
Abstract
Selected antibodies that have become available in recent years and have applications in diagnostic pathology are discussed. They include antibodies that are organ-related, provide information on cellular differentiation or histogenetic type, have predictive value in tumors, and highlight infective agents. PAX8 (paired box gene 8) is a marker expressed in the lower female genital tract, thyroid, and kidney and their tumors. Napsin A is expressed in the lung and kidney and is an alternative marker for pulmonary adenocarcinoma. Arginase A is a sensitive and specific marker for liver tumors. ERG (Ets-related gene) is an excellent marker for endothelium and vascular tumors as well as prostatic cancer (about 50% of cases). SOX10 (SRY-related HMG box) is expressed predominantly in melanocytic and Schwann cells and the corresponding tumors. DOG1 (discovered on GIST 1) is an excellent marker for gastrointestinal stromal tumor (GIST) and acinic cell carcinoma. OCT3/4 is a pan–germ cell tumor marker, except yolk sac tumor. SALL4 is positive in various types of germ cell tumors, including yolk sac tumor. MUC4 (mucin-related antigen 4) is a sensitive and specific marker for low-grade fibromyxoid sarcoma. Langerin is a specific marker for Langerhans cells and their tumors. SOX11 is a sensitive marker for mantle cell lymphoma. New generation antibodies against anaplastic lymphoma kinase (ALK) are required to reliably demonstrate ALK gene translocation in pulmonary carcinomas. Lack of expression of succinate dehydrogenase B is seen in paragangliomas of the hereditary form and in the pediatric type of GIST. Antibodies against Trepenoma pallidum can facilitate the diagnosis of syphilis, whereas those against SV40 (simian virus 40) are helpful for diagnosis of BK virus infection and progressive multifocal leukoencephalopathy.
Keywords
Immunohistochemistry has remarkably revolutionized the practice of surgical pathology during the past few decades. The ever-expanding range of commercially available antibodies permits new applications in diagnostic practice, creating opportunities to solve problems not previously possible. In this review, selected antibodies that have become available in recent years and have applications in diagnostic pathology are discussed (Table 1). Additional antibodies are discussed in the separate review, “The utility of immunohistochemistry for providing genetic information on tumors.” 1
Newly Available Antibodies Discussed in This Review.
Abbreviations: PAX8, paired box gene 8; ERG, Ets-related gene; SOX, SRY-related HMG box; DOG1, discovered on GIST 1; MUC4, mucin-related antigen 4; SV40, simian virus 40; ALK, anaplastic lymphoma kinase.
PAX8 (Paired Box Gene 8)
Nature of Antigen and Immunoreactivity in Normal Cells
PAX8 is a transcription factor essential for organogenesis of the thyroid, kidney, and Mullerian system. The normal cells that are PAX8 positive, with nuclear staining pattern, include the following: 2
thyroid—follicular epithelium;
kidney—tubular epithelium and Bowman capsule lining cell;
female genital tract—ovary (inclusion cysts and rete ovarii but not surface mesothelium), fallopian tube (epithelium), uterus (epithelium), endocervix (epithelium, with weak to moderate staining) 3 ;
male genital tract—epithelium from rete testis to ejaculatory duct 4 ;
thymus—thymic epithelium (weak staining) 5 ;
pancreas—islet cells 6 ; and
lymphocytes—some lymphoid cells, especially those in lymphoid follicles, are PAX8 positive, because of cross reaction with PAX5. 7
Immunoreactivity in Tumors and Practical Applications
The immunoreactivity of PAX8 in tumors mirrors the pattern seen in normal cells.
In the thyroid, follicular-related neoplasms (follicular adenoma, follicular carcinoma, papillary carcinoma, and poorly differentiated carcinoma) are positive in practically 100% of cases, anaplastic carcinomas in 79% (often focal), and medullary carcinoma in 75% (often focal). 8
All types of renal cell carcinoma, including collecting ductal carcinoma, are positive. 9 The positivity rates in clear-cell, chromophobe, and papillary types are 93%, 80%, and 95%, respectively. 9 Oncocytomas are positive in approximately 90%.9-11 Urothelial carcinomas are usually negative. In the bladder, nephrogenic adenoma and clear cell adenocarcinoma are positive for PAX8, whereas urothelial carcinoma and prostatic carcinoma are usually negative. 12
Serous, endometrioid, and clear-cell types of ovarian carcinoma are positive in virtually 100% of cases, transitional/undifferentiated carcinomas in 67%, and mucinous tumors in 8% to 22%.2,3,10 Primary serous carcinoma of the peritoneum is consistently positive, whereas mesothelioma is negative except for focal weak staining in occasional cases. 13 Endometrial carcinoma is PAX8 positive. 10 Cervical adenocarcinoma is positive in a variable proportion of cases, whereas mesonephric adenocarcinoma is consistently positive.10,14
In the male genital tract, PAX8 expression occurs in serous cystadenoma of the epididymis, carcinoma of the rete testis, Wolffian adnexal tumor of the seminal vesicle, and endometrioid carcinoma of the seminal vesicle. 4
Thymomas are positive for PAX8 in 93% to 100% of cases and thymic carcinomas in 77%.5,10
Pancreatic neuroendocrine tumors are positive for PAX8 in 67% of cases, with the percentage being higher in the well-differentiated tumors. Among well-differentiated neuroendocrine tumors of other sites, PAX8 positivity rates are as follows: lung 0%, stomach 20%, duodenum 100%, ileum 0%, appendix 21%, and rectum 85%. 6
Thus, there are several major applications in surgical pathology practice:
aid in diagnosis of anaplastic thyroid carcinoma (often PAX8 positive, but TTF1 [thyroid transcription factor 1] negative);
aid in confirming the kidney origin of a carcinoma, in the correct setting;
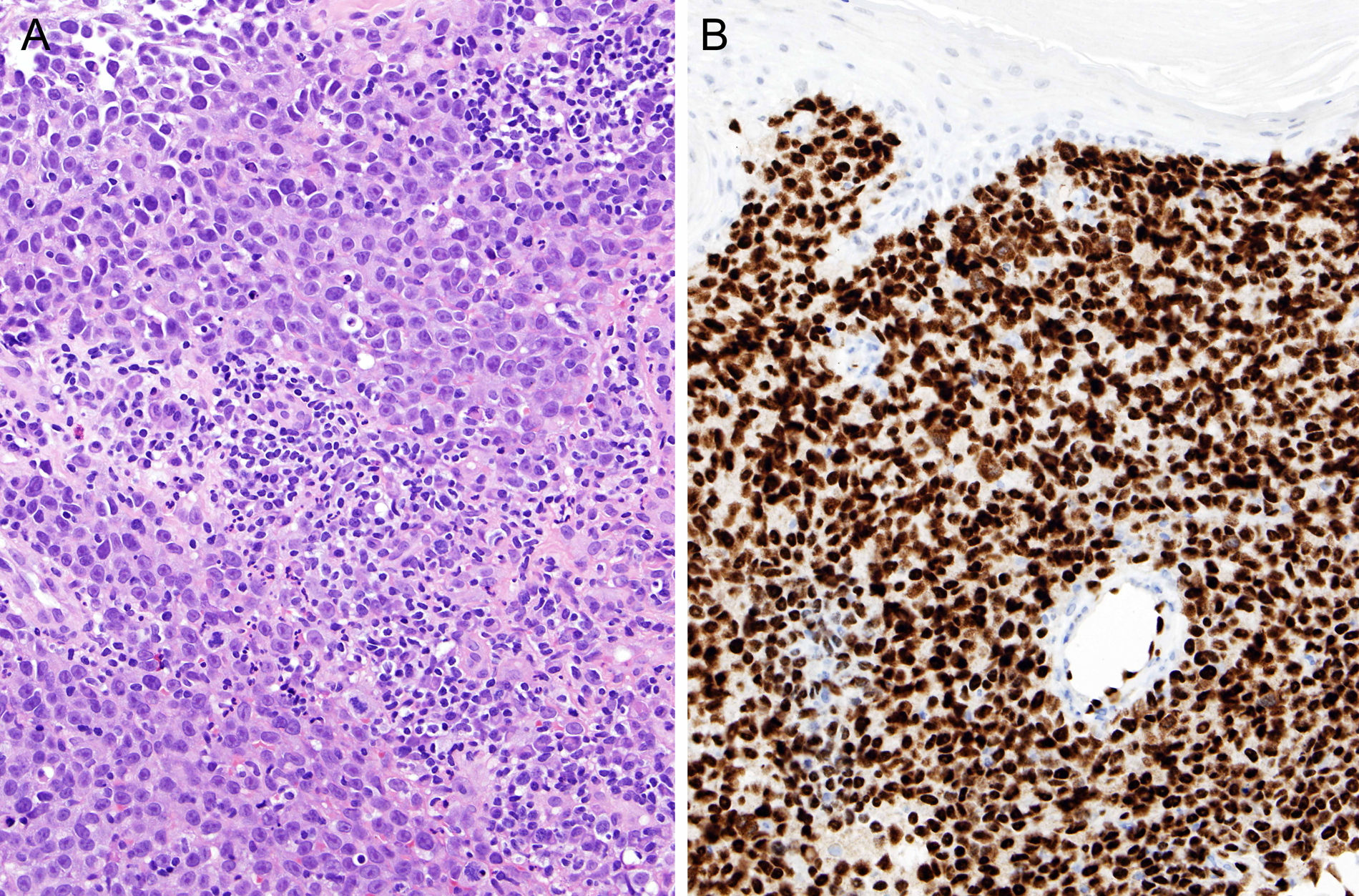
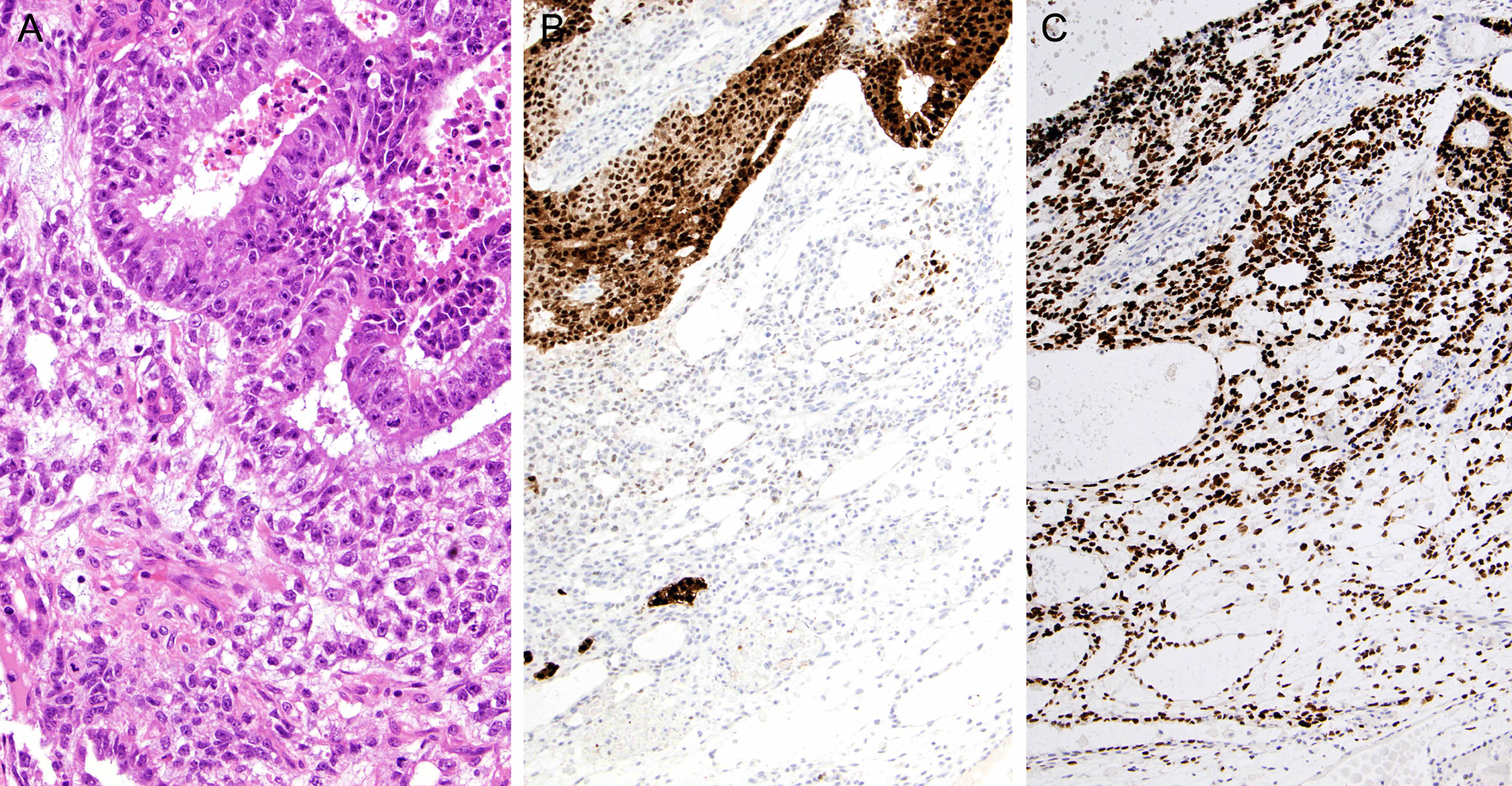
supporting a diagnosis of gynecological tract carcinoma, in the correct setting, such as distinction from mesothelioma, or confirming the ovary/endometrial origin or a metastatic adenocarcinoma (Figure 1); PAX8 is much more sensitive and more specific than WT1 and CA125;
aid in diagnosis of nephrogenic adenoma of the bladder in difficult cases; and
determining the primary site for a well-differentiated neuroendocrine tumor metastatic to the liver because ileal (PAX8 negative) and pancreatic (PAX8 positive) tumors may present as metastasis from an occult primary. 6
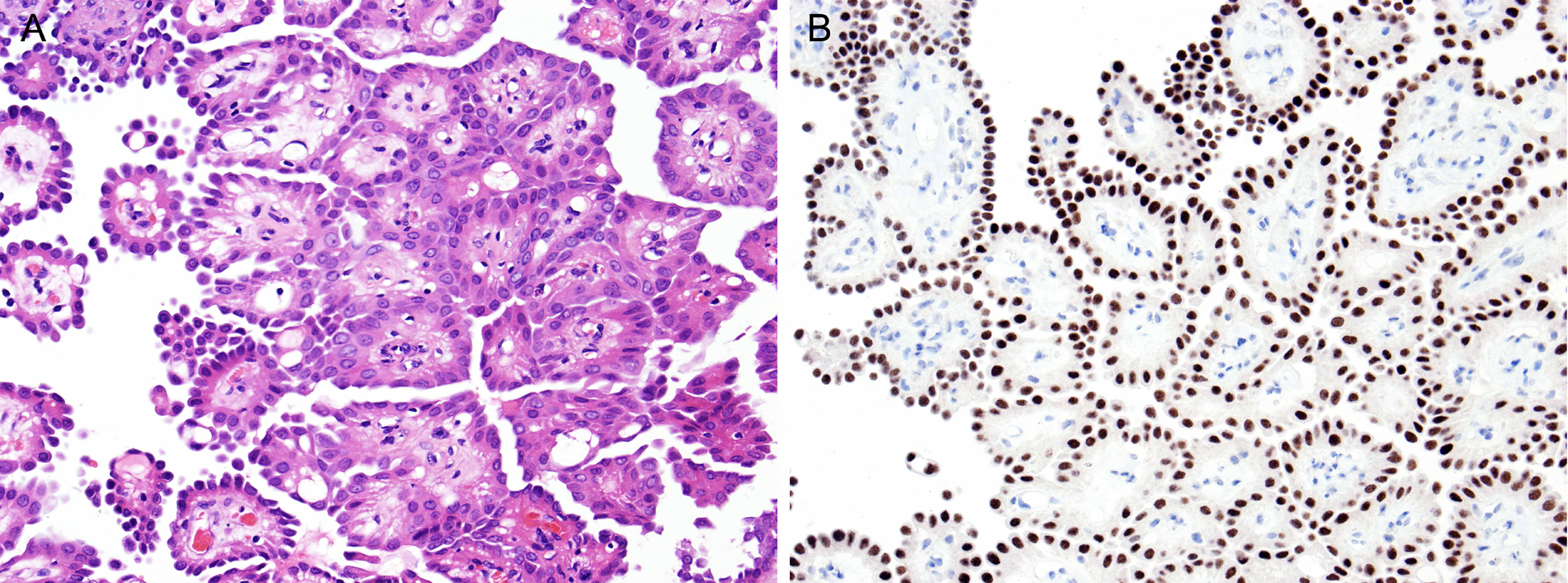
Low-grade serous carcinoma growing on the surface of the ovary: A. The papillary growth raises the differential diagnoses of adenocarcinoma and mesothelioma. B. Positive immunostaining for PAX8 (paired box gene 8) supports the diagnosis of adenocarcinoma of the female genital tract.
Napsin A
Nature of Antigen and Immunoreactivity in Normal Cells
Napsin is a pepsin-like aspartic proteinase, and Napsin A is involved in processing of pneumocyte surfactant precursors. 15 Thus, pneumocytes in the normal lung are positive in a granular cytoplasmic pattern. Alveolar macrophages are often positive because of ingestion of materials released from pneumocytes. Renal tubular epithelium is also positive for Napsin A.
Immunoreactivity in Tumors and Practical Applications
Napsin A is positive in 83% to 87% of pulmonary adenocarcinomas, compared with 60% to 73% for TTF-1 according to 3 separate studies (Figure 2).15-17 Carcinomas of other sites, with the exception of the kidney, are negative. Thus, Napsin A can be used as an alternative or additional marker for confirming the pulmonary origin of an adenocarcinoma. However, interpretation can be problematic because of diffusion of napsin A from surrounding pneumocytes or entrapment of pneumocytes, and alveolar macrophages may cause false-positive interpretation. 18
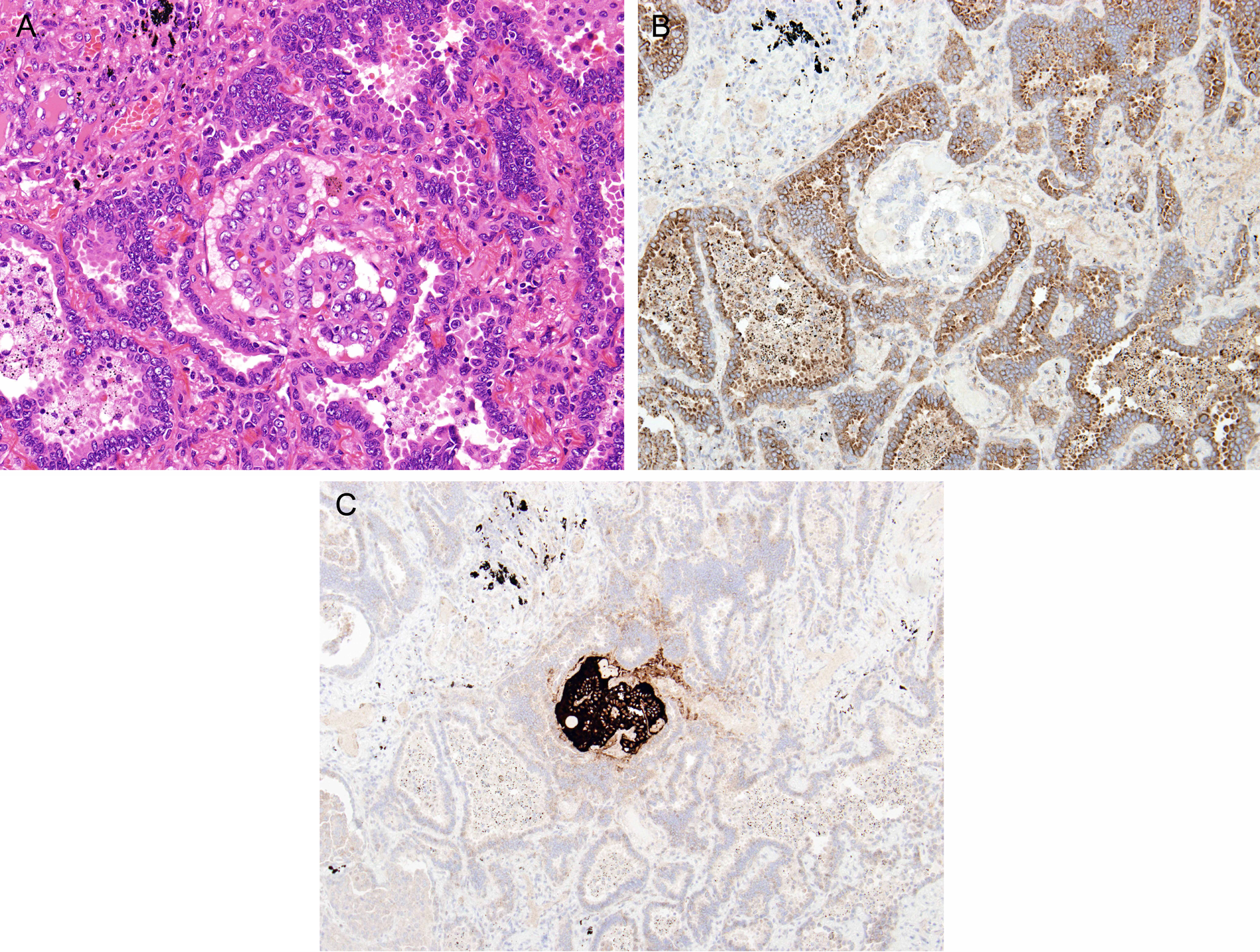
Pulmonary adenocarcinoma harboring a tiny focus of metastatic papillary thyroid carcinoma: A. In the lung, the adenocarcinoma grows in the form of irregular-shaped glands. In the central portion, there is a tiny tumor comprising papillae lined by cells with ground glass nuclei, suggestive of papillary thyroid carcinoma. Immunostaining for TTF1 (thyroid transcription factor 1) will not help in distinguishing between the 2 components, with both being expected to be positive. B. Immunostaining for Napsin A shows granular cytoplasmic staining in the pulmonary adenocarcinoma, whereas the central papillary tumor is negative. C. The tiny tumor in the center shows immunoreactivity for thyroglobulin, confirming a diagnosis of metastatic thyroid carcinoma.
Among renal tumors, napsin A is positive in most papillary renal cell carcinomas (76%-79%), 34% to 39% of clear-cell renal cell carcinomas, and only 3% of chromophobe renal cell carcinomas.15,19 Thus, napsin A immunostaining may have some value in the diagnosis of papillary renal cell carcinoma. 19
Arginase-1
Nature of Antigen and Immunoreactivity in Normal Cells
Arginase-1, also known as liver arginase, is a binuclear manganese metalloenzyme. It is a key enzyme of the urea cycle in the human liver. 20 Arginase-1 is abundantly expressed in liver cells in a nuclear cytoplasmic pattern.
Immunoreactivity in Tumors and Practical Applications
Most hepatocellular carcinomas are positive for arginase-1, whereas non–hepatocellular carcinomas are almost always negative. The advantage of arginase-1 over the traditional hepatocellular marker HEP-PAR1 (hepatocyte paraffin 1) is that the former is more sensitive and more specific and, thus, especially helpful in poorly differentiated hepatocellular carcinomas (Figure 3). According to the study of Yan et al, 20 the sensitivities of arginase-1 in well, moderately, and poorly differentiated hepatocellular carcinomas are 100%, 96%, and 86%, respectively, whereas those of HEP-PAR1 are 100%, 83%, and 46%, respectively. In scirrhous hepatocellular carcinoma, arginase-1 is also more often positive (85%) than HEP-PAR1 (26%). 21 Thus, arginase-1 is the marker of choice for demonstrating the hepatocellular origin for a carcinoma.
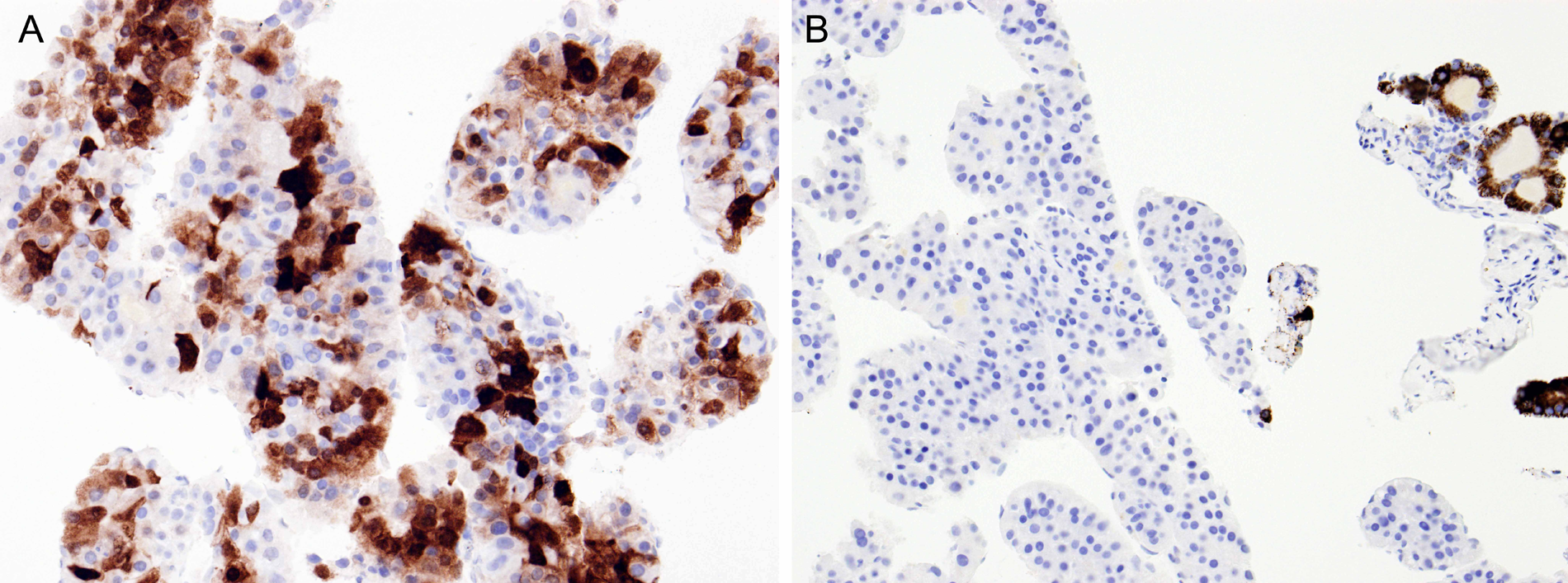
Metastatic hepatocellular carcinoma in bone, presenting as metastatic tumor of unknown primary: A. Immunostaining for arginase-1 shows that about half of the tumor cells are positive, supporting a hepatic origin of the carcinoma. B. Immunoreactivity for HEP-PAR1 (hepatocyte paraffin 1) is much more focal.
ERG (Ets-Related Gene)
Nature of Antigen and Immunoreactivity in Normal Cells
ERG, a member of the ETS family transcription factors, is constitutively expressed in endothelial cells, regulating angiogenesis and endothelial apoptosis.22,23 ERG antibody labels the nuclei of endothelial cells of blood vessels and lymphatics, whereas pericytes and vascular smooth muscle cells are negative. 23 Normal epithelial, mesenchymal (other than endothelial), neuroectodermal, and lymphoid cells are all negative. Only a subpopulation of immature myeloid cells in the marrow are ERG positive.
Immunoreactivity in Soft-Tissue Tumors and Practical Applications
Benign and malignant vascular tumors, either of blood vessel or lymphatic type, are immunoreactive for ERG in practically all cases.23-26 In the majority of cases, all neoplastic cells are labeled (Figure 4). Because other mesenchymal tumors are rarely ERG positive, ERG is a superior marker for the diagnosis of vascular tumors.23-25 In contrast to CD31, a gold standard vascular marker, ERG does not stain histiocytes and plasma cells, which can cause problems in interpretation. ERG is expressed in 38% of epithelioid sarcomas, and this can be a potential diagnostic pitfall in the differential diagnosis with epithelioid angiosarcoma. 27
Angiosarcoma of the nasal skin: A. The skin biopsy shows a poorly differentiated malignant neoplasm that may raise several differential diagnoses, such as carcinoma, melanoma, and angiosarcoma. B. Strong positive nuclear staining for ERG (Ets-related gene) supports a diagnosis of vascular neoplasm, that is, angiosarcoma. The overlying epidermis is negative for ERG, whereas the endothelial cells of an entrapped blood vessel (lower field) are positive.
Approximately 10% of cases of Ewing sarcoma are immunoreactive for ERG, an expected result because a small proportion of cases exhibit EWSR1-ERG gene fusion. 23 If an ERG antibody (EPR3864) that cross-reacts with FLI1 is used, 82% of cases are positive because Ewing sarcoma commonly shows EWSR1-FLI1 gene fusion. 28
Extramedullary myeloid sarcoma has been reported to be positive for ERG in 70% of cases. 23 This may be attributable to the presence of ERG gene fusion, as has been documented in a subset of acute myeloid leukemias, or a reflection of ERG expression in subpopulations of hematopoietic stem cells.
Immunoreactivity in Prostatic Cancer and Practical Applications
Prostate carcinoma is characterized by fusion of the ERG gene with a variety of genes, most commonly androgen-regulated transmembrane protease serine 2 (TMPRSS2) gene in approximately half of all cases. The gene fusion results in expression of an TMPRSS2-ERG oncoprotein. On immunostaining, 33% to 61% of all prostatic carcinomas are shown to be immunoreactive for ERG (Figure 5).23,24,26,29-33 When positive, practically all neoplastic cells are labeled strongly. There is excellent correlation of ERG immunohistochemistry with presence of ERG gene fusion.31,32,34 In high-grade prostatic intraepithelial neoplasia, ERG is positive in approximately 20% of cases. Carcinomas of other anatomical sites are negative for ERG with rare exceptions, and the staining is often focal in such cases. 26
Immunostaining for ERG (Ets-related gene) in the prostate: A. In the normal prostate, the prostatic epithelium is negative for ERG. The positive cells represent endothelial cells. B. Prostatic adenocarcinoma showing nuclear immunoreactivity for ERG, indicating presence of ERG gene fusion.
Thus, ERG immunohistochemistry is a valuable tool for diagnosis of limited prostate carcinoma in biopsies. 26 This assay is of moderate sensitivity but high specificity. Also, given the lack of ERG expression in a wide variety of tumors and its robust presence in prostatic carcinoma, ERG immunohistochemistry is of value for determining the prostatic origin of metastatic adenocarcinoma of unknown primary. 27
SOX10 (SRY-Related HMG Box 10)
Nature of Antigen and Immunoreactivity in Normal Cells
SOX10 is a transcription factor essential for the generation of neural crest cells, their survival, and maintenance of pluripotency. 35 Immunostaining for SOX10 shows nuclear localization. Normally, SOX10 is expressed in (1) melanocytes, (2) Schwann cells, (3) oligodendrocytes, (4) myoepithelial cells of mucosal glands and the breast, and (5) acinar cells and myoepithelial cells of the acini and intercalated ducts in the salivary gland (Figure 6).35-38 SOX10 expression is also observed in mast cells in both the nuclei and cytoplasm.
SOX10 (SRY-related HMG box 10) immunohistochemistry: (A, B) desmoplastic melanoma. A. Atypical spindly tumor cells are admixed with collagen. B, The tumor cells show extensive nuclear staining for SOX10, supporting a diagnosis of melanoma. C. Sentinel lymph node from a patient with melanoma. A few single atypical cells are highlighted. Such cells are likely to be missed in an S100 immunostain. D. In the normal parotid gland, the acinar and intercalated duct cells show nuclear staining for SOX10, whereas the striated duct cells are negative.
Immunoreactivity in Tumors and Practical Applications
SOX10 is reported to be positive in the following tumor types35-37,39:
Melanocytic tumors
40
:
melanocytic nevi are all positive; almost all melanomas are positive, including desmoplastic melanoma (78%-100% of cases, with the percentage of positive cells being lower than in conventional melanoma);
Schwann cell tumors:
Schwannoma Neurofibroma Granular cell tumor Malignant peripheral nerve sheath tumor (27%-50% of cases)
Clear cell sarcoma of soft tissue.
Brain: astrocytic and oligodendroglial tumors; primitive neuroectodermal tumor.
Breast: triple-negative and metaplastic carcinomas are commonly positive (66%).39,41
Salivary gland: SOX10 is expressed in almost all cases of adenoid cystic carcinoma, acinic cell carcinoma, epithelial-myoepithelial carcinoma, carcinoma ex pleomorphic adenoma, myoepithelioma, and myoepithelial carcinoma. 38 Both luminal and abluminal cells are stained up for tumors with dual cell differentiation. Salivary duct carcinoma, mucoepidermoid carcinoma, oncocytoma, oncocytic carcinoma, and Warthin tumor are negative.
Sustentacular cells of pheochromocytoma, paraganglioma, and pulmonary carcinoid. 42
Carcinomas of the various anatomical sites (other than the breast) and angiomyolipomas are usually negative.
The major diagnostic applications are as follows:
Distinction of melanoma from its mimickers can be made using SOX10 as an alternative or principal immunohistochemical marker. SOX10 is particularly helpful for distinction of melanoma cells (SOX10+) from heavily melanin-laden macrophages (SOX10−) because interpretation is facilitated by the nuclear staining and because positive staining for SOX10 is extensive, whereas staining for other melanocytic-associated markers is not uncommonly patchy.
It aids in diagnosis of desmoplastic melanoma, which is often positive for SOX10 but infrequently positive for other melanocytic-associated markers (Figures 6A and 6B).
This is the antibody of choice for the assessment of sentinel lymph nodes resected from patients with melanoma for micrometastases because all tumor cells are expected to be positive and not affected by the presence of cytoplasmic pigment. Immunostaining for SOX10 is much easier to interpret than S100 protein (Figure 6C) because S100+ nodal dendritic cells may mask isolated melanoma cells.43,44
It aids in diagnosis of malignant peripheral nerve sheath tumor, with SOX10 being more sensitive and more specific than S100 protein. 35
DOG1 (Discovered on GIST 1)
Nature of Antigen and Immunoreactivity in Normal Cells
DOG1 (anoctamin-1 or TMEM16a), a calcium-activated chloride channel protein, was originally discovered in gene expression profiling studies on gastrointestinal stromal tumors (GISTs; Figure 7A). 45 Subsequently, antibodies have been produced against DOG1 for immunohistochemical diagnosis of GISTs.
DOG1 immunohistochemistry in a gastrointestinal stromal tumor: A. Usual gastrointestinal stromal tumors showing strong staining, predominantly in a cell membrane pattern. (B-D) Needle biopsy of intra-abdominal epithelioid gastrointestinal stromal tumor. B. The biopsy shows tumor cells with epithelioid morphology. C. Few cells show KIT immunoreactivity, rendering a diagnosis of gastrointestinal stromal tumor not that secure. D. Extensive positive staining for DOG1 supports the diagnosis.
DOG1 is normally expressed in interstitial cells of Cajal of the gastrointestinal tract. 46 Luminal surface staining is also present in the gastric mucosa, pancreatic centroacinar cells, intrahepatic bile duct, gall bladder, and bladder urothelium. 46 In the salivary gland, DOG1 is expressed in the apical cell membranes of acinar cells (being stronger in serous than mucinous cells) and intercalated duct cells (Figure 8A). Myoepithelial cells, striated ducts, and excretory ducts are negative. 47
DOG1 immunohistochemistry of the salivary gland: A. In the normal salivary gland, DOG1 immunostaining is seen in the apical membranes of the acini, resulting in a distinctive canalicular pattern. The intercalated ducts are also positive, whereas striated ducts are negative. (B, C) Oral acinic cell carcinoma. B. The tumor grows in the form of columns, accompanied by a prominent vasculature. Basophilic granules are not seen. C. The canalicular pattern of staining for DOG1, highlighting subtle lumens, recapitulates the pattern seen in normal salivary acini.
Immunoreactivity in GIST and Practical Applications
DOG1 is a sensitive and specific marker for GISTs, being positive in about 95% of cases, a positivity rate similar to KIT/CD117.46,48,49 The staining for DOG1 is cytoplasmic and/or membranous and is usually extensive and strong (Figure 7A). In all, 36% to 46% of KIT-negative cases are DOG1 positive, whereas 50% of DOG1-negative cases are KIT positive.46,50 DOG1 can identify a significant proportion of GISTs with PDGFRA mutation and those lacking both KIT and PDGFRA mutations.45,48,50,51
Non-GIST mesenchymal tumors are generally DOG1 negative. Exceptions are leiomyomatosis peritonealis, leiomyoma of uterine type, and synovial sarcoma, which can sometimes be DOG1 positive.46,48 Among epithelial tumors, gastric, esophageal, colonic, and endometrial carcinomas are occasionally positive.46,52
Therefore, DOG1 is a sensitive immunohistochemical marker for GIST. It can be used as a backup antibody if GIST is suspected but KIT staining is negative or equivocal or if KIT is positive but other differential diagnoses are also being considered (Figure 7).
Immunoreactivity in Salivary Gland Tumors and Practical Applications
Among salivary gland tumors, acinic cell carcinomas are consistently DOG1 positive, with a complex mixture of intense apical membranous, cytoplasmic, and complete membranous staining (Figures 8B and 8C). 47 Mammary analogue secretory carcinoma is positive in one-third of cases. Adenoid cystic carcinomas and epithelial-myoepithelial carcinomas are often positive, with a combined apical ductal and membranous/cytoplasmic myoepithelial staining profile. 47 Pleomorphic adenoma, myoepithelial neoplasms, Warthin tumor, mucoepidermoid carcinoma, salivary duct carcinoma, polymorphous low-grade adenocarcinoma, and oncocytic neoplasms are usually negative.
Thus, in the context of appropriate morphological differential diagnoses, DOG1 is valuable for supporting a diagnosis of acinic cell carcinoma, which otherwise lacks diagnostic immunohistochemical markers (Figure 8).
OCT3/4 and SALL4
Nature of Antigen and Immunoreactivity in Normal Cells
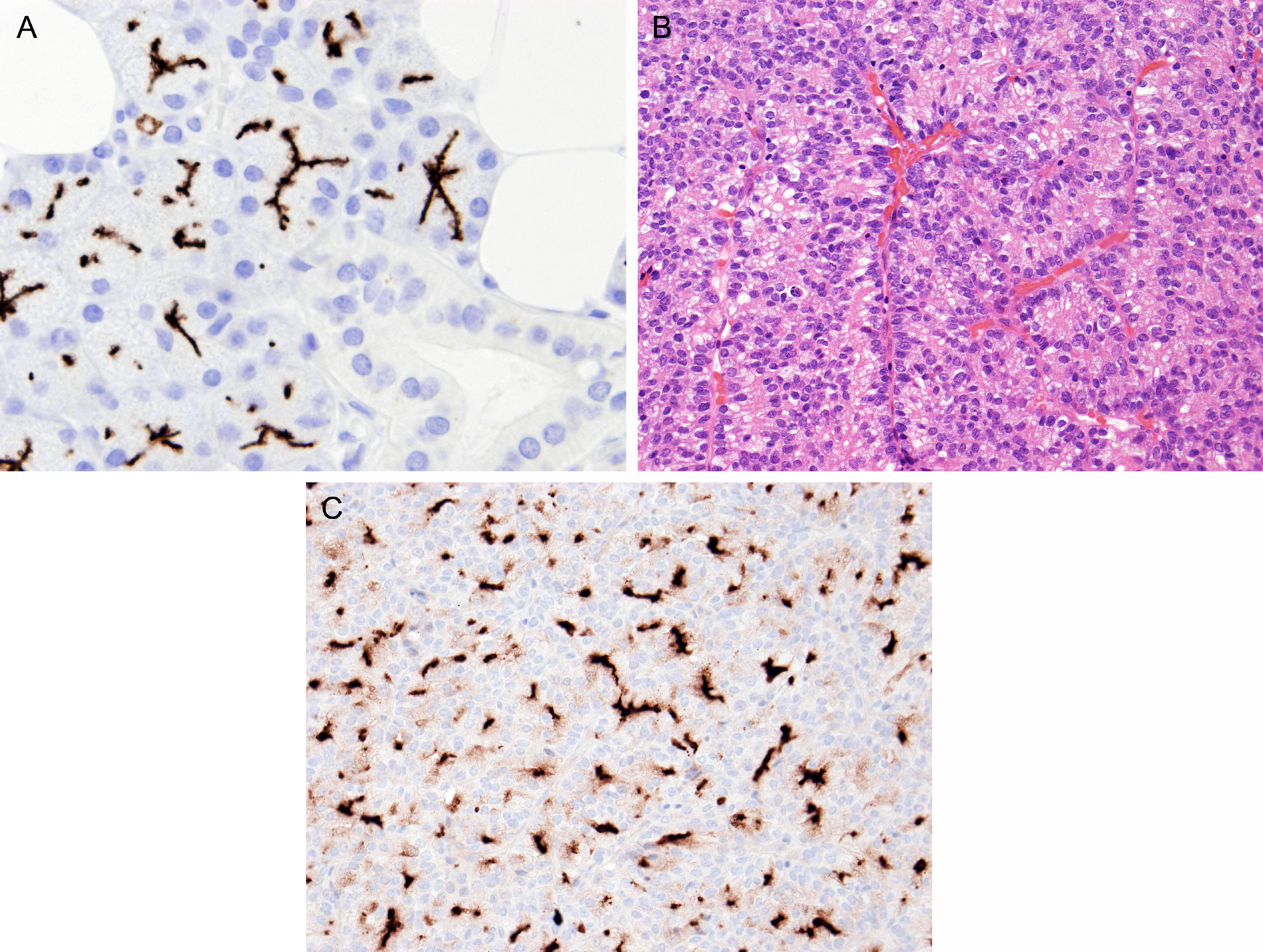
OCT3/4, also known as OCT3 or OCT4, is a mammalian POU (Pit-Oct-Unc) transcription factor that is expressed in undifferentiated, pluripotent cells, including embryonic stem cells and germ cells. The normal germ cells in the testis and ovary are negative (Table 2). 53
Immunoreactivity of Normal Germ Cells and Intratubular Germ Cell Neoplasia for “Germ Cell Markers.”
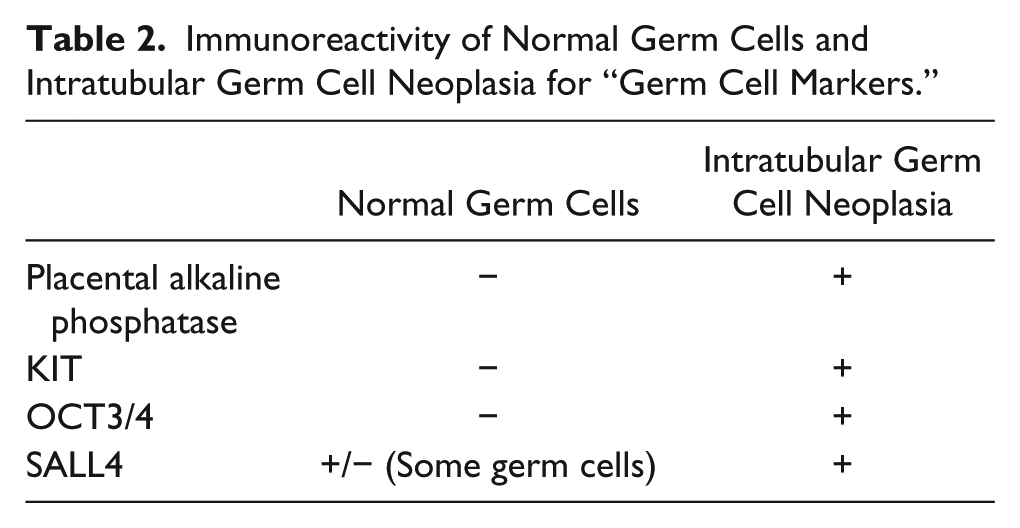
SALL4 is a zinc finger transcription factor in the same family as OCT3/4, being involved in the maintenance of self-renewal and pluripotency of embryonic stem cells. It regulates transcription of OCT3/4. SALL4 is normally expressed in subpopulations of germ cells (Table 2). 54 SALL4 expression is also observed in the neofetal stomach in gestational week 9 and disappears thereafter. 55
Immunoreactivity in Tumors and Practical Applications
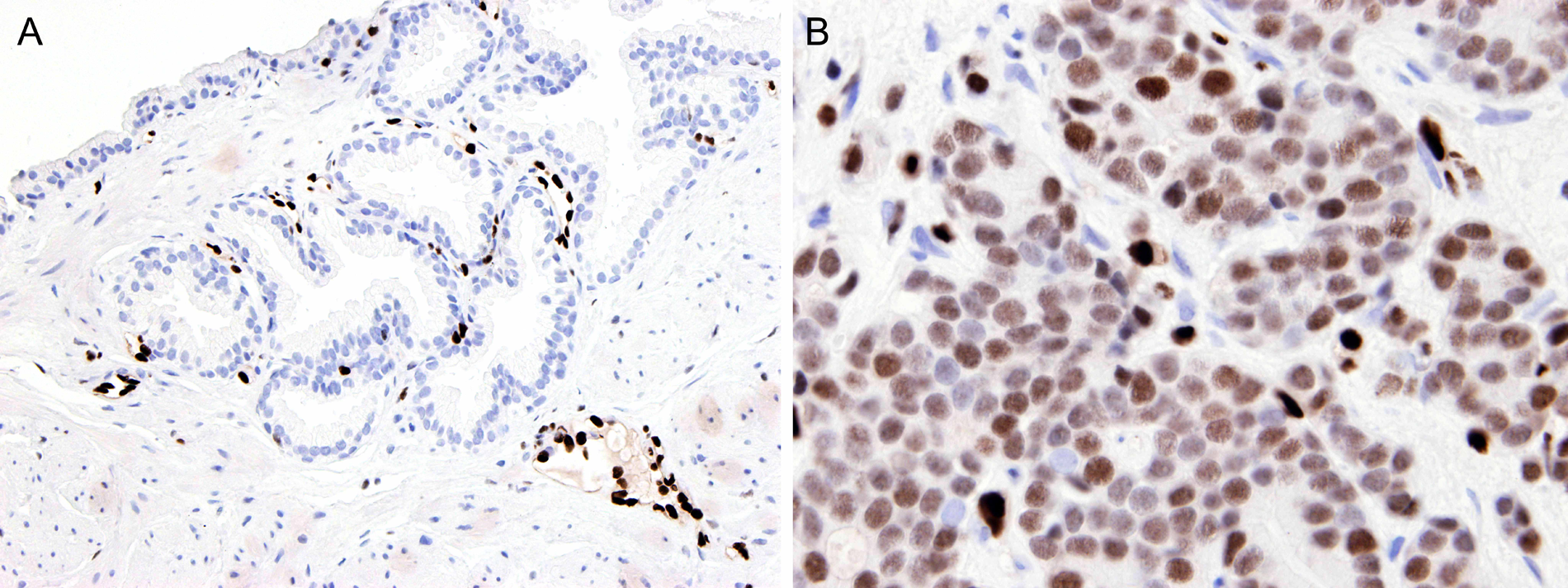
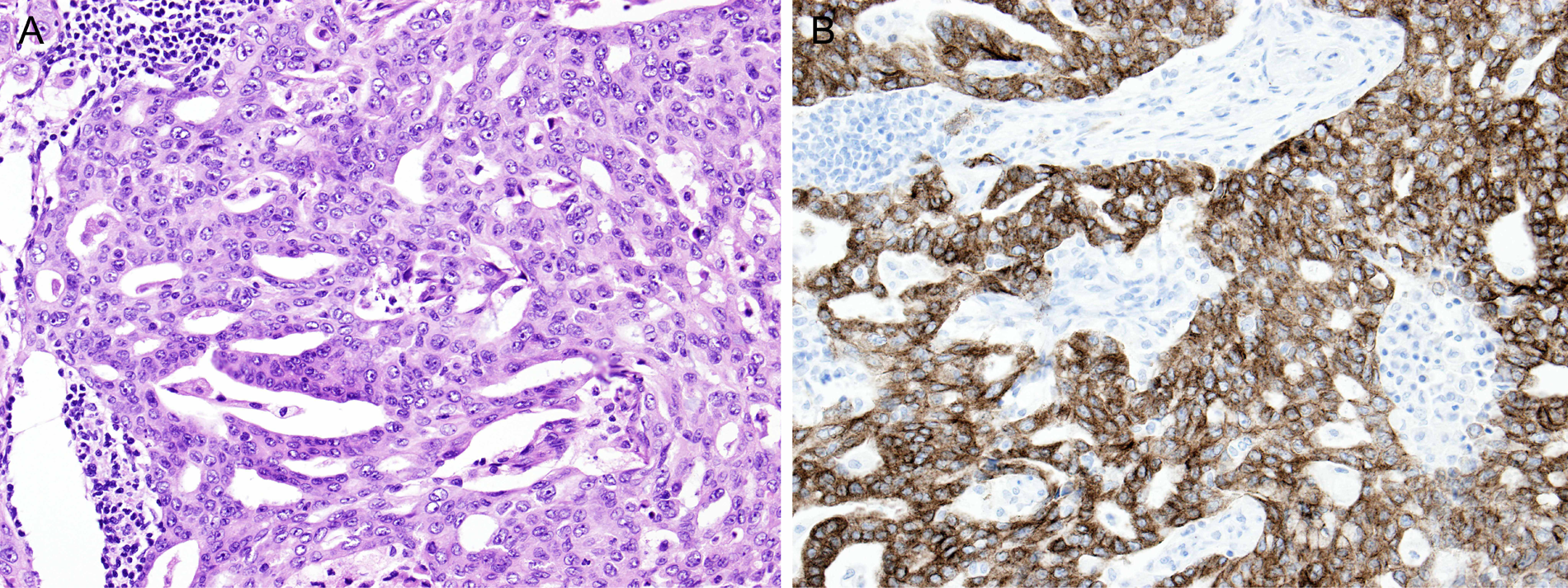
Staining for OCT3/4 and SALL4 occurs in the nuclei. The pattern of immunoreactivities in germ cell tumors is shown in Figure 9 and Table 2.53,54,56-60 OCT3/4 is positive in seminoma and embryonal carcinoma but not in yolk sac tumor, whereas SALL4 is positive in all 3 types of germ cell tumors (Figure 10). An OCT3/4− SALL4+ immunophenotype is highly distinctive of yolk sac tumor, which previously did not have reliable immunohistochemical markers; α-fetoprotein is of limited sensitivity and specificity, and glypican-3 is of high sensitivity but low specificity. 61
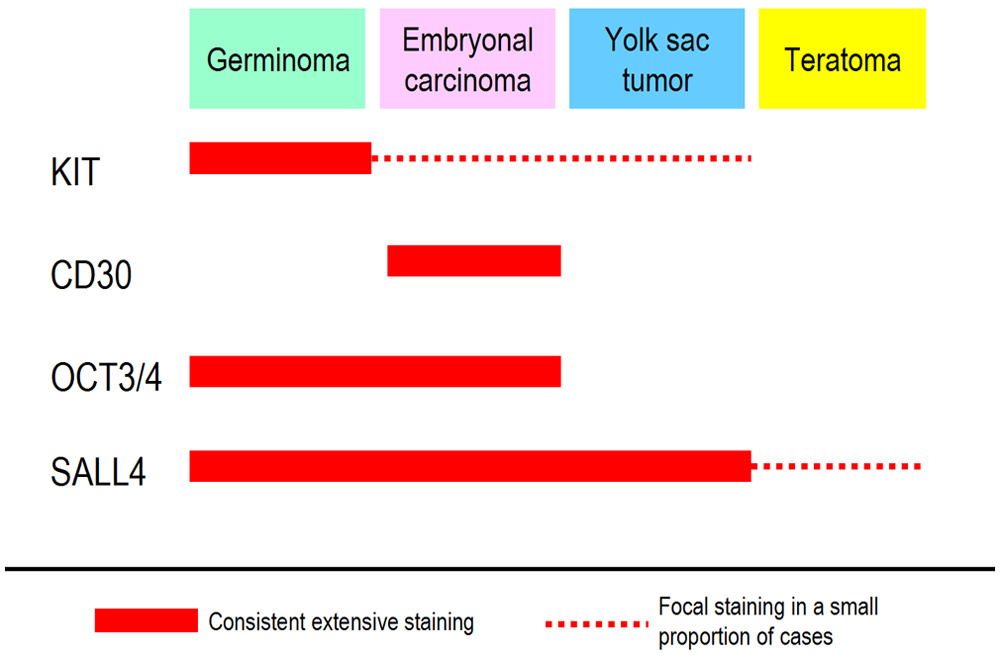
Immunoreactivities of various types of germ cell tumors for KIT, CD30, OCT3/4, and SALL4.
Testicular germ cell tumor: A. Upper field shows embryonal carcinoma with overlapping nuclei. The lower field shows yolk sac tumor, comprising cells with smaller nuclei, growing in a reticulated pattern. B. Embryonal carcinoma is positive for OCT3/4, whereas yolk sac tumor is negative. C. Both embryonal carcinoma and yolk sac tumor are positive for SALL4.
Somatic carcinomas, with rare exceptions, are negative for OCT3/4 and SALL4. SALL4 is positive in α-fetoprotein-producing gastric carcinomas, and this can be utilized to distinguish this tumor type from hepatocellular carcinoma. 55
Thus, OCT3/4 and SALL4 are excellent pan–germ cell tumor markers and should replace the traditional germ cell marker placental alkaline phosphatase, which lacks specificity and sensitivity. 62
MUC4 (Mucin-Related Antigen 4)
Nature of Antigen and Immunoreactivity in Normal Cells
MUC4 (mucin-related antigen 4) is a transmembrane glycoprotein that functions in the cell growth signaling pathway. It is normally expressed in various epithelial tissues of endodermic origin, such as bronchus and intestines. MUC4 is also positive in the trophoblastic cells of the trophoblastic columns and implantation site. 63
Aid in Diagnosis of Low-Grade Fibromyxoid Sarcoma (LGFMS) and Sclerosing Epithelioid Fibrosarcoma
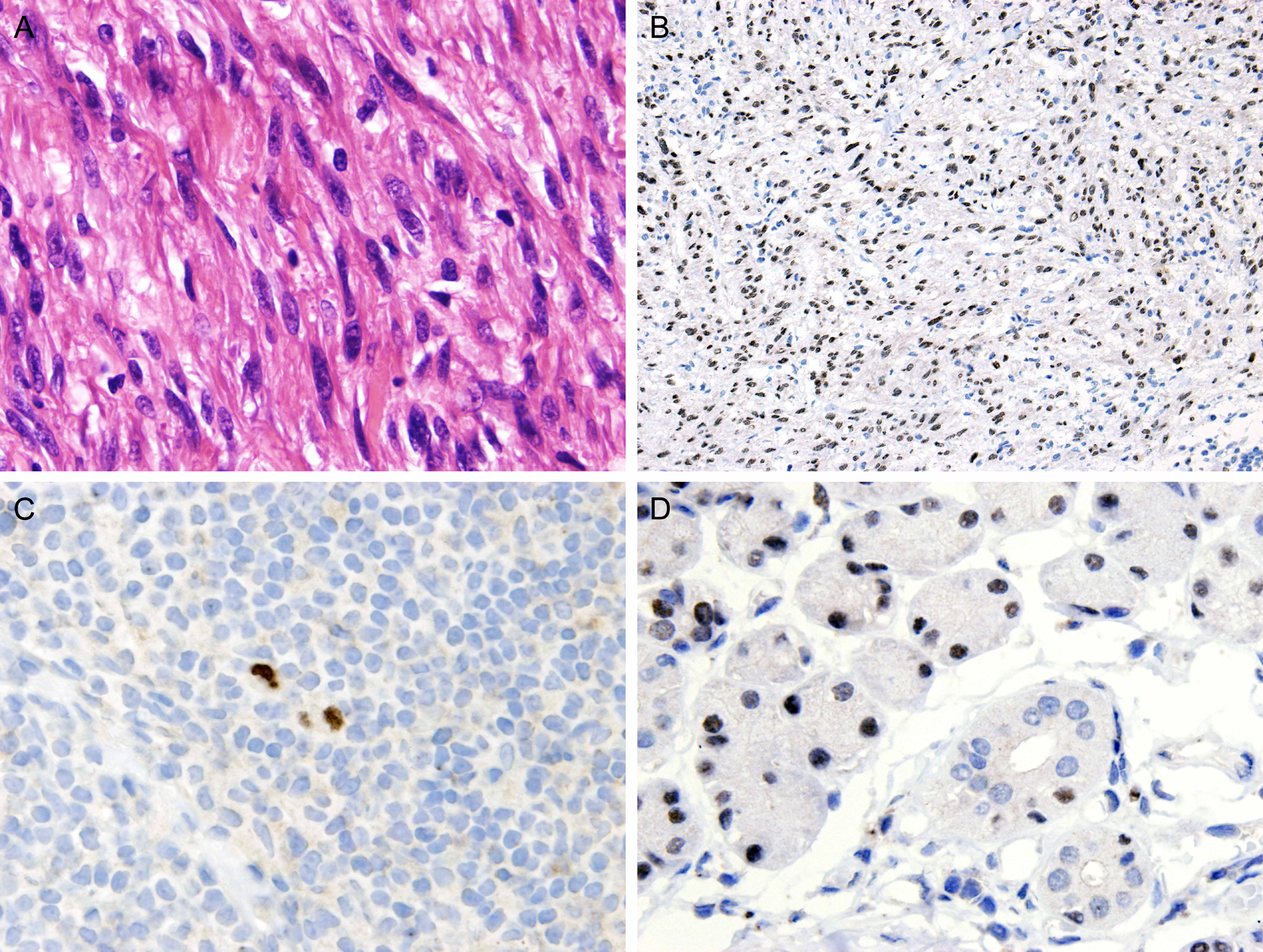
LGFMS is a deceptively bland-looking fibroblastic neoplasm that is difficult to distinguish from benign mesenchymal tumors and other low-grade sarcomas. Difficulties in diagnosis are compounded by a lack of distinctive immunohistochemical markers. Inspired by the finding of marked differential upregulation of the MUC4 gene in LGFMS on gene expression profiling, the study of Doyle et al 64 confirmed the high sensitivity and specificity of immunostaining for MUC4 in the diagnosis of LGFMS. All LGFMS cases show cytoplasmic staining, usually diffuse and intense (Figure 11), whereas all other tumor mimickers are negative, except in 30% of cases of monophasic synovial sarcoma.
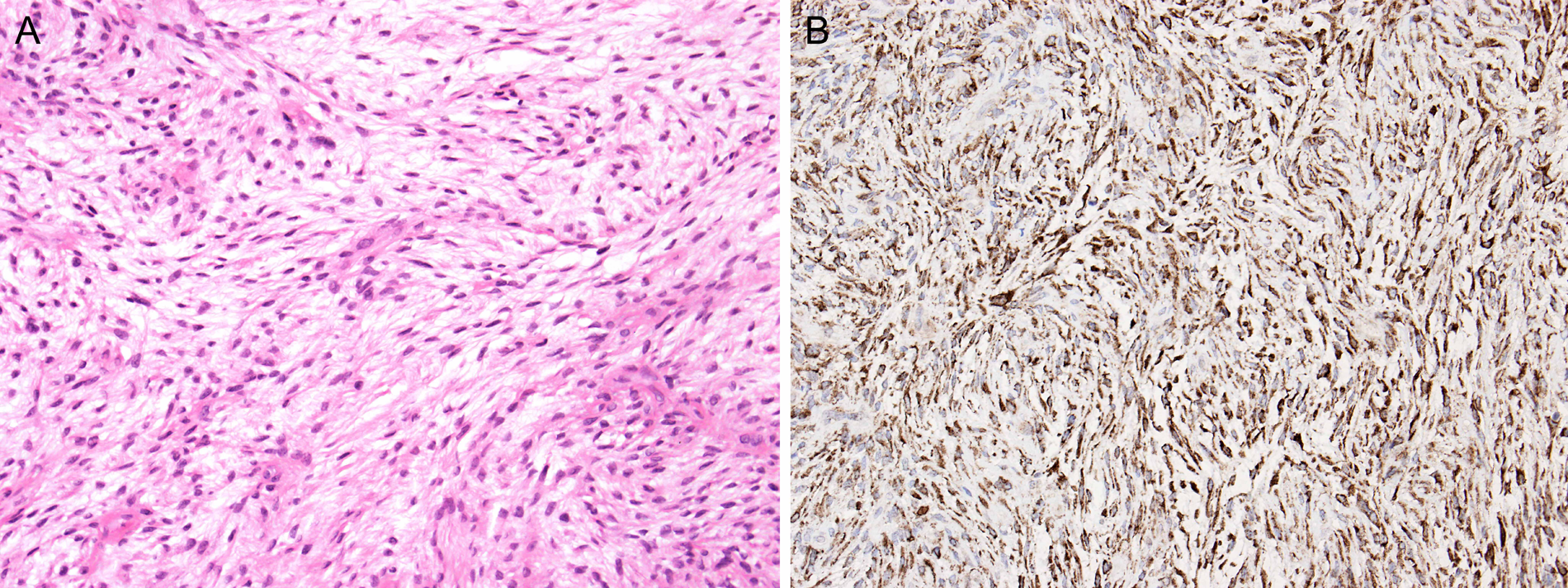
Low-grade fibromyxoid sarcoma of soft tissue: A. The tumor comprises bland-looking spindly cells with relatively low cellularity, making one reluctant to render a diagnosis of malignancy. B. Extensive positive staining for MUC4 (mucin-related antigen 4) supports the diagnosis.
Sclerosing epithelioid fibrosarcoma, which shows morphological and molecular overlap with LGFMS, similarly shows a high frequency of MUC4 expression (78% of cases).
Other Potential Applications
Because pulmonary adenocarcinoma is often positive for MUC4 (91%), whereas mesothelioma is consistently negative, immunostaining for MUC4 is of help in the differential diagnosis between these 2 entities. 65
Because MUC4 is expressed in adenocarcinomas from a variety of anatomical sites, it does not have value in suggesting a likely primary site. Nonetheless, expression of MUC4 in carcinomas appears to be associated with a worse clinical outcome.
In the assessment of uterine curettings in which chorionic villi are not found but pregnancy is suspected, MUC4 is a valuable marker for highlighting implantation site trophoblasts (MUC4+). The presence of trophoblastic cells indicates intrauterine pregnancy, rendering ectopic pregnancy most unlikely.
Langerin
Nature of Antigen and Immunoreactivity in Normal Cells
Langerin (CD207) is a type II transmembrane C-type lectin associated with the formation of Birbeck granules in Langerhans cells. On immunostaining, the normal Langerhans cells show a coarsely granular cell membrane and/or cytoplasmic staining. 66 Some sinusoid-lining cells of the lymph node and liver also label for langerin, but these cells are negative for CD1a. 66
Immunoreactivity in Tumors and Practical Applications
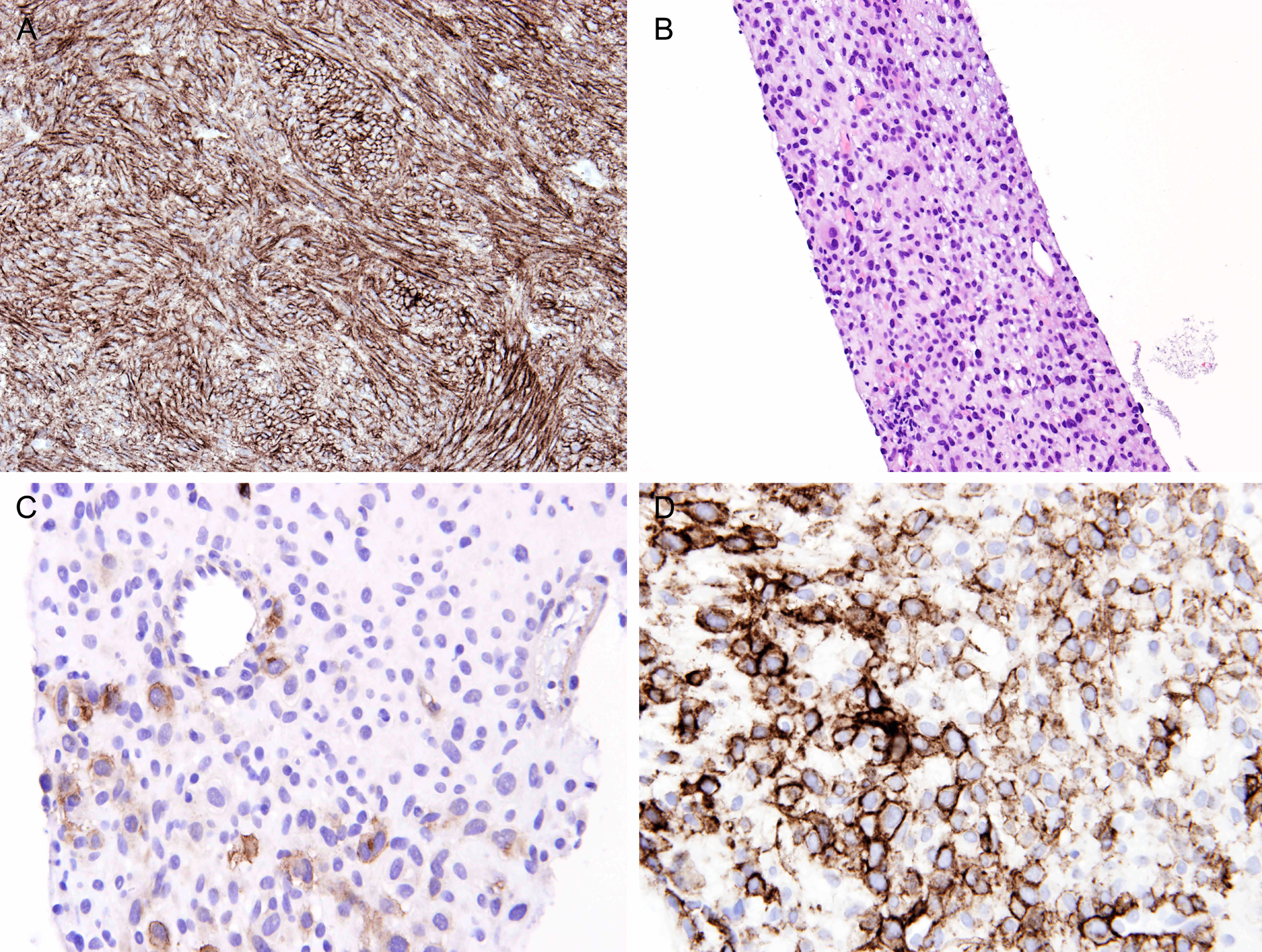
Langerin, being consistently positive in Langerhans cell histiocytosis/sarcoma and negative in other types of histiocytosis, can serve as a defining immunohistochemical marker of Langerhans cell neoplasms.66,67 An immunophenotype of S100+ CD1a+ langerin+ distinguishes Langerhans cell neoplasms from indeterminate dendritic cell neoplasms (S100+ CD1a+ langerin−). 68
SOX11 (SRY-Related HMG Box 11)
Nature of Antigen and Immunoreactivity in Normal Cells
SOX11 is a neural transcription factor belonging to subgroup C of the SOX gene family. It shows significant homology with SOX4, which is a transcription factor in B- and T-lymphoid cells and crucial for B lymphopoiesis. 69 SOX11 has no known lymphopoeitic function and is not expressed in B-cells. 69
Only nuclear immunostaining for SOX11 is considered genuine staining. There are no positive cells in the normal lymph node, although some follicular center cells can show nonspecific cytoplasmic staining.69,72 Nuclear staining is found in Schwann cells and squamous cells (such as tonsillar epithelium), whereas other tissues, including bone marrow and brain, are negative for SOX11. 69
Immunoreactivity in Tumors and Practical Applications
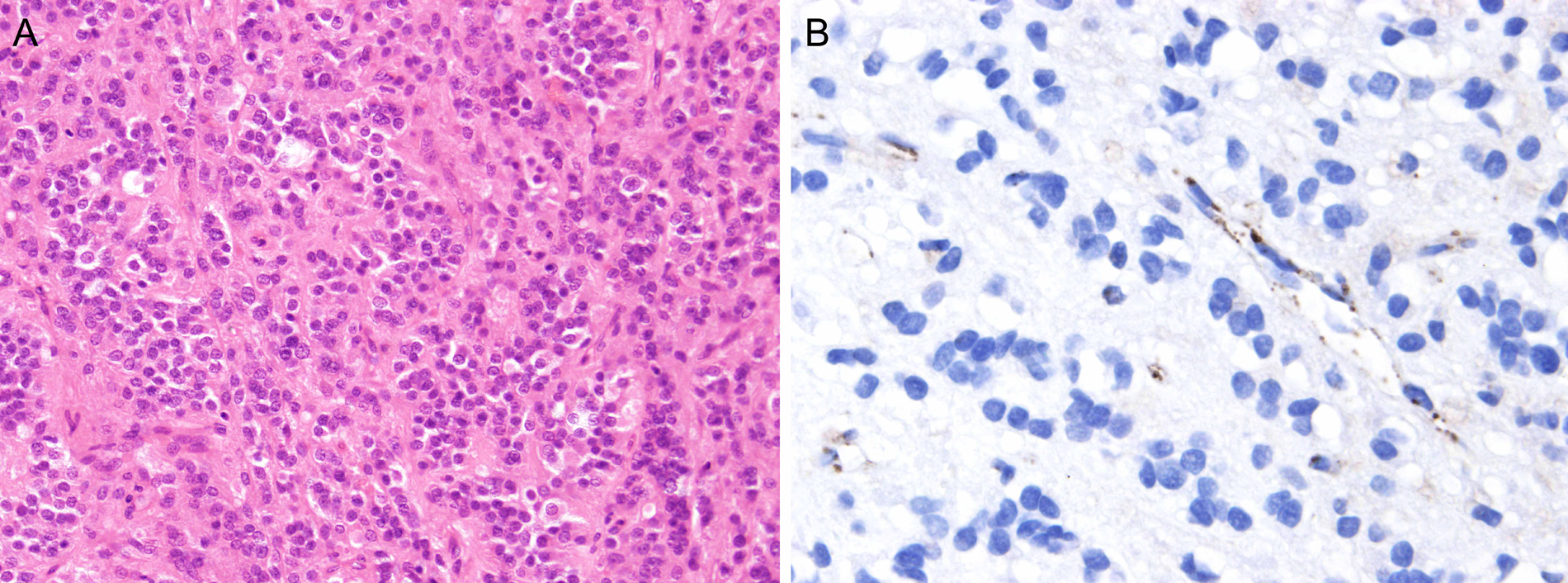
Mantle cell lymphomas are positive for SOX11 in 93% to 100% of cases (Figure 12).69-72 Other lymphoma types are negative, except lymphoblastic lymphoma of B or T lineage (100%), T-cell prolymphocytic leukemia (66%), and Burkitt lymphoma (25%-50%).70,71,73 Although up to 50% of cases of hairy cell leukemia have been reported to be positive for SOX11, 71 this finding cannot be confirmed when the newly available monoclonal antibody against SOX11 is used (SOX11-C1). 72 In the rare cases of diffuse large-B-cell lymphomas that express cyclin D1, SOX11 is negative. 74
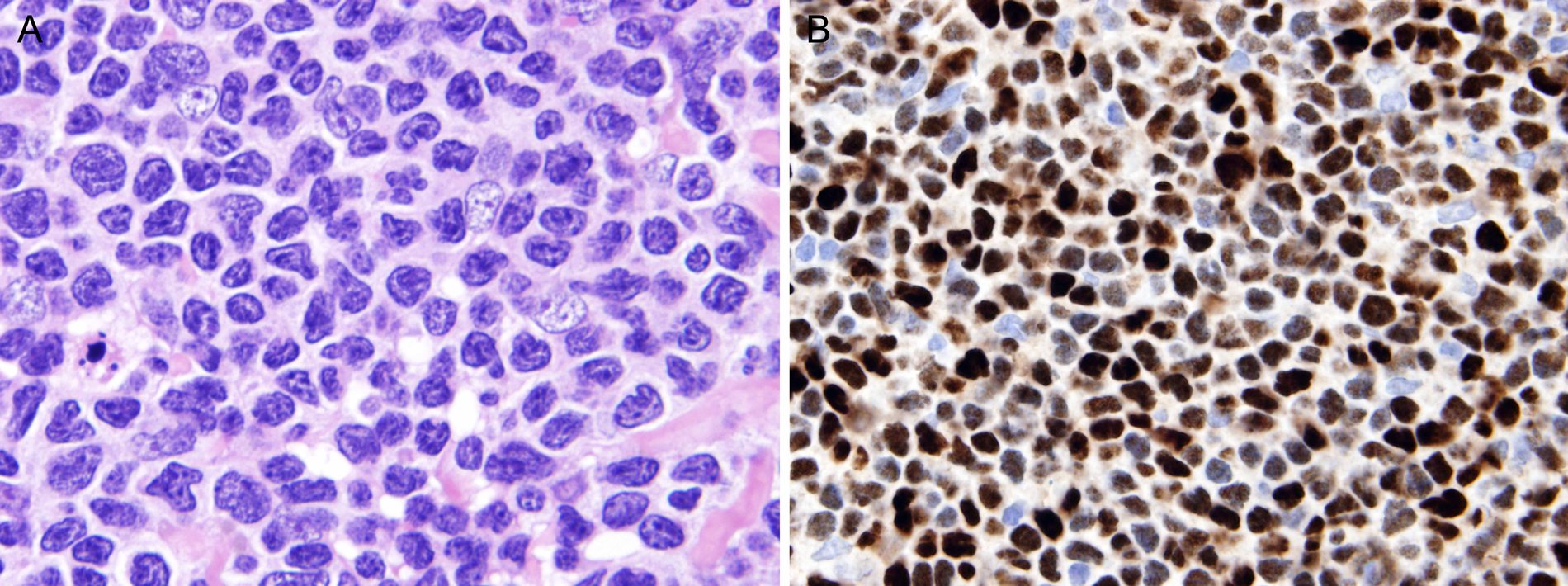
Mantle cell lymphoma and SOX11 (SRY-related HMG box 11). A. Mantle cell lymphoma comprising small cells with irregularly folded nuclei and dense chromatin. B. The tumor cells show extensive nuclear staining for SOX11.
Approximately 5% of all mantle cell lymphomas are cyclin D1 negative. These cases are difficult to diagnose because of marked morphological and immunophenotypic overlap with other low-grade B-cell lymphomas. Because practically all such cases strongly express SOX11, this immunostain is valuable for confirmation of the diagnosis of mantle cell lymphoma. 70 Thus, SOX11 antibody can be added to the routine antibody panel for investigation of lymphomas (which may help detect unsuspected cases of blastoid variants of mantle cell lymphoma) or can be reserved for investigation of problematic cases, such as cyclin D1+ or CD5+ diffuse large-B-cell lymphomas versus mantle cell lymphoma.
Treponema pallidum
Nature of Antigen and Practical Applications
Treponema pallidum is the causative agent of syphilis. It used to be demonstrated in tissue sections by silver stains such as Steiner’s and Warthin-Starry, but these stains are fastidious, and interpretation is not always easy because of the presence of silver deposits in the background. T pallidum can now be successfully demonstrated by immunohistochemistry using a polyclonal antiserum (specific for T pallidum, except for cross-reaction with Borrelia burgdoferi). This is a great advantage because the spirochetes are easily visualized in a clean background. 75 The spirochetes are quite large and show a spiral morphology (Figures 13A and 13B). 76 Sometimes they can appear fragmented, in which circumstance, the spirochetes would be impossible to identify with confidence in conventional silver stains (Figures 13C and 13D).
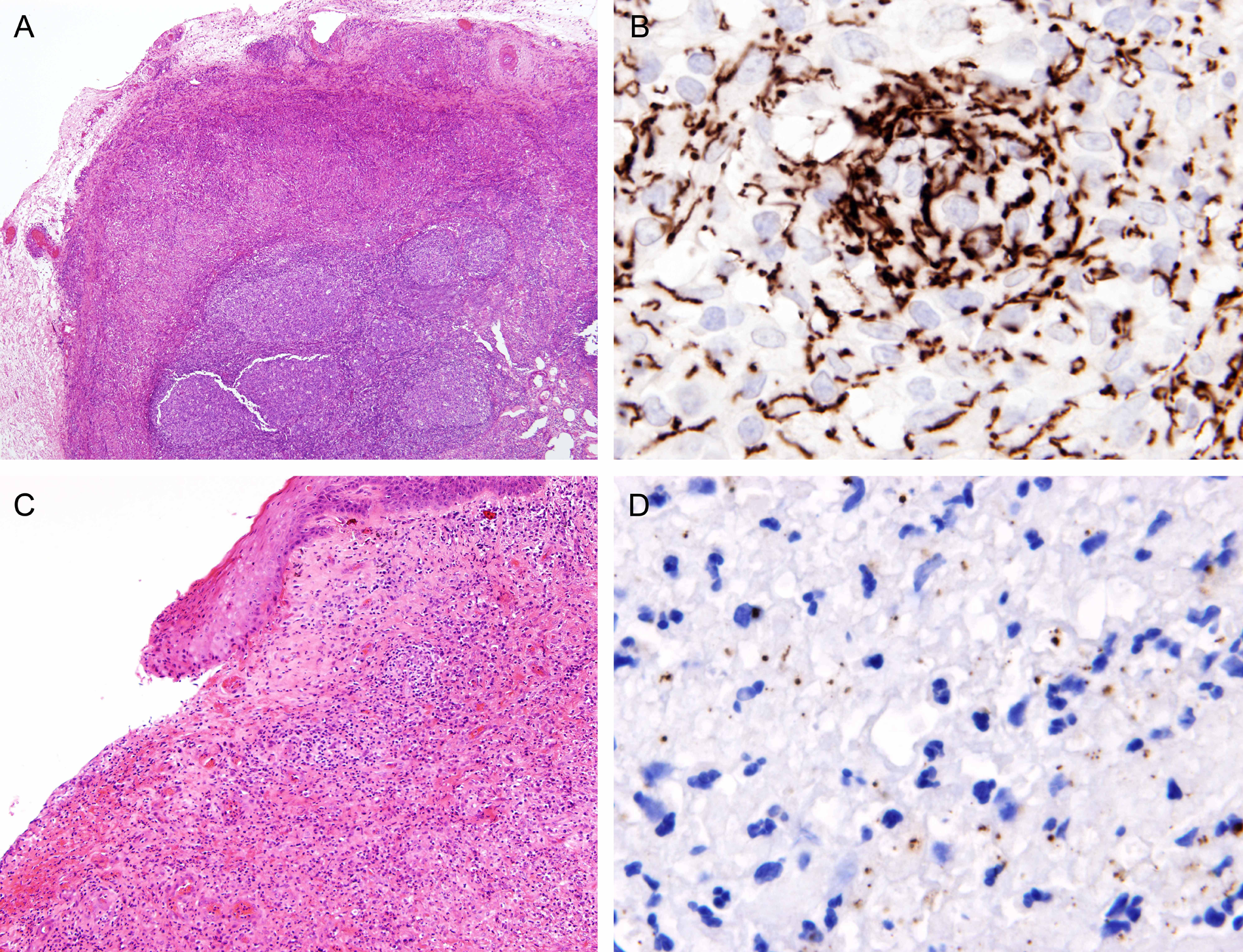
Immunostaining for Treponema pallidum. (A, B) Syphilitic lymphadenitis. A. Lymph node shows reactive follicular hyperplasia. The capsule is markedly thickened, resulting in an inflammatory pseudotumor-like morphology. B. Immunostaining for T pallidum reveals numerous spirochetes, supporting a diagnosis of syphilis. (C, D) Syphilitic chancre of the penis. C. The biopsy shows ulcerated tissue with chronic inflammatory cell infiltration. D. Immunostaining for T pallidum reveals fragmented bacteria. There are only rare intact spirochetes.
SV40 (Simian Virus 40)
Nature of Antigen and Practical Applications
A paraffin section–reactive antibody against the large-T antigen of the SV40 polyomavirus has become commercially available. This is valuable in surgical pathology diagnosis because it can be utilized for its cross-reaction with the large-T antigen of the BK and JC polyomavirus.77,78
The anti-SV40 antibody is applicable for diagnosis of BK virus infection of the urinary tract, in kidney or urine specimens. It can also be used in the diagnosis of progressive multifocal leukoencephalopathy (caused by JC virus infection); the number of labeled cells is usually much greater than cells with recognizable nuclear inclusions (Figure 14). Thus, the diagnosis is facilitated, particularly in small biopsies.
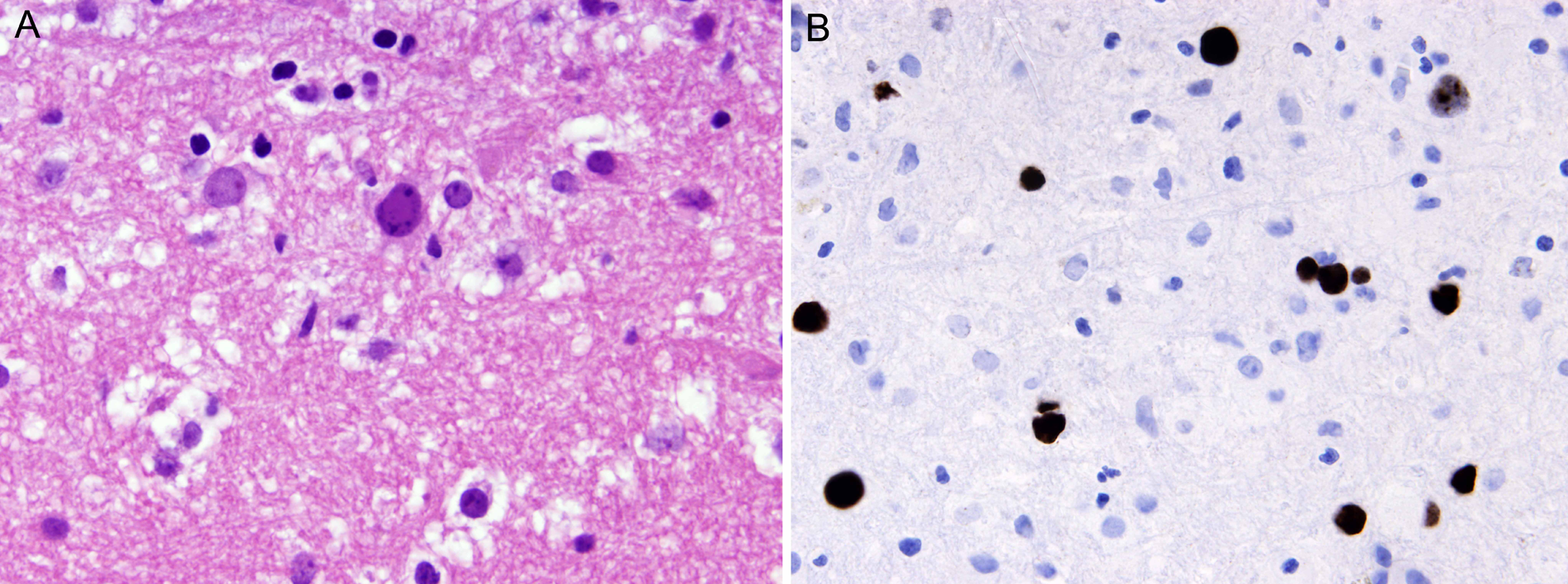
Progressive multifocal leukoencephalopathy: A. The brain biopsy reveals rare cells with round nuclei and smudged chromatin, suggesting the presence of viral inclusion. B. Immunostaining with SV40 (simian virus 40) antibody reveals considerable numbers of positive cells, supporting a diagnosis of JC virus infection (progressive multifocal leukoencephalopathy).
Anaplastic Lymphoma Kinase (ALK; New-Generation Antibodies)
Nature of Antigen and Immunoreactivity in Normal Cells
Antibodies against ALK have long been used to support diagnoses of ALK+ anaplastic large-cell lymphoma, ALK+ large-B-cell lymphoma, and ALK+ inflammatory myofibroblastic tumor. However, the standard ALK antibodies (such as ALK1 clone) are not sensitive enough to consistently demonstrate ALK expression in pulmonary adenocarcinoma with ALK gene translocation because of the low level of ALK chimeric protein expression. This problem can be solved by the new-generation ALK antibodies, such as 5A4 (mouse monoclonal antibody), D3F3 (rabbit monoclonal antibody), and D9E4 (rabbit monoclonal antibody), which are much more sensitive.79-82 Like standard ALK antibodies, the new-generation ALK antibodies do not stain normal cells, with the exception of rare neural cells.
Immunoreactivity in Tumors and Practical Applications
The new-generation ALK antibodies label various ALK-translocated tumors much more intensely than the standard ALK antibodies. Staining of ALK-translocated pulmonary adenocarcinomas is moderate to strong, and there is excellent correlation between immunohistochemical and fluorescence in situ hybridization (FISH) results (Figure 15).80,83-85 In a recently published guideline on ALK testing in lung cancer, immunohistochemistry is recommended as the screening tool, with molecular study (FISH) being reserved as a confirmatory test for cases showing any degree of immunostaining. 79
Pulmonary adenocarcinoma with ALK (anaplastic lymphoma kinase) gene translocation: A. The tumor shows a cribriform growth pattern, one of the characteristic (but not pathognomonic) growth patterns of this tumor type. B. Immunostaining with 5A4 antibody against ALK shows extensive strong staining.
Succinate Dehydrogenase B (SDHB)
Nature of Antigen and Immunoreactivity in Normal Cells
SDHB is a subunit of succinate dehydrogenase (SDH), which is located in the inner membranes of mitochondria. Because all normal cells contain mitochondria, all are immunoreactive for SDHB, with a granular cytoplasmic staining pattern.
Loss of SDHB Immunoreactivity in Hereditary Paragangliomas
A proportion of patients with paraganglioma or pheochromocytoma have an inherited syndrome (paraganglioma-pheochromocytoma syndrome or hereditary paragangliomatosis), and the underlying genetic defect is germline mutation in one of the SDH genes: SDHA, SDHB, SHDC, or SDHD.86-88 There may or may not be a known family history.
The various subunits of SDH are assembled in the mitochondria to form the mitochondrial complex 2, a key respiratory enzyme that links the Krebs cycle and the electron transport chain. 88 Abnormality in any subunit caused by double-hit inactivating mutations will lead to degradation of the complex. Therefore, analysis of 1 SDH subunit (such as SDHB) is sufficient to screen for the presence of mutations in the various SDH genes. 88 As expected, hereditary paragangliomas/pheochromocytomas lack immunoreactivity for SDHB, whereas nonhereditary (sporadic) paragangliomas/pheochromocytomas usually show positive staining (Figure 16). The interpretation must be made in areas where appropriate internal positive controls are present, such as endothelial cells and lymphoid cells. According to the study of van Nederveen et al, 89 the sensitivity and specificity of SDHB immunohistochemistry for the detection of the presence of germline mutations in an SDH gene are 100% and 84%, respectively. Thus, SDHB immunohistochemistry can be utilized as a screening tool for all paragangliomas and pheochromocytomas, with cases showing loss of SDHB staining to be triaged for molecular analysis of a SDH germline mutation.88,90
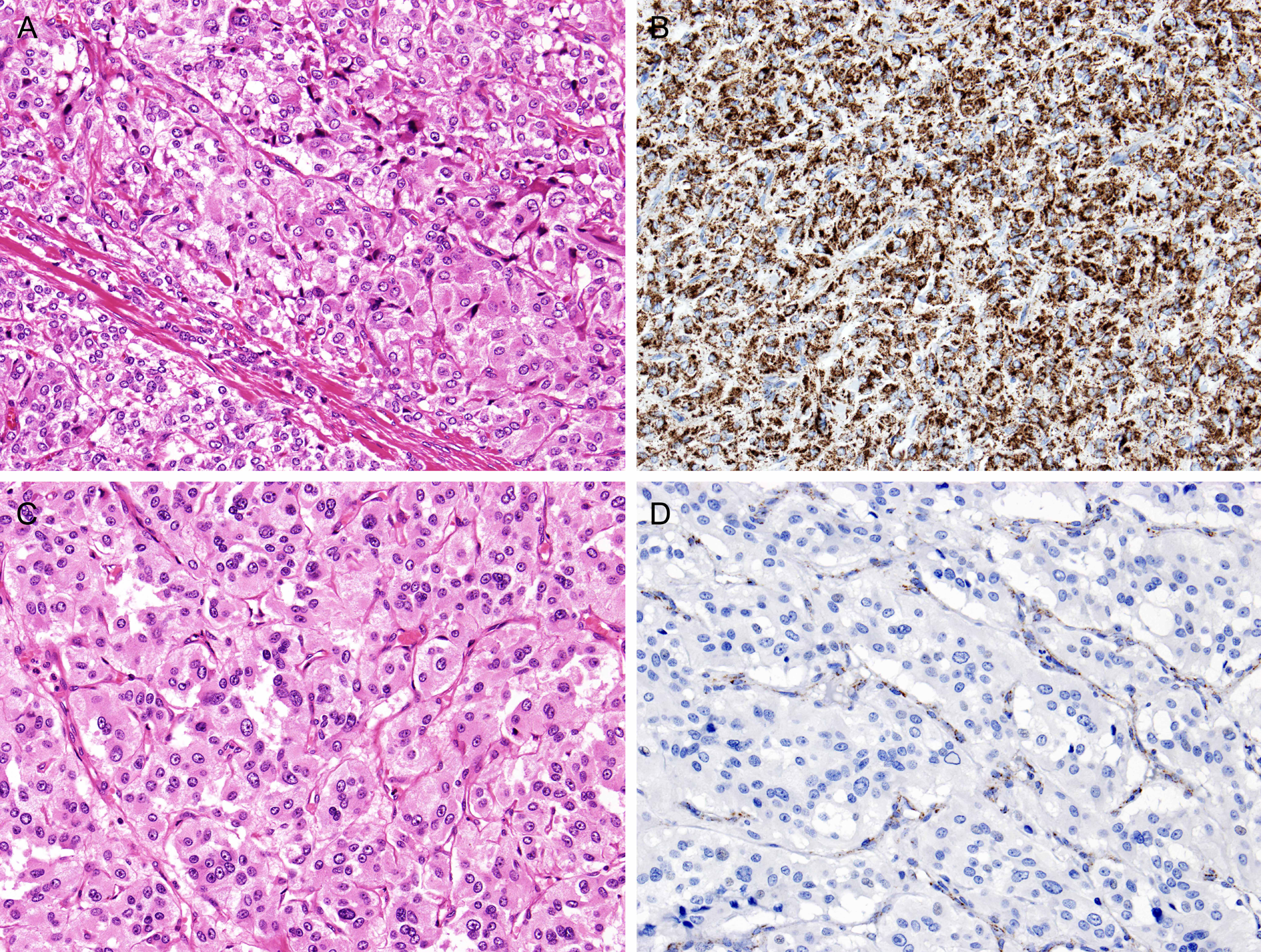
Succinate dehydrogenase B (SDHB) immunohistochemistry in paragangliomas. (A, B) Sporadic paraganglioma. A. Typical paraganglioma with packeting pattern and prominent vasculature. B. The tumor cells show granular staining for SDHB, supporting the sporadic nature of the tumor. (C, D) Hereditary paragangliomas. C. Typical paraganglioma morphology. D. The tumor cells are negative for SDHB, whereas the endothelial cells are positive (supporting validity of the immunostain). This pattern of staining is suggestive of the hereditary form of paraganglioma and would mandate investigation for germline mutations in the SDH gene.
Loss of SDHB Immunoreactivity in a Distinct Subtype of GIST
In recent years, a distinct subtype of GIST, the pediatric type (type II; SDH-deficient type), has been recognized (Figure 17).91-93 It is characterized by the following features:
Occurrence predominantly in children and young adults 94
Female predominance
Gastric localization, often with multinodular or plexiform growth pattern
Multiple tumors
Often epithelioid morphology and malignant histological features
High frequency of metastasis, especially to lymph nodes
Good prognosis despite presence of metastases
Absence of KIT and PDGFR mutations
Pediatric-type gastrointestinal stromal tumor: A. This gastric tumor occurring in an adolescent girl shows an epithelioid morphology. Both KIT and DOG1 are positive (results not shown). B. Immunostaining for succinate dehydrogenase B (SDHB) shows negative staining in the tumor cells, whereas the endothelial cells of the interspersed blood vessels are positive. This feature indicates the pediatric type (type 2 or SDH-deficient type) of gastrointestinal stromal tumor.
GISTs of the Carney triad (occurrence of 3 tumor types: GIST, extra-adrenal paraganglioma, and pulmonary chondroma but with no known familial basis) and Carney-Stratakis syndrome (familial paraganglioma and GIST caused by germline mutation in either SDHB, SDHC, or SDHD) also fall into this group but not those of neurofibromatosis. 95 Pediatric-type GISTs consistently lack immunoreactivity for SDHB, whereas usual GISTs (adult-type or type I) are strongly positive. 91 It is important to recognize the pediatric (SHD-deficient) type because of the good prognosis even in the presence of metastases. When a GIST is found to be SHD deficient, molecular analysis for germline mutations in SDH genes may be warranted if there are relevant clinical features.
Two recent studies report very interesting findings on SDHA mutation. Using an antibody against SDHA, 28% of SDHB-deficient GISTs are found to lack immunoreactivity. All these cases are found to exhibit germline mutation in the SDHA gene.96,97 Thus, it is suggested that immunostaining for SDHA can be used to select patients for genetic testing for germline mutations in the SDHA gene. 97
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.