
Abstract
Schwannoma is a benign peripheral nerve sheath neoplasm of soft tissue that consistently demonstrates immunohistochemical staining for S100 protein. Intraosseous location of schwannoma is very uncommon. We report the first case of an intraosseous schwannoma located in the epiphysis of tibia in an adult patient. Radiologically, it mimicked a primary bone tumor and despite benign histological appearance, the tumor eroded cortical bone. Morphologically on routine stains and electron microscopy it has features of a schwannoma. But by immunohistochemistry, the tumor was positive for both desmin and S100 protein in the same region.
Introduction
Schwannoma is a benign peripheral nerve sheath neoplasm arising from Schwann cells of nerve, typically sensory nerve roots. It usually presents as a slowly growing mass with nonspecific neurological symptoms. They can occur at any age, most commonly in the 30s and 40s, with no sex predilection. Schwannoma is a common peripheral nerve sheath tumor accounting for 8% of intracranial and 28% of primary spinal tumors. The estimated incidence is approximately 1 in 40 000. Bilateral vestibular schwannomas are characteristic of NF2. Sensory nerves are preferentially affected because of high Schwann cell to axon ratio (1:1). 1 Minor sensory loss can occur but motor changes are uncommon. Clinically and radiologically, schwannoma usually is eccentrically located in relation to the nerve in contrast to the centrally located neurofibroma. 2 This feature allows surgical resection without sacrificing a major nerve.
Although the most common location is soft tissue of head and neck, schwannoma can rarely occur within bone. The incidence of intraosseous schwannoma is the highest in the mandible along the long intraosseous course of the inferior alveolar nerve, but documented reports also exist of schwannomas arising within the maxilla, sacrum, vertebral bodies, radius, ulna, sternum, ribs, humerus, metacarpals, femur, and fibula. 1 Clinically, intraosseous schwannoma usually presents as a slowly growing bone lesion with local pain and swelling.
We report the first case of an intraosseous schwannoma located in the epiphysis and metaphysis of the tibia in an adult patient. It mimicked a primary bone tumor radiologically, and was found to have unique pathologic features.
Case Presentation
Clinical History
This 75-year-old woman was admitted to the University of Pittsburgh Medical Center for left distal leg pain that had persisted for over a year associated with a small lump. There was no history of trauma or infection. Her past medical history was significant for diabetes mellitus type 2, hypertension, coronary artery disease, deep vein thrombosis, and pulmonary embolism. On physical examination, the patient had a visible nontender mass over the anterolateral aspect of her left ankle proximal to the tibiotalar joint line. The left lower extremity was neurologically intact with normal range of motion of the ankle. The patient’s blood counts and basic metabolic panel were within normal limits.
Radiographic views of the left ankle demonstrated a multilobulated lucent lesion measuring 4.8 × 4.2 × 3.5 cm in the distal tibial epiphysis and metaphysis, sparing the tibiotalar joint. It was well defined with a thin sclerotic rim and narrow zone of transition without any intralesional calcification. There was no significant periosteal reaction. Computed tomographic scan showed a lobulated intraosseous lesion involving the epiphysis and metaphysis of the tibia. There was associated bone remodeling of the adjacent bone. A small area of cortical breakthrough along the lateral tibial cortex approaching the distal tibiofibular joint was noted, resulting in slight bone remodeling along the medial aspect of the distal fibula (Figure 1). Differential diagnosis based on radiographic findings included giant cell tumor, unicameral bone cyst, aneurysmal bone cyst, and chondrosarcoma. Schwannoma was not considered.

Radiologic findings. (A) Plain radiograph and (B) computed tomographic scan of left tibia demonstrated multilobulated lucent lesion of distal tibial epiphysis and metaphysis, sparing the tibiotalar joint. The lesion was well-defined with a thin sclerotic rim and narrow zone of transition. A small area of cortical breakthrough along the lateral tibial cortex approaching the distal tibiofibular joint was noted. No significant periosteal reaction was seen.
The patient underwent biopsy, curettage, and cementation because of impending fracture. During surgery, an incision was made directly over the soft tissue mass anteriorly. The lesion was found to have a prominent fibromyxoid consistency with 95% of the lesion occupying the tibial epiphysis and the remainder extending into the adjacent metaphysis. A focus of soft tissue extension was found, with no joint invasion. The lesion was removed with meticulous curettage and the bone defect was filled with polymethylmethacrylate cement. The patient tolerated the procedure well without complications.
Gross Features
Gross pathological examination of excised specimen showed an aggregate of tan-white irregular soft tissue admixed with hemorrhagic, gelatinous material, tan-white firm bone fragments, and focal cystic areas.
Microscopic Features
Microscopic examination on routine hematoxylin and eosin–stained sections revealed foci of viable medullary and cortical bone with no periosteal new bone formation. The tumor was moderately cellular and consisted of sheets of monomorphic, plump spindle cells with bland nuclei, well-defined cytoplasmic borders, and some cytoplasmic vacuoles. Tumor cells were haphazardly arranged. A rare focus of nuclear palisading, resulting in vague Verocay bodies, was noted (Figure 2). Ectatic and hyalinized blood vessels were readily identified. Some hyalinized areas resembled senescent schwannoma. Compact and myxoid areas were also identified. Neither mitotic activity nor necrosis was seen.
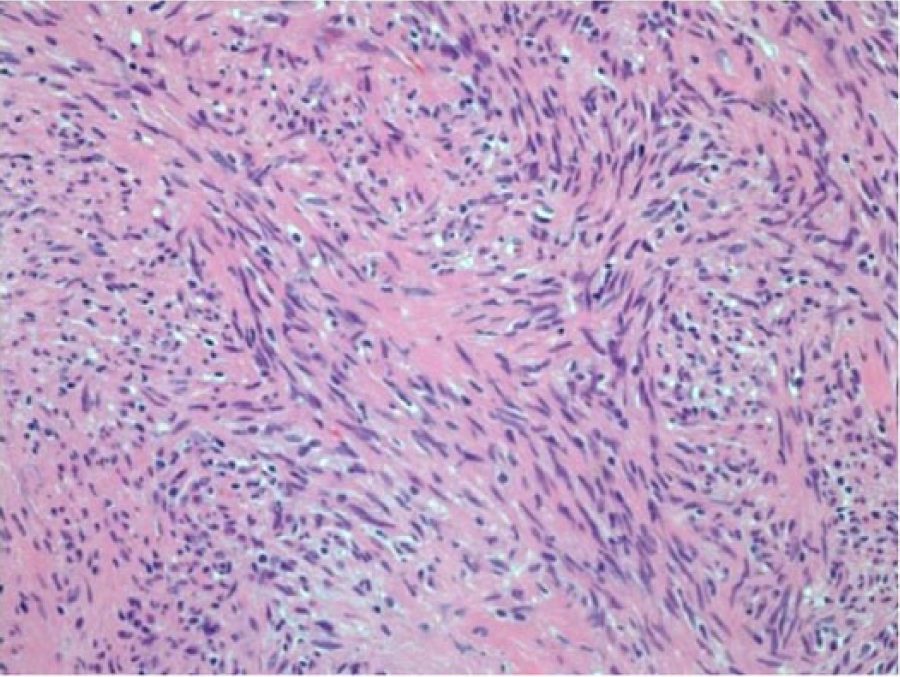
Histological features. The lesion was located mainly in medullary cavity of bone with focal cortical bone breakthrough and composed of monomorphic spindle cells with haphazard arrangement, some areas with nuclear palisading and vague Verocay bodies. The spindle cells were plump with bland nuclei and well-defined cell borders; some had cytoplasmic vacuoles; magnification 100×.
Immunohistochemical stains were performed to further characterize the tumor. The tumor cells strongly and diffusely expressed S100 (polyclonal rabbit, 1:500, Dako, Glostrup, Denmark) with both nuclear and cytoplasmic immunoreactivity (performed on 2 sections). CD56 (monoclonal mouse, prediluted, Cell Marque, Rocklin, CA) and glial fibrillary acidic protein (GFAP; monoclonal mouse, 1:25, Ventana, Tucson, AZ) also were strongly positive. Tumor cells were focally reactive for desmin (monoclonal mouse, prediluted, Ventana) and actin (all muscle, clone HHF-35, monoclonal mouse, 1:100, Dako) in the same regions that were positive for S100. Interestingly, 2 to 3 clusters of cells of uncertain lineage expressed pancytokeratin (polyclonal rabbit cocktail, Abcam, Cambridge, MA) in the areas negative for S100. Tumor cells were negative for myogenin (monoclonal mouse, prediluted, Cell Marque), Melan A (monoclonal mouse, 1:100, Dako), P63 (monoclonal mouse, 1:200, Thermo Scientific, Waltham, MA), and estrogen receptor (rabbit monoclonal, prediluted, Ventana). Ki-67 (monoclonal mouse, 1:100, Dako) was performed on 2 separate paraffin blocks and revealed 2% to 5% positivity (Figure 3). The final diagnosis was intraosseous schwannoma with aberrant positivity for muscle markers.
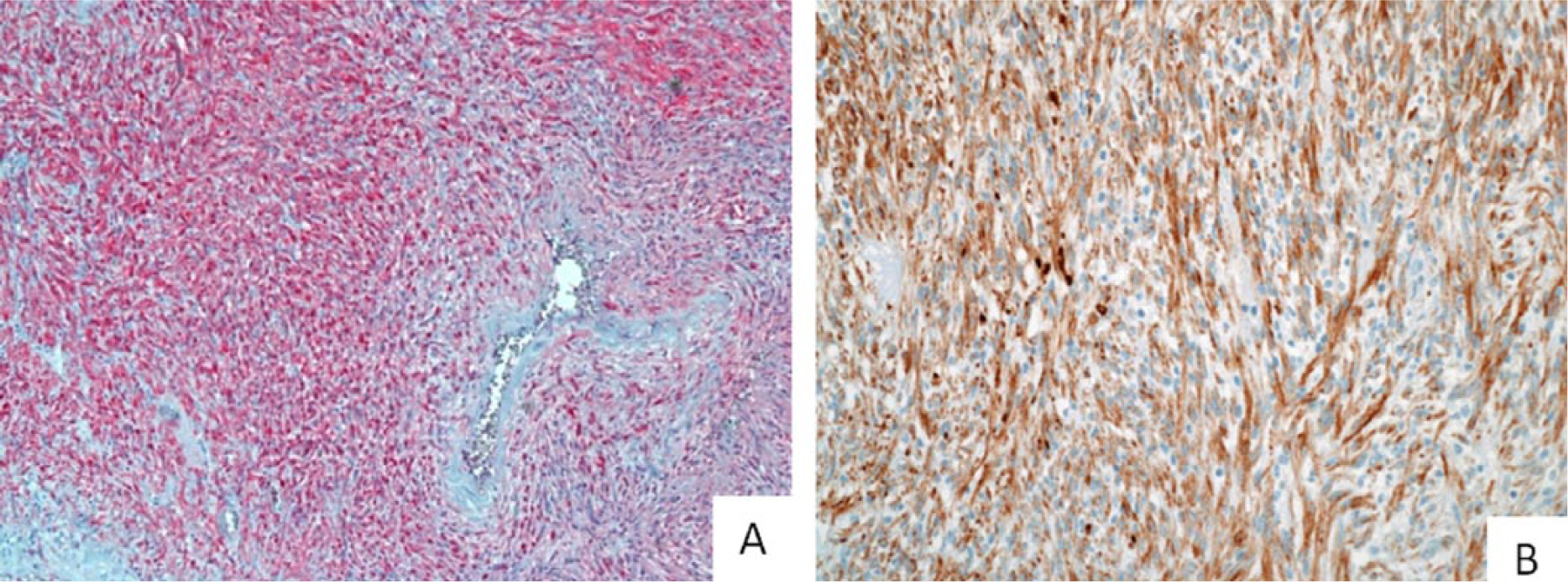
Immunohistochemical stains. The tumor cells are strongly and diffusely positive for (A) S100 (magnification, 40×) and focally positive for (B) desmin (magnification, 100×) in the same area.
Electron Microscopic Features
Ultrastructural examinantion of the formalin-fixed tissue of the region displaying desmin and S100 immunopositivity revealed spindle cells with slender, rarely interdigitaing, cytoplasmic processes, and oval nuclei. There were few primitive intercellular cell junctions and some cells had discontinuous basal lamina. There were abundant microfilaments in the cytoplasm that did not demonstrate typical Z bands. Luse bodies with parallel long-spaced collagen fibers, microfilaments, and partial basal lamina present were present (Figure 4). The cellular detail was poor because of formalin fixation, but findings were consistent with those described in schwannoma. The presence of abundant cytoplasmic microfilaments was considered unusual.
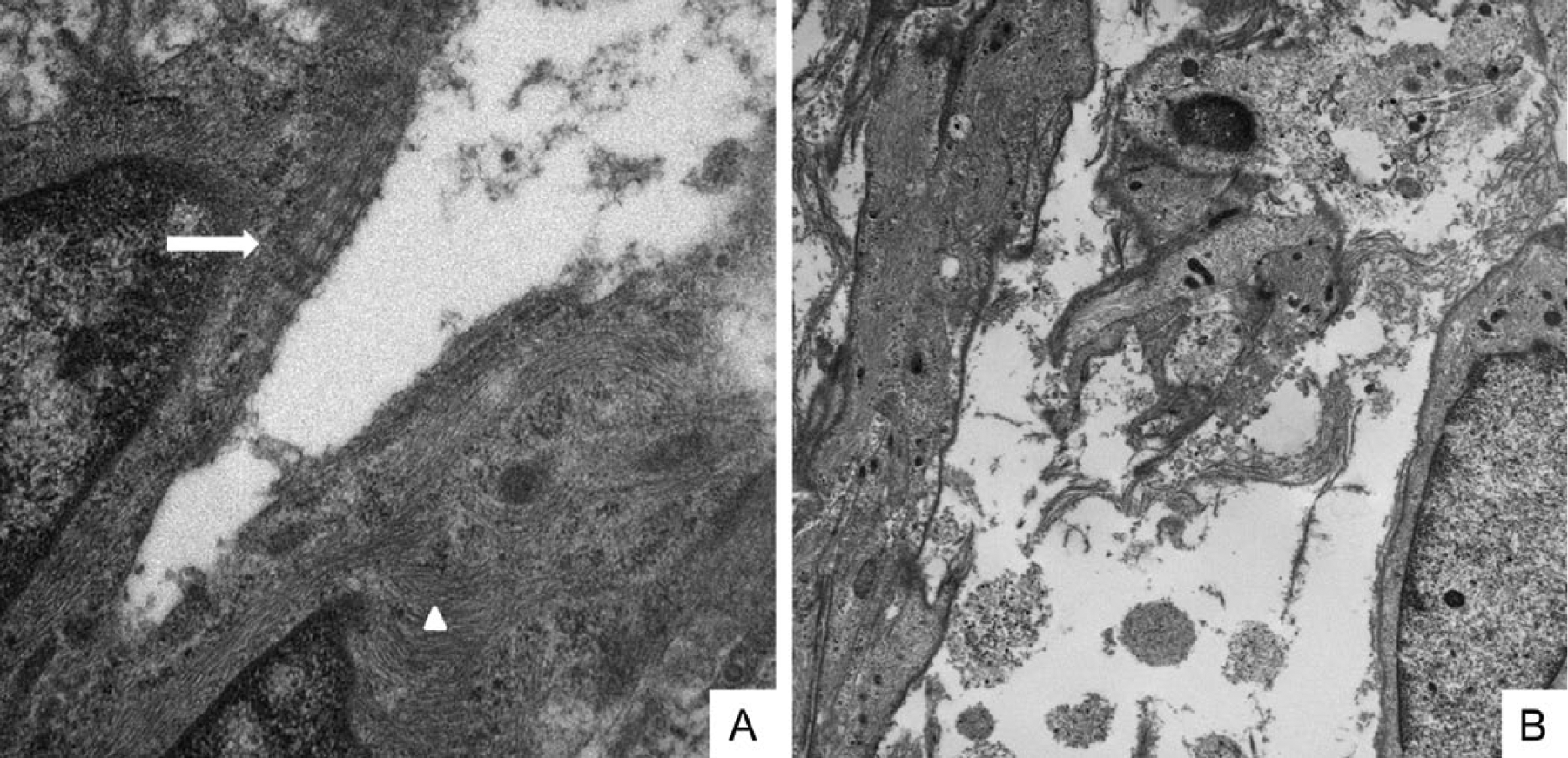
Electronic microscopy of tumor cell. (A) Luse bodies formed from parallel troopcollagen fibers (arrow) and collections of collagen fibers in cytoplasm (arrowhead) (magnification, 22 000×). (B) Microfilaments and partial basal lamina (magnification 11 000×).
Discussion
Intraosseous schwannoma is a very rare entity and accounts for less than 2% of benign bone tumors. Mandible, maxilla, and sacrum are the most common sites, although theoretically any bone can be involved.3-5 However, schwannomas in these cases are arising from nerves that do not innervate the bone but rather pass through these bones. Primary schwannoma of bone is defined as schwannoma limited to the substance of bone and centered in the medullary cavity. They are mostly metaphyseal lesions; only one intraosseous schwannoma has been described in the epiphysis of the bone in a pediatric case. 6 They probably arise from vasomotor nerves that accompany blood vessels to the bone marrow. They are slow growing tumors and the most common clinical presentation is pain. Radiologically, intraosseous schwannoma presents as a benign cyst-like bone lesion centrally located within a long bone and has a thin sclerotic rim, often mimics other primary bone tumors. Extraosseous extension has been reported in intraosseous schwannoma. 7 Histologically, the tumor has all the features of conventional schwannoma with alternating cellular Antoni A and hypocellular Antoni B areas. Characteristic nuclear palisading referred to as Verocay bodies may be seen in Antoni A areas. Cellular schwannoma only contains Antoni A areas and tends to have a more fascicular arrangement of tumor cells. The immunohistochemical features include diffuse, strong S100 expression (both nuclear and cytoplasmic) with rare focal cytokeratin positivity. 2 Primary intraosseous schwannoma can be treated with either curettage or en bloc excision; bone grafting is usually needed. 8 Tumor may recur locally if incompletely resected, but no malignant transformation has been reported.
Radiologically, our case showed a multilobulated lucent lesion of the distal tibial epiphysis with well-defined borders and a thin sclerotic rim, which indicated a nonaggressive behavior. But there was also a small area of cortical breakthrough so aggressive lesion could not be completely ruled out. Histologically, the lesion displayed occasional Verocay bodies and was diffusely positive for S100 protein, some regions were strong positive for desmin in serial sections of the same block. A couple of small foci of cytokeratin positive cells was also found although not in the spindle S100 positive cells. Several differential diagnoses were considered. Malignant peripheral nerve sheath tumors (MPNSTs) have been described with rhabdoid differentiation and desmin and actin positivity (triton tumor), but only less than a third of MPNST cells show focal S100 staining compared with the strong diffuse S100 immunopositivity found in schwannoma. 9 The strong GFAP and CD56 positivity and low Ki-67 (ranging 2% to 5%) proliferative activity noted in our case also made MPNST unlikely. It is also unlikely to represent malignant melanoma given this morphology and lack of immunohistochemical reactivity for other melanoma markers. Ultrastructually, no premelanosomes were found either. Benign triton tumor, also known as neuromuscular hamartoma, was also considered. It is an exceedingly rare entity that occurs in a very young population and exhibits characteristic fascicles of striated muscle of varying size mixed with nerve fibers within the same perimysial fibrous sheath. 10 These features were absent in our case. Myoepithelioma have been shown to demonstrate S100 and desmin positivity. 11 But the diffused positivity for CD56 and GFAP, together with rare staining for cytokeratin, made it unlikely to be myoepithelioma. Ultrastuctural features also supported the diagnosis of schwannoma in our case. 12
The unique features in our case include aberrant desmin positivity expressed in the same region, if not the same Schwann cells. The presence of focal desmin positivity is very unusual for schwannoma; only one desmin-positive schwannoma has been reported, recurrent in the retroperitoneum. 13 Myofibroblastic phenotype of Schwann cells has been noted in in vitro experiments of other species. During vertebrate embryogenesis, the migrating cervical and cephalic neural crest cells, including pleuripotent and oligopotent cells, can undergo a phenotype switch induced by the environment and growth factors, such as transforming growth factor-β. 14 Therefore, benign Schwann cell neoplasms may have the same capability to switch and express a muscle phenotype, albeit rarely. Interestingly, lipomatous changes have also been noted in schwannomas, suggesting that Schwann cells are capable of differentiating along different mesenchymal lines. 15 Another unusual feature of our case is the epiphyseal location that simulated a giant cell tumor radiologically. There has been only one report of epiphyseal intraosseous schwannoma in a pediatric patient. 6 Because of the cortical thinning, further clinical follow-up of the patient was considered to be judicious, even though there was no significant cytological atypia
In summary, we report most likely the first intraosseous epiphyseal schwannoma of the tibia in an adult. It presented classic histological features of schwannoma. The presence of microfilaments in electronic microscopy suggests that the desmin positivity is likely not aberrant.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.