastric mucosa shows peculiar degenerative changes in the capillary blood vessels (arrows). The superficial capillary walls are deeply eosinophilic with luminal microthrombi (hematoxylin–eosin stain, 400×). Abdominal pain disappeared with stoppage of doxycycline; follow-up biopsies were normal.
Proton pump inhibitors (PPIs) can cause hypertrophy of parietal cells due to hypergastrinemia. This is a very common phenomenon as PPIs are widely available and prescribed and the patients present at endoscopy without interrupting the symptomatic PPI therapy. The parietal cells protrude into the lumen of the oxyntic gland, can become vacuolated, and confer a serrated, even frayed, look to the lumen of the oxyntic glands, which appear dilated (Figure 2B). These changes occur in other situations with hypergastrinemia such as Zollinger–Ellison syndrome. It is generally thought that PPIs cause fundic gland polyps. These are seen in 17% to 35% of patients after 12 months of PPIs therapy, are typically multiple, sessile, fundic, and small (less than a centimeter). They show cystic dilatations of the oxyntic glands lined by chief, parietal, and mucus cells.
Morphological changes due to PPIs regress if PPI intake ceases. PPIs reduce the number of Helicobacter pylori microorganisms and the intensity of the gastritis in the antrum.
PPIs cause a shift in the presence of the Helicobacter bacteria from the antrum to the fundus and from the foveolar surface to the deeper oxyntic glands, even into the intracellular canaliculi of the parietal cells. PPIs can further complicate the detection of H pylori as they can cause false-negative urea breath tests. 11 PPI therapy induces apoptosis in the antrum reducing the usefulness of antral biopsy in the diagnosis of low-grade graft-versus-host disease (GVHD); the fundic mucosa appears instead surprisingly unaffected by the apoptotic PPI effect and is therefore more reliable for the diagnosis of low-grade GVHD in the stomach. 12
Selective internal radiation therapy with yttrium-90-emitting microspheres can induce radiation gastritis that can be easily diagnosed when the distinctive microspheres are in the histology slides at hand. Microspheres, introduced via the hepatic artery for therapy of unresectable liver cancer or liver metastases, become misdirected or migrate into gastric vessels. These microspheres can migrate also to pancreas, esophagus, gallbladder, and other organs. Microspheres appear as dense, ink jet black, round objects, 30 to 40 µm in size, scattered in the vessels of gastric mucosa that shows radiation injury (Figure 4). Yttrium-90 so delivered to the stomach may cause ulceration, bleeding, and perforation (rate of complications varies from 3% to 24% of cases). 13 The gastric complications are difficult to treat and may delay potentially curative treatment of the primary malignancy. 14 The differential diagnosis of gastric dysplasia can arise in the settings of selective internal radiation or in hepatic arterial chemotherapy infusion. In radiation-induced atypia, stromal cells are also affected, the changes are limited to the base of the glands, there is vacuolization, and mitoses are scant.
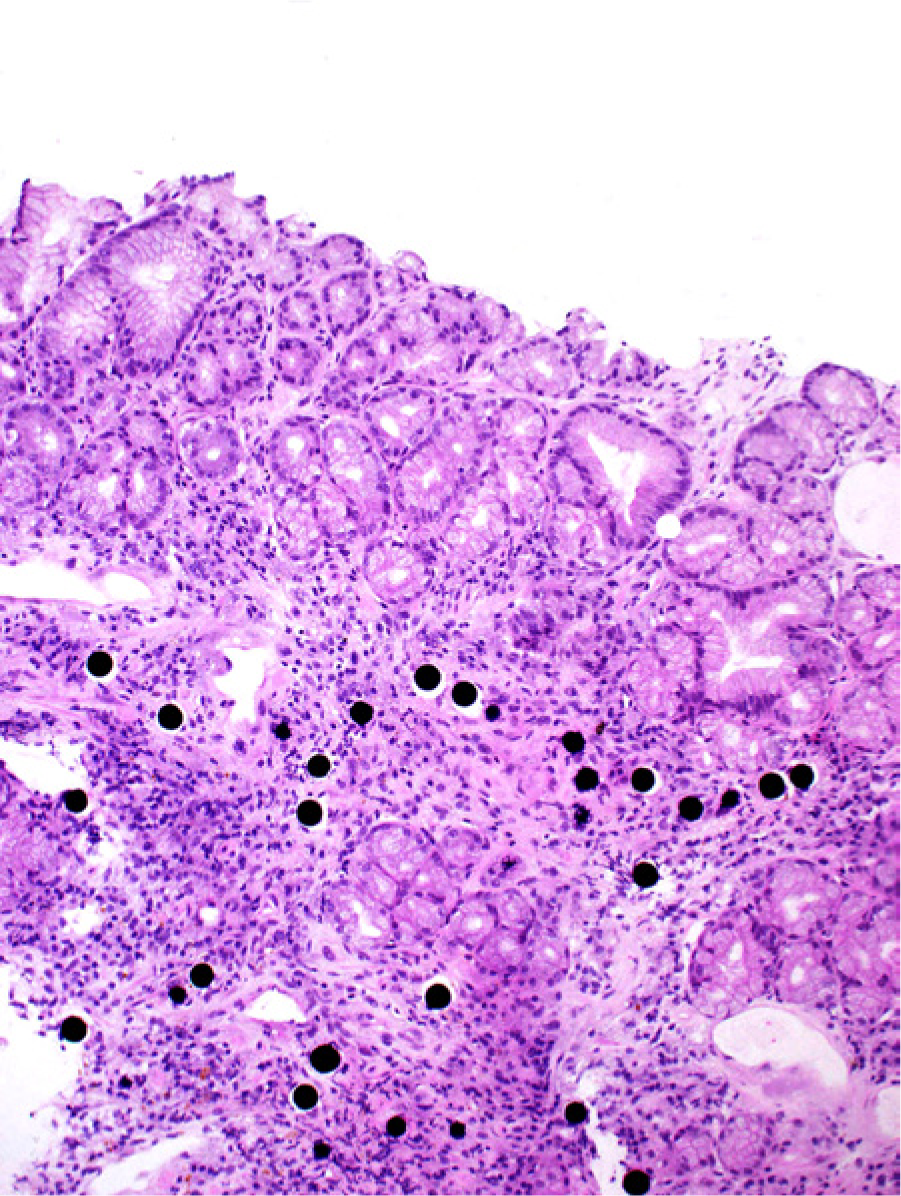
Ytrrium-90-emitting microspheres used in selective internal radiation are easily identified by their perfectly round, ink jet black appearance, and uniform size; in this case they are lodged in gastric mucosa (hematoxylin–eosin stain, 40×).
The condition called gastric calcinosis (GC) is a usually asymptomatic abnormality that may occur associated with hypercalcemia or in the posttransplant setting. GC may be a marker of generalized metastatic calcification, a significant clinical condition. The endoscopic manifestations of GC are whitish plaques and nodules in the stomach. Histology shows amorphous, non-birifringent, basophilic deposits, usually seen in the superficial lamina propria of normal appearing mucosa. The deposits are positive for the Von Kossa stain (Figure 5).
Example of gastric calcinosis in post–renal transplant patient taking sucralfate. The calcium is deposited in the superficial aspect of the lamina propria (shown in A, 100×, hematoxylin–eosin stain), just below the superficial epithelium (better shown in B, 200×). Von Kossa stain–positive reaction is shown in C.
Drugs such as sucralfate, alendronate, aluminum-containing antacids, isotretinoin, and citrate-containing blood products have been associated with GC arising on the background of a variety of clinical conditions. The mechanistic relationship, if any exists, of the drugs with calcinosis is unclear.15,16
Olmesartan (Benicar), an antihypertensive drug that acts as an angiotensin II receptor inhibitor, can cause collagenous gastritis and/or lymphocytic gastritis and collagenous enteritis often in combination. 17 The collagenous diseases of the gastrointestinal tract due to olmesartan may be indistinguishable from the non-drug-related idiopathic or celiac disease related conditions (Figure 6).
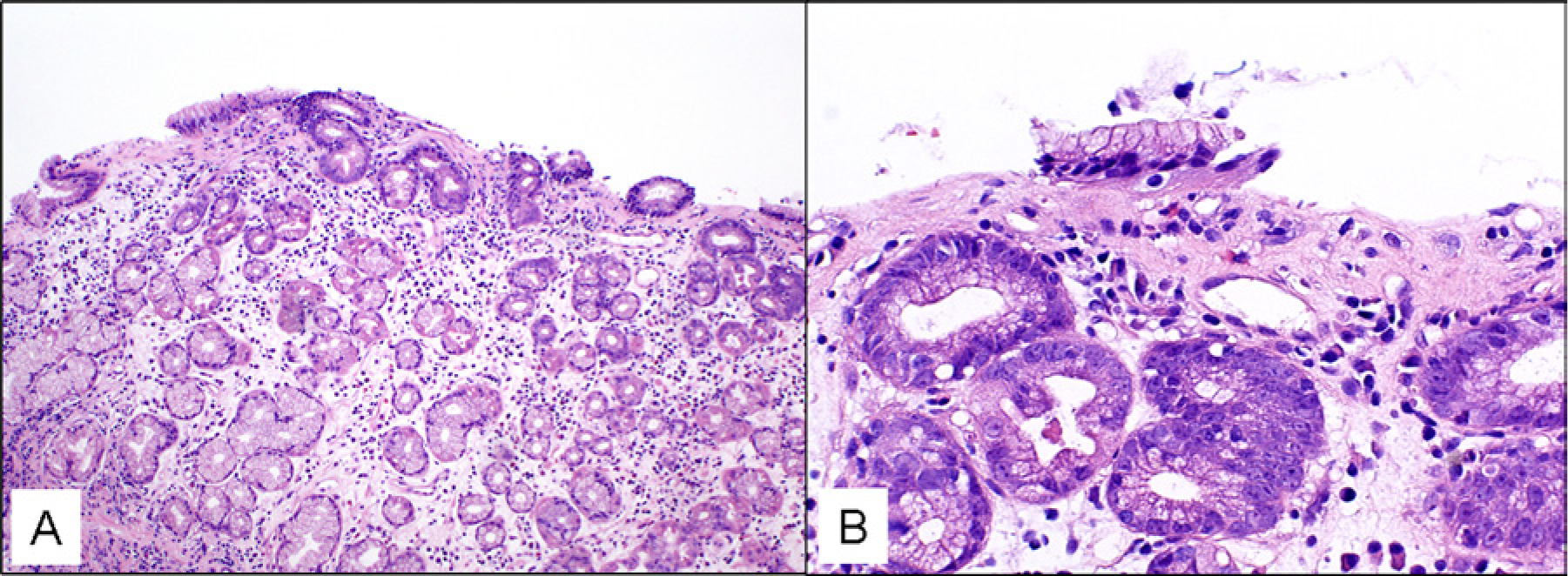
Collagenous gastritis is an uncommon condition characterized by thickened collagen plate below the superficial epithelium of the stomach (A, hematoxylin–eosin stain, 100×) with capillaries and stromal cells embedded in the newly deposited collagen (B, 400×). Note the missing superficial epithelium. While association with celiac disease and other autoimmune disorders is known, in this case the disease was associated with olmesartan intake. The histology improved completely after the withdrawal of the drug.
Small Intestine
Endoscopic exploration of the small intestine (SI) is now widespread. As a consequence, the detection of drug-induced injury has increased. The use of enteric resistant coating that may shift the side effects beyond the upper GI is among the mechanisms thought responsible for the effects of NSAIDs in the SI.
NSAIDs cause erosions and ulcers throughout the SI but especially at its 2 ends: the duodenal bulb and the terminal ileum. NSAID-induced ulcers are without distinctive histologic features, are common (47% of patients with rheumatoid arthritis taking NSAIDs had ulcers in the SI 18 ), well demarcated, punched out, can be aphthoid, and arise in a noninflammatory background. An exception to this lack of specificity could be the macroscopic appearance of the circumferential ulcers associated with the tips of the diaphragms in diaphragm disease (Figure 7). 19 When compared to Crohn’s disease, NSAID injuries lack, or induce only very rarely, granulomas and cause less inflammation or architectural distortion. Pseudopyloric metaplasia can be seen in diaphragm disease, usually in proximity of the eroded mucosa. Rosary bead-like distribution of deep mural lymphoid nodular aggregates, fissuring, and fistulae are not seen in NSAID injury. Important is the capacity of NSAIDs to cause villous atrophy 19 (Figure 8; a list of drugs capable of causing villous atrophy is provided in Table 1), intraepithelial lymphocytosis, and to induce distinctive structural changes to the wall of the intestine called diaphragm disease. 19
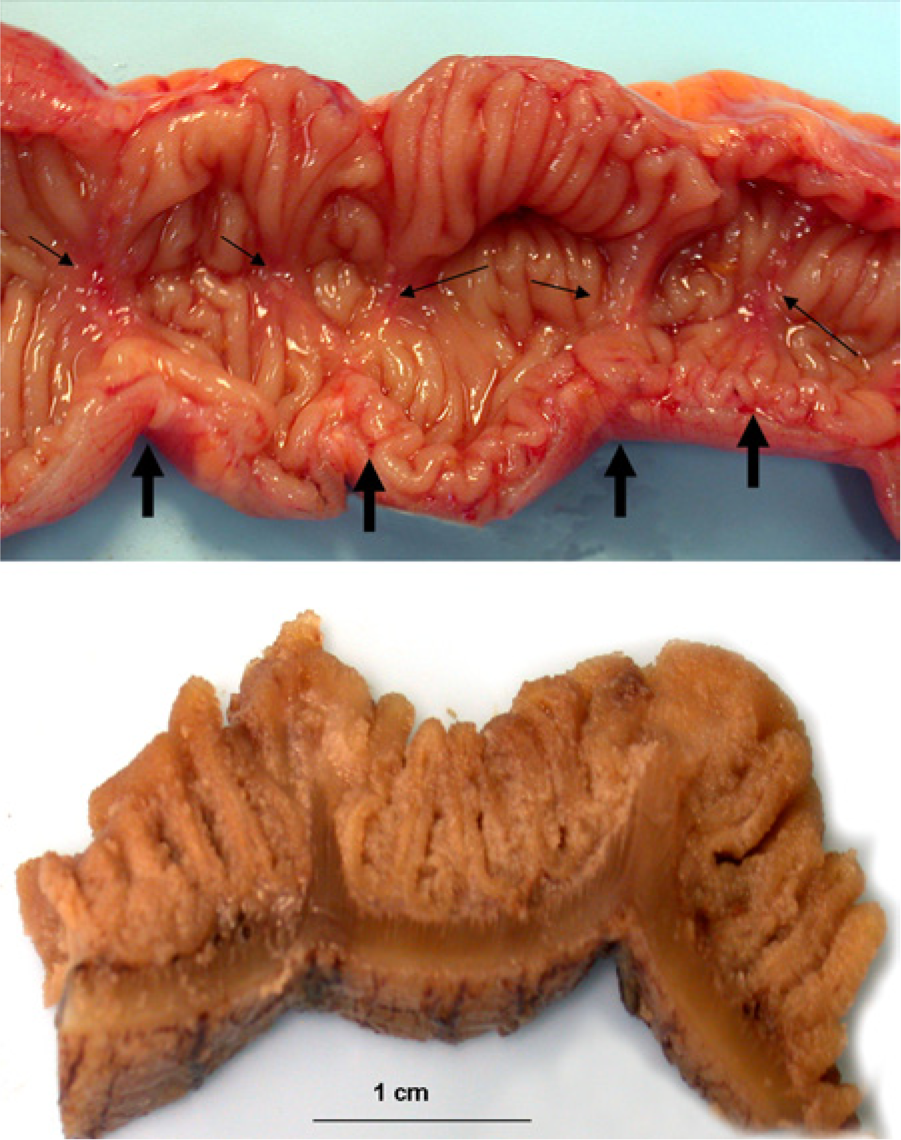
A 65-year-old woman with long history of orthopedic procedure and NSAID intake presented with symptoms of subacute obstruction and anemia. Laparotomy revealed circular stenoses of the distal ileum. Resection of affected ileum showed (A) multiple diaphragms in the open segment of intestine (arrows). Note the circular circumferential ulcers on the tips of the diaphragms. In “B,” the formalin-fixed resection specimen shows the diaphragms to better avail. Reproduced with modifications from reference 19 with permission, © 2008-13 American Society for Clinical Pathology, © 2008-13 American Journal of Clinical Pathology.
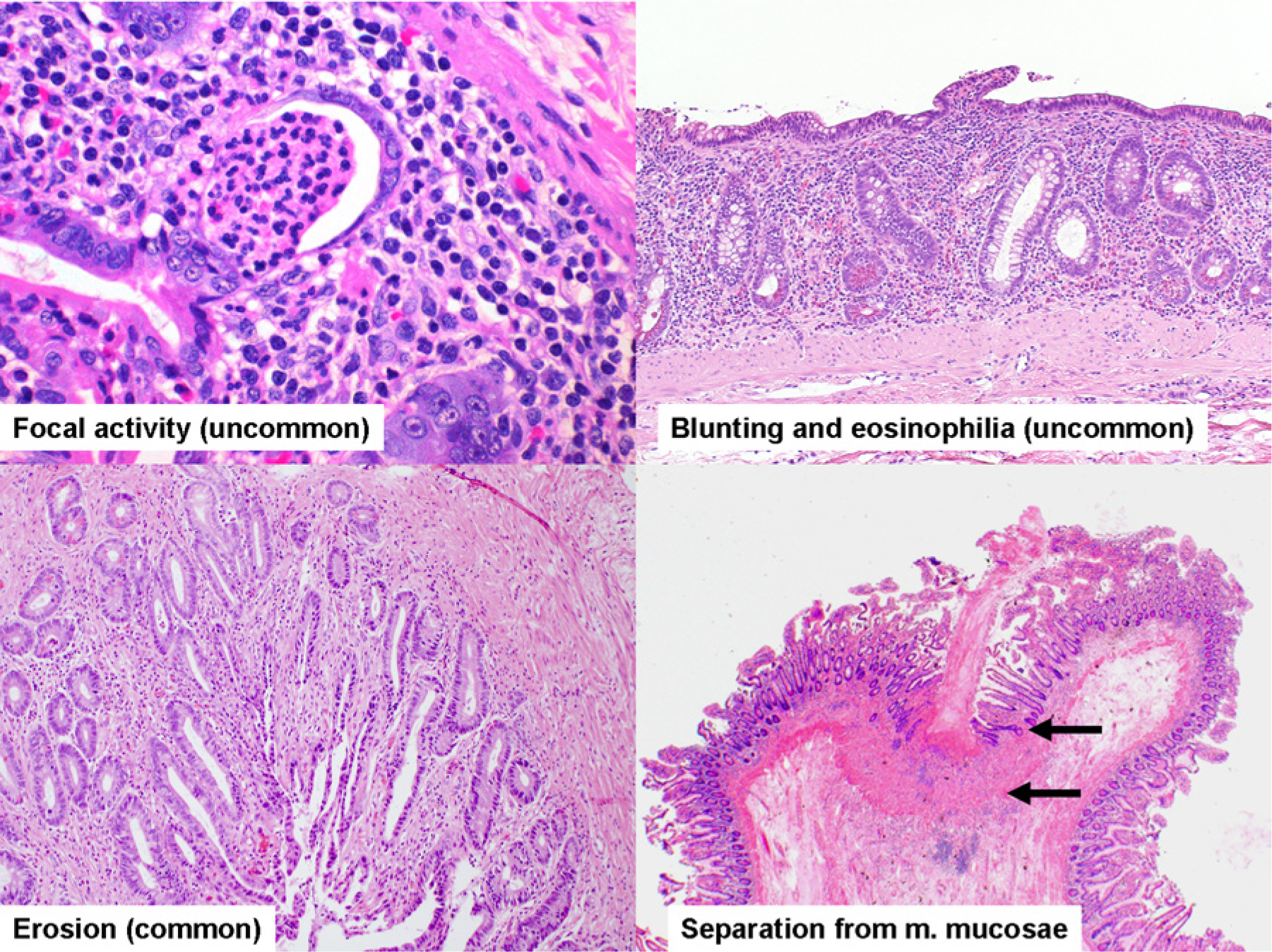
The spectrum of abnormalities in NSAID enteropathy associated with diaphragm disease: rare are focal activity and villous atrophy with eosinophilia, common instead are erosions. The tip of a diaphragm in the bottom right shows the typical crater-like ulcer and the adjacent separation of crypts bases from the m. mucosae. Reproduced with modifications from reference 19 with permission, © 2008-13 American Society for Clinical Pathology, © 2008-13 American Journal of Clinical Pathology.
Drugs Capable of Causing Small Intestine Villous Atrophy.
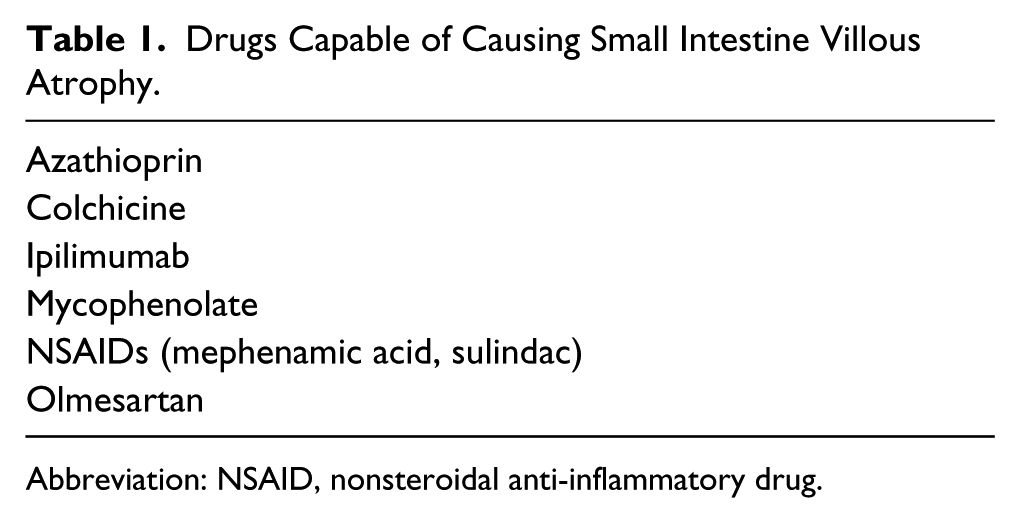
Abbreviation: NSAID, nonsteroidal anti-inflammatory drug.
Diaphragm disease (DD) is associated with the prolonged use of high doses of NSAIDs but is not exclusively due to these drugs and should not be considered always synonymous of NSAID use. DD is characterized by often ulcerated, circumferential, tent-like, short, stenosing luminal projections that occur especially in the SI and right colon, but also in duodenum and stomach. The lumen of the intestine can be reduced to a diameter of a few millimeters. The stenotic areas appear much less impressive once the segment of intestine is opened longitudinally, with an effect on the restricted area truly resembling the release of a tied string. Modest circumferential fibrosis in areas with circumferential “napkin-ring”-like constrictions can be seen on the serosa. The pattern of nonspecific histologic features in a diaphragm and in the background mucosa of DD is shown in Figure 8. Of note is that numerous NSAID-linked abnormalities in the background mucosa may create a pattern of injury that may be diagnostically useful. 19
Patients with chronic diarrhea, weight loss, and frequent hospitalization with villous atrophy and collagenous enteritis resistant to gluten-free diet, and with no serological evidence of celiac disease, showed complete clinical reversal and histological recovery after discontinuation of olmesartan and resumption of gluten-containing diet in a recent study of 22 patients from Mayo Clinic. 17 While collagenous enteritis is considered a rare and serious disease of the small bowel associated with celiac disease in a significant percentage of the cases, in the dramatic olmesartan-linked injury the clinical improvement is reliably, and often promptly, obtained after cessation of the drug use; the pathological changes can be reversed completely (Figure 9). The importance of this observation cannot be overemphasized given the progressive malabsorption and higher mortality otherwise associated with conventional collagenous enteritis. 20 In the case of olmesartan-associated spruelike enteropathy, a drug effect has cast a completely new light in the differential diagnosis on an entity known to be difficult to treat and for long time thought to be simply a marker of poor prognosis celiac disease. 21
Collagenous enteritis in hypertensive patient taking olmesartan. There was no serological evidence of markers of celiac disease, and no response to gluten free-diet was obtained. In “A,” arrows point to thickened collagen plate. As typical of olmesartan-associated enteropathy, the abnormality disappeared after withdrawal of the drug (B) with dramatic symptomatic improvement (hematoxylin–eosin stain, 200×).
Leprosy has no specific GI involvement, so GI symptoms in such patients should be thought primarily as related to therapy. Clofazimine is a drug used in the treatment of leprosy and other mycobacterial infections. Clofazimine can impart a brown coloration to the intestine (reversible on discontinuation of the drug), the skin, and most body fluids and secretions. Patients on high doses of clofazimine may develop, even after cessation of the drug, intestinal and lymph nodal clofazimine-induced crystal storing histiocytosis. 22 The crystals are soluble in alcohol and will appear clear in routine hematoxylin–eosin section but red in frozen sections or in alcohol-fixed tissue. Crystals of clofazimine display bright red birefringence under polarized light; they are PAS negative while those associated with B cell neoplasm, the main differential diagnosis, are PAS positive.
Colon
The endoscopic examination of the colon requires preparation for examination. The products used for this purpose are capable of morphological effects. An example of the iatrogenic effect is provided by sodium phosphate (NaPO4), a laxative used for colon preparation to endoscopy, which is capable of inducing aphtous lesions, focal active colitis, and increased apoptosis.
Iatrogenic chemical colitis can follow glutaraldehyde and hydrogen peroxide contact with the mucosa or as contaminant (glutaraldehyde is a germicide used at 2% solution to disinfect endoscopes and can remain in the instrument if not properly cleansed) or as component of enemas (hydrogen peroxide was used in the past in fecal impaction and in meconium ileus treatment, practices largely abandoned; occasional use as laxative is still reported, however). 23 The injury due to these compounds closely resembles ischemic colitis (Figure 10), including the frequent presence of pseudomembranes and/or nonspecific inflammatory patchy colitis. Usually, the symptoms appear 24 to 48 hours after exposure but can occur immediately after or even during the procedure.
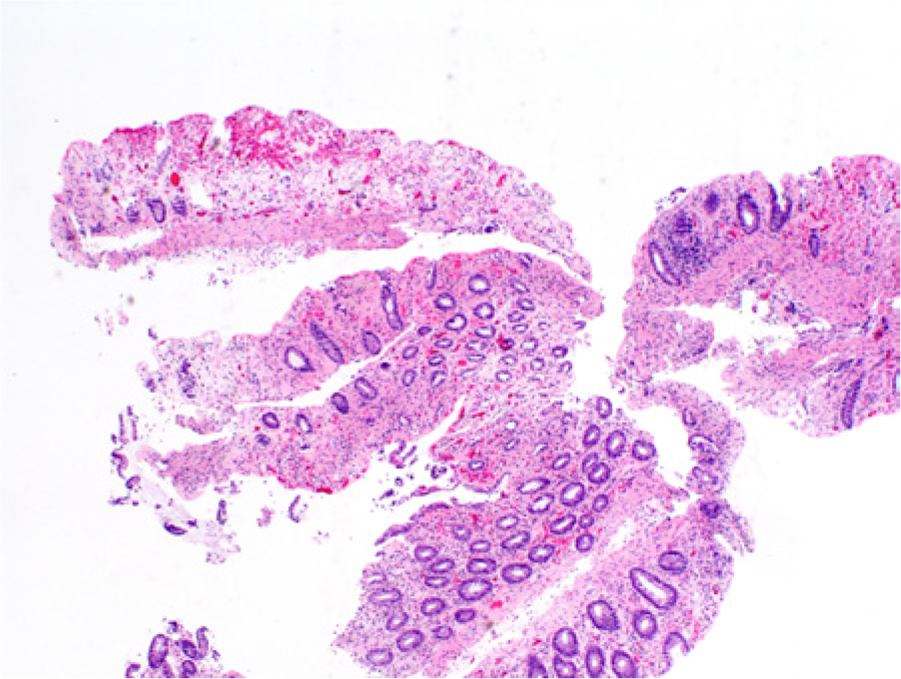
Chemical colitis with features of ischemic colitis due to enema with hydrogen peroxide (hematoxylin–eosin stain, 100×).
Morphologic lesions due to drugs in the colon are thought to be relatively uncommon (with the exception of melanosis coli, due to antrachinonic laxatives, and pseudomembranous colitis, due to antibiotics). Colonic histopathological drug-induced adverse effects can be categorized according to the pattern of lesions they cause (Table 2). The role of biological agents in generation of colitis was presented in Part I of this review.
Colitis Patterns with, Underneath, the Lists of Drugs Most Commonly Associated with Them.
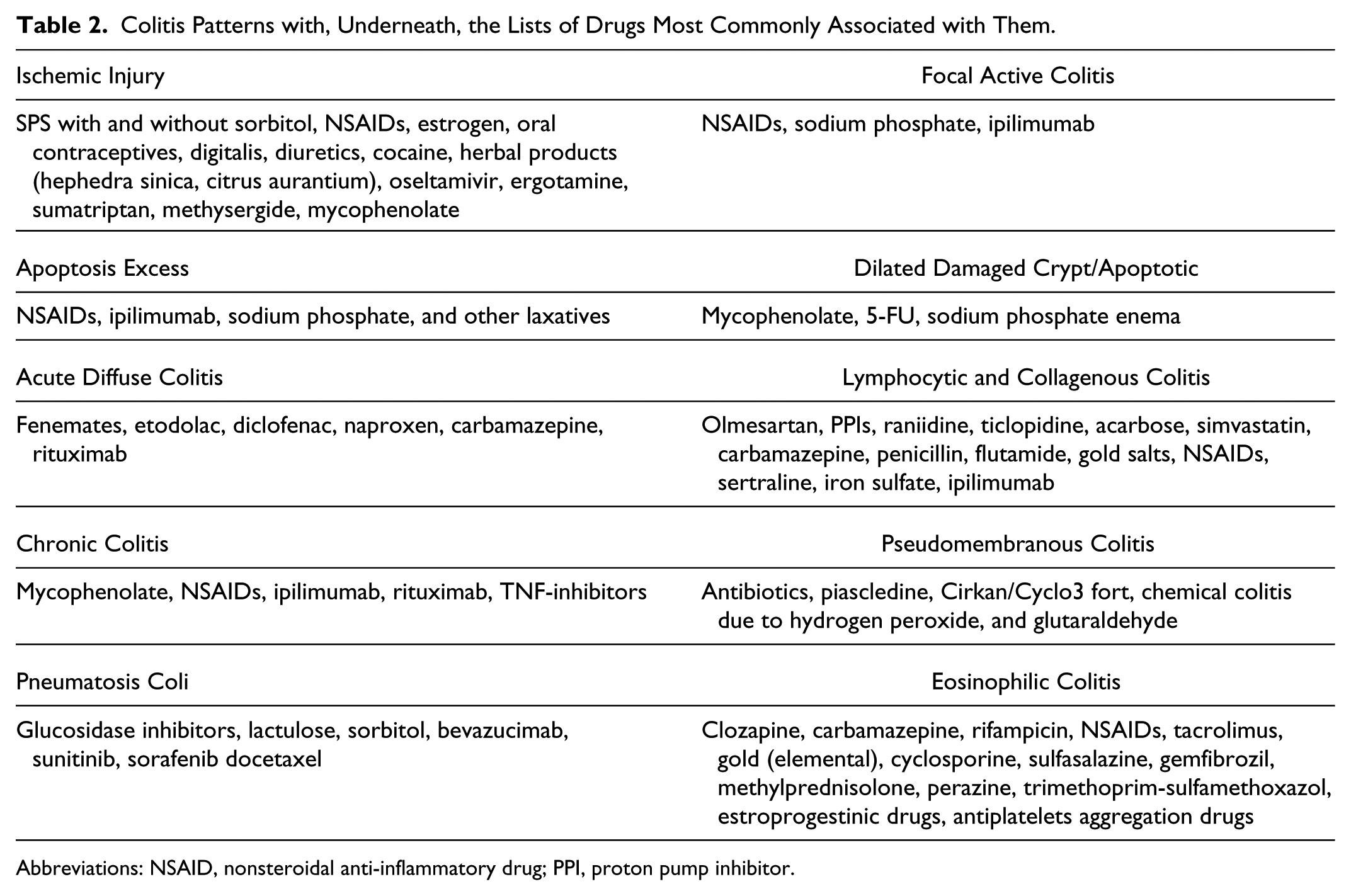
Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; PPI, proton pump inhibitor.
NSAIDs can be a direct cause of injury or can aggravate preexisting conditions (eg, diverticulitis, inflammatory bowel disease [IBD]). Colonic NSAID injuries are histologically nonspecific and/or not thought to be secondary to a drug. These adverse effects include microscopic colitis (be it lymphocytic or collagenous type), focal active colitis, chronic colitis, eosinophilic colitis, and ischemic colitis.
Focal active colitis due to NSAIDs is reported as of the basal type, in which granulocytes are seen in the occasional crypt base. 24 Granuloma formation has been reported following Sulindac. 25 Goldstein and Cinenza showed mild crypt disarray and mixed inflammatory infiltrates associated with NSAIDs in the colon. 26 Deshpande et al 27 reported regression of idiopathic incidental chronic colitis in 2 of 17 cases after discontinuation of NSAIDs. In addition, the patients’ distal ileitis also regressed. Eight of their 17 patients had documented use of NSAIDs. The colitis displayed basal lymphoplasmacytosis and crypts distortion, was patchy, and was located in the right colon and cecum. The localization in the right colon is intriguing as it emphasizes a previous observation of Mutinga et al: in their study 75% of left-sided ulcerative colitis patients who also showed patchy right-sided inflammation took NSAIDs. 28
Ischemic-type lesions, particularly at young age, should always raise suspicion of a drug adverse effect. Drugs can cause ischemic colitis because of vasoconstriction (eg, cocaine causing severe ischemia with gangrene, ergotamine causing shallow ulcers in rectum), reduced blood flow (eg, digitalis or diuretics), thromboses (eg, due to estrogens with injury favoring the rectum and splenic flexure), 29 or bleeding (eg, due to anticoagulants).
A drug that can produce IBD-like changes with marked apoptosis is mycophenolate, a compound used extensively in allograft maintenance and as immunosuppressive. Mycophenolate mofetil (MMF; CellCept, Genentech, absorbed in the stomach) or mycophenolate sodium (marketed under the name Myofortic, Novartis, an enteric coated drug absorbed in the intestine) are converted in the active metabolite mycophenolic acid (MPA). MPA inhibits inositol monophosphate dehydrogenase, which is critical to the de novo synthesis of guanine nucleotide in both B- and T-lymphocytes. Other tissues are less dependent on this enzyme as they have salvage or back-up pathways, making the drug relatively specific to target lymphoid cells. Although less targeted than lymphocytes, the proliferation of enterocytes can be inhibited by MPA that remains, thus capable of causing epithelial injury.
The colitis induced by MMF, while sometimes referred to as Crohn’s-like, is more often a “dilated, apoptotic, damaged crypt” form of colitis similar to low-grade GVHD 30 : crypt disarray, occasional crypt dilatation with increased epithelial cell apoptosis, eosinophilic debris in the lumen, thin stretched eosinophilic crypt lining cells, and lamina propria inflammation are the features of MMF colitis (Figure 11). After bone marrow transplant, the differential diagnosis of MMF colitis with GVHD in a cytomegalovirus (CMV)-negative colon (CMV colitis is another “dilated damaged crypt” process mimicking GVHD) is difficult. If suspension of MMF is clinically possible, regression of MMF colitis will be prompt and diagnostic. Mild GVHD-like changes in patients exposed to MMF extend also to other portions of the GI tract with apoptosis increased in esophagus, stomach, and small bowel. 31 In the upper GI tract, erosion and ulcers of esophagus, RG, chronic peptic duodenitis, and Crohn’s-like injuries are associated with MMF, suggesting a generalized adverse mucosal effect due to MMF.
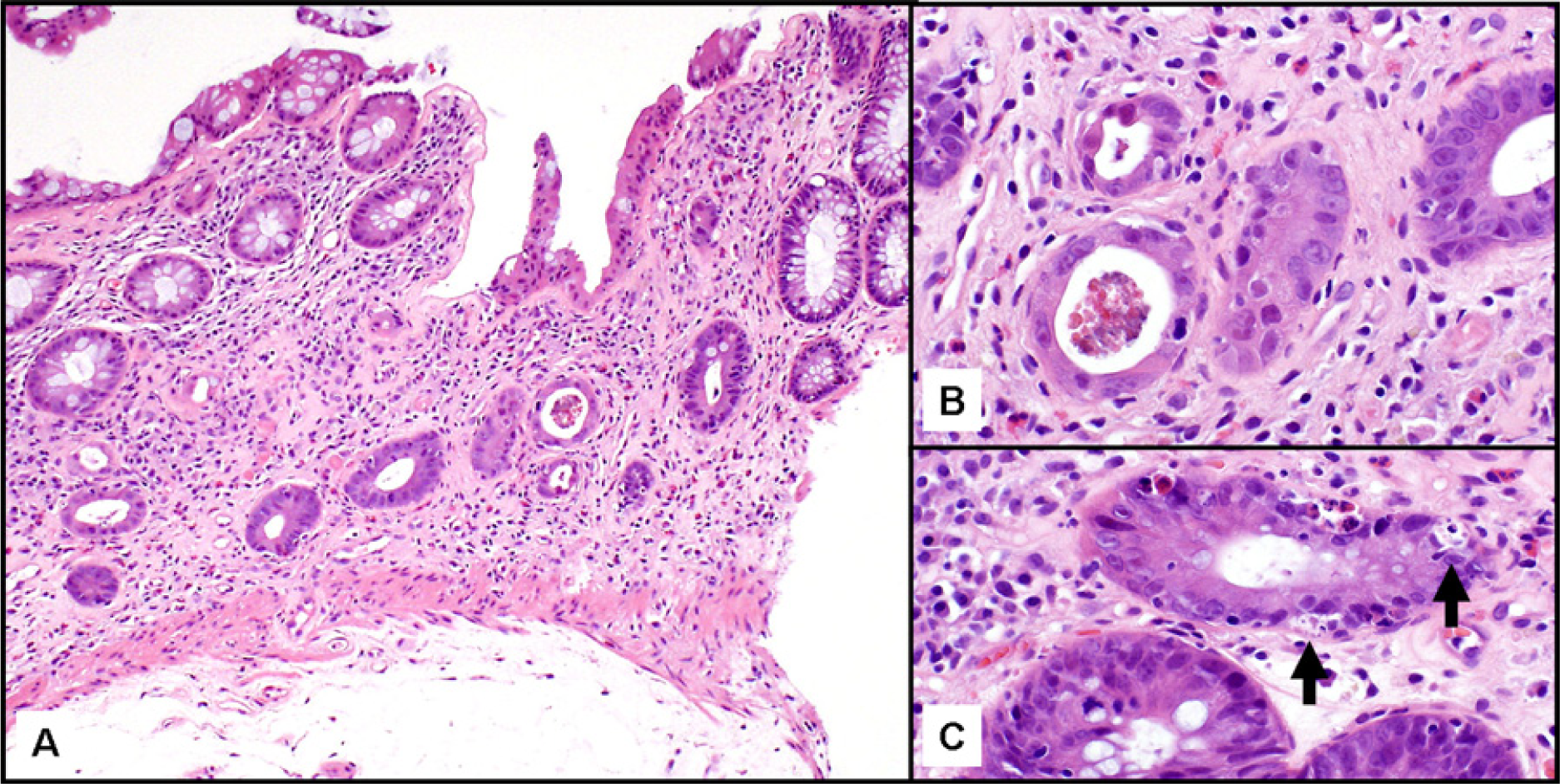
Colitis due to mycophenolate (MMF). In “A,” crypts disarray with few dilated damaged crypts (hematoxylin–eosin stain, 200×). Eosinophilia of the epithelium can be appreciated with greater clarity in “B.” Apoptotic bodies are part of MMF colitis and are shown in “C” (arrows). (B and C: 400×).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.