
Abstract
Intra-abdominal cysts have a variety of origins, of which lymphatic and mesothelial types are the most commonly encountered. Here we describe a combined mesothelial cyst and lymphangioma arising within the small bowel subserosa of an 80-year-old woman. This was found incidentally at laparotomy performed for an unrelated condition. To date, such a hybrid lesion has not been previously reported. The ways by which this lesion might have arisen are discussed.
Introduction
Cystic lesions in the abdominal cavity can occur in the retroperitoneum, mesenteries, bowel subserosa, or on or within visceral organs such as the spleen. They are often found incidentally, although can grow to large sizes and give rise to symptoms of abdominal distension and pain.1,2 Pathologically, abdominal cysts can be classified into (a) cysts of lymphatic origin, (b) cysts of mesothelial origin, (c) cysts of enteric origin, (d) cysts of urogenital origin, (e) mature cystic teratomas, or (f) pseudocysts. 3 We report a case of a woman with recurrent endometrial sarcoma, who was found incidentally at laparotomy to have a nodule within the small bowel subserosa, and which was histologically a combined mesothelial cyst and lymphangioma. To our knowledge, this is the first such case described.
Case Report
An 80-year-old woman had a history of endometrial stromal sarcoma resected 19 years previously with total hysterectomy, bilateral salpingoophorectomy, and left nephrectomy. She had remained well until she presented with heavy sweats and shivering at night without fever. Magnetic resonance imaging scan showed a large 12 × 9.9 cm left-sided hemipelvic mass with focal calcification and central necrosis, at the site of previous disease. There was no intestinal obstruction or vessel encasement, and all viscera, including the single right kidney, were unremarkable. Core biopsy of the mass showed high-grade endometrial sarcoma, consistent with recurrence of the previous neoplasm. The patient proceeded to laparotomy and resection of the pelvic tumor, during which a small nodule was noted on a segment of small bowel wall. This was thought clinically to represent a separate focus of transperitoneally disseminated sarcoma and was also excised.
Materials and Methods
Immunohistochemical staining (streptavidin-biotin peroxidase complex method, with diaminobenzidine as the chromogen) was performed on formalin-fixed, paraffin-embedded tissue using a panel of commercial antibodies (Table 1).
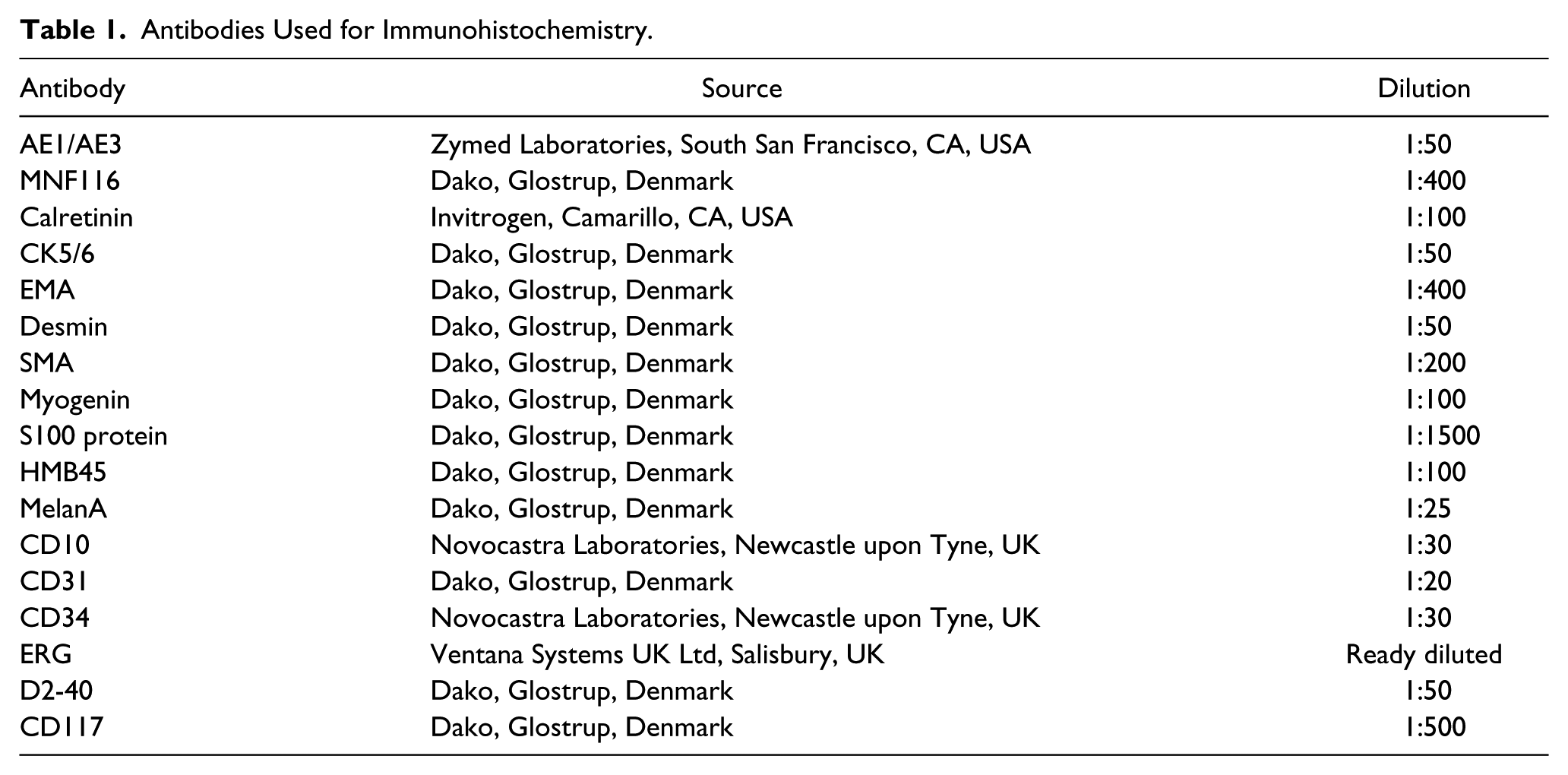
Antibodies Used for Immunohistochemistry.
Results
Gross examination of the main specimen showed a large 17 × 13 × 12 cm lobulated tumor adherent to segments of both small and large bowel, and with variegated cut surface with firm pale cream tissue, extensive necrosis, and hemorrhage. The separate smaller lesion comprised a 2 × 1.5 × 1 cm nodular piece of soft gelatinous tissue with unremarkable small bowel mucosa at one end. Bisecting the lesion showed that it was composed of multiple small cysts containing thick yellowish fluid. No hard areas, necrosis, or papillary excrescences were present.
Histologically, the main tumor was an infiltrative, focally necrotic and highly mitotic cellular neoplasm comprising sheets of highly pleomorphic spindle and epithelioid cells with ovoid nuclei and eosinophilic cytoplasm, diffusely positive for CD10, ER, and PgR, focally positive for h-caldesmon and negative for AE1/AE3, MNF116, epithelial membrane antigen (EMA), S100 protein, desmin, myogenin, CD34, CD117, MelanA, and HMB45, and similar to the previous biopsy. JAZF1-SUZ12 fusion transcript was present with quantitative real-time reverse transcription polymerase chain reaction, and the features were of high-grade endometrial sarcoma.
Sections of the small bowel lesion showed expanded subserosa containing a haphazard pattern of multiple cystic structures (Figure 1A) ranging from 0.5 to 6 mm in diameter. The cysts were well formed and dilated, and were either largely empty, sometimes with fibrinoid material or with acellular fluid consistent with lymph (Figure 1B). At higher power, it was apparent that there were different types of cyst, present in roughly equal proportions and closely but randomly intermingled. All cysts were lined by single layers of cells. Some were lined by small cuboidal cells with ovoid vesicular nuclei, often small pinpoint nuclei, and moderate amounts of amphophilic cytoplasm (Figure 1C), which while in areas were plump showed no cellular atypia or pleomorphism. Other cysts were lined by flattened simple, often almost indiscernible cells with small, hyperchromatic ovoid nuclei and scanty cytoplasm (Figure 1D), again lacking any cellular atypia. No infiltrating pattern, solid cellular areas, mitotic figures or necrosis were present. The cuboidal cells were diffusely positive for AE1/AE3 (Figure 2A), calretinin, and D2-40, and negative for CK5/6, CD31, CD34, and ERG. The flattened cells were diffusely positive for CD31 (Figure 2B) and ERG (Figure 2C) and focally for D2-40, but negative for CD34, AE1/AE3, CK5/6, and calretinin. SMA and desmin highlighted thin bundles of smooth muscle surrounding their walls (Figure 2D), which were often difficult to discern morphologically. There was no immunoreactivity for S100 protein, HMB45, or MelanA.
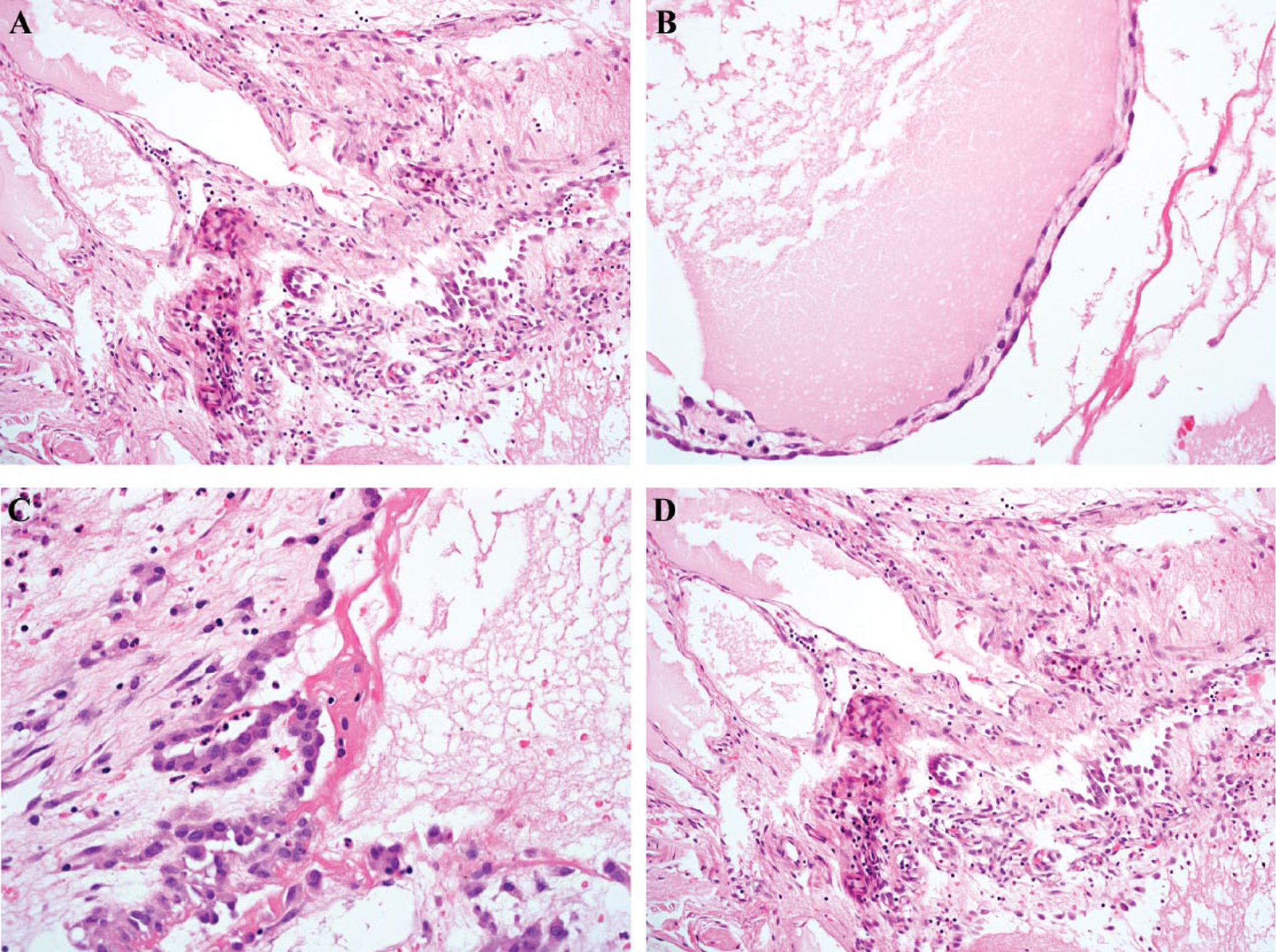
(A) Histologically, the small bowel subserosa shows expansion by multiple, dilated cystic structures, present in a haphazard pattern. (B) The cysts are well formed and are either largely empty with small amounts of fibrinoid material or, as illustrated here, contain acellular fluid consistent with lymph. (C) There are 2 types of cysts, which are extensively intermingled. The first type is lined by small cuboidal cells with ovoid vesicular nuclei and often small pinpoint nuclei, which are plump but show no cellular atypia or pleomorphism. (D) The second type of cyst is lined by bland flattened cells which are often difficult to discern (left of field). The mesothelial cystic component is present on the right.
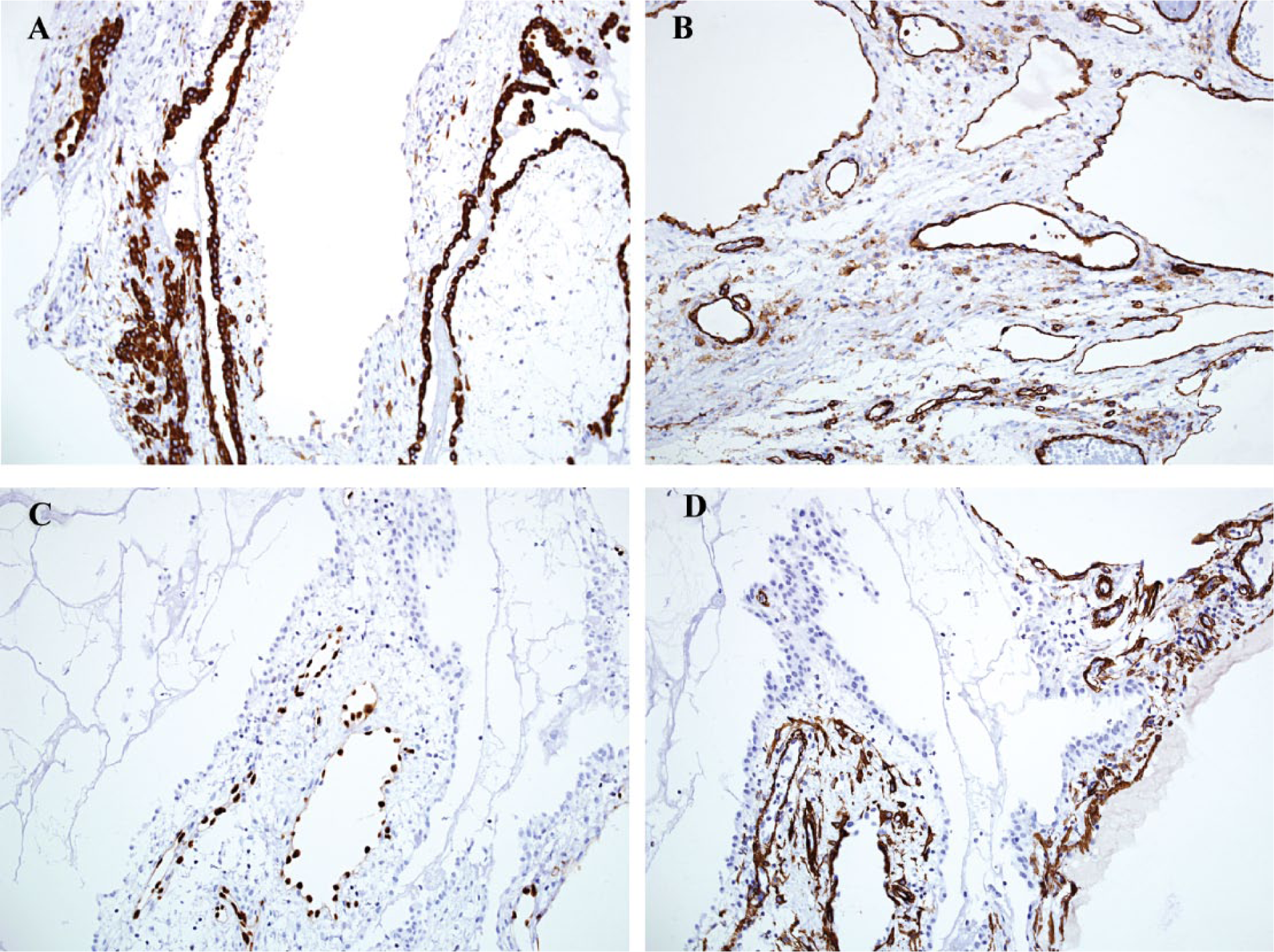
(A) The cuboidal cells are diffusely positive for AE1/AE3 (shown here), as well as calretinin and D2-40, consistent with mesothelial differentiation. Note the intermingled second cystic component lined by flattened cells (center), which are negative for AE1/AE3. (B, C). The flattened cells are strongly positive for CD31 (B) and ERG (C), consistent with lymphatic/vascular endothelium. Above and to the right of the cysts lined by ERG-positive cells are mesothelial cysts, in which the hyperplastic mesothelium is nonimmunoreactive for ERG. (D) SMA highlights the smooth muscle surrounding the lymphatic cysts. This is noticeably absent in the adjacent mesothelial cysts.
The findings were of a benign multicystic lesion with features of combined lymphangioma and mesothelial cyst. The patient was discharged uneventfully.
Discussion
Intra-abdominal cystic lesions can be classified into 6 groups: (a) cysts of lymphatic origin, (b) cysts of mesothelial origin, (c) cysts of enteric origin, (d) cysts of urogenital origin, (e) mature cystic teratomas, or (f) pseudocysts. Of these, cysts of lymphatic and mesothelial origin are the most commonly encountered. 3
Cysts of lymphatic origin can be subdivided into cystic lymphangioma or benign lymphatic cysts. 4 While it was previously thought that cystic lymphangiomas (hygromas) usually occur in childhood with a female predominance, a much wider range of ages (23-75 years) has now been shown. 1 It is thought that lymphangiomas might represent malformations, caused by proliferating ectopic lymphatics or the failure of lymphatic vessels to communicate with the venous system. Lymphatic cysts predominantly occur in adulthood, with a female preponderance. Although these lesions are usually asymptomatic, they may cause abdominal discomfort or distension.
Histologically, both cystic lymphangiomas and benign lymphatic cysts appear similar, and comprise large lymphatic channels dispersed within loose connective tissue, although lymphangiomas have a disorganized smooth muscle layer surrounding the vessels. Despite the similarities, correct diagnosis is important as lymphangiomas can be locally infiltrative and carry a risk of local recurrence, 1 whereas lymphatic cysts tend to be localized lesions.
Mesothelial cysts, which are also known as peritoneal inclusion cysts, or sometimes, confusingly, benign cystic mesotheliomas, are thin-walled cysts lined by mesothelial cells, most often found within the mesenteries or omentum. More rarely, they are found on the surfaces or parenchyma of organs such as the spleen. 5 Although the majority behave indolently, malignant transformation can occur more rarely. 6 Clinically, radiologically, and histologically, they can be confused with cysts of lymphatic origin: Both have a wide presenting age range (10-61 years), similar presenting symptoms, and range from 3 to 20 cm in size.1,2 In fact, some intra-abdominal cysts that were previously thought to be lymphangiomas were on further investigation found to be mesothelial cysts.7,8 Early reports used ultrastructural differences to distinguish between mesothelial or endothelial cells lining the cysts 7 but now immunohistochemistry is used to differentiate between the two.5,9 Lymphatic endothelial cells are positive for CD31, D2-40, and ERG, while mesothelial cells are variably positive for cytokeratins, WT1, CK5/6, calretinin, and also D2-40.
This case clearly showed 2 intermingled but different types of cyst lined by separate populations of cells. This was suspected morphologically, with some cysts having a cuboidal cell lining while others were lined by flattened, often barely perceptible cells, with the 2 different cellular origins confirmed immunohistochemically. In addition, many of the cysts lined by lymphatic endothelial cells had surrounding thin layers of smooth muscle, favoring lymphangioma. The overall diagnosis was therefore of a combined or composite lymphangioma and mesothelial cyst.
The etiology of this hybrid lesion is unclear. Mesothelial cysts are frequently idiopathic, although can develop secondary to causes of peritoneal irritation such as intra-abdominal malignancy, surgery, or ascites, which result in the invagination of the serosal lining. 2 Two of these precipitating factors were notable in this patient’s previous history. While childhood lymphangiomas can be developmental malformations or hamartomas as discussed earlier, some of these might be reactive to inflammation, trauma, or surgery, 10 which result in obstruction of lymphatic drainage with secondary dilation and cyst formation of the lymph channels. Again, these precipitating features were present in this patient. One possibility for the development of this hybrid lesion is of the patient having a longstanding nonsymptomatic lymphangioma, in which the mesothelial cystic lesion developed secondary to her previous treatment. These components then slowly intermingled over the course of the nearly 2 decades between her treatment and this new presentation. Finally, and least likely, is the redifferentiation or metaplasia of one cell type to the other. In summary, this is the first reported case of a combined lymphangioma and mesothelial cyst, showing an unusual complex intermingling of these 2 components.
Footnotes
Acknowledgements
We acknowledge support from the NIHR RM/ICR Biomedical Research Centre.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.