
Abstract
Background. Hyalinizing clear cell carcinoma (HCCC) is a rare low-grade malignant tumor affecting the minor salivary glands; nasopharyngeal involvement is uncommon. Methods and Results. A 38-year-old male patient presented with a 3.2 × 4.5 × 4.4 cm expansile mass obliterating the lumen of the nasopharynx and extending into the left nasal cavity. Histopathologically, the tumor was characterized by clear round to polygonal epithelial cells arranged in anastomosing trabeculae and solid nests. The stroma consisted of fibromyxoid connective tissue with areas of intense hyalinization and desmoplasia. Immunohistochemically, strong and diffuse reactivity for AE1/AE3, CK5/6, and p63 was observed. EWSR1 gene rearrangement was confirmed by fluorescence in situ hybridization. The diagnosis of nasopharyngeal HCCC was rendered. Surgical excision was performed along with adjuvant radiotherapy and chemotherapy. Conclusions. HCCC generally demonstrates good prognosis with low metastatic potential. Identification of EWSR1 gene disruption is useful in discerning HCCC from other neoplasms with overlapping microscopic features.
Introduction
Originally described as a distinct entity by Milchgrub et al in 1994, 1 hyalinizing clear cell carcinoma (HCCC) is a rare epithelial malignant neoplasm that predominates in the minor salivary glands of the palate, base of the tongue, and floor of the mouth.2,3 Other less common locations include the parotid and the submandibular glands, the larynx, and, on rare occasions, the orbit and nasopharynx.2,4 Clinically, HCCC manifests usually as an asymptomatic mass. 5 There is slight female predilection, and the majority of patients are in their sixth decade of life.2,3 HCCC is a low-grade malignancy; however, recurrence and nodal metastases have been reported.6,7
Histopathologically, HCCC is characterized by anastomosing cords, nests, and sheets of round or polygonal cells with cytoplasmic clearing and central nuclei; the latter feature mild pleomorphism, inconspicuous nucleoli and low mitotic activity.1-4,8,9 Occasionally, admixed with the clear cells, a subpopulation of smaller, polygonal cells with eosinophilic to amphophilic cytoplasm is noted.2,4,8,9 Characteristically, the stroma of this tumor is hyalinized, but may show myxoid changes.2,3 Perineural and intraneural infiltration occurs in almost 50% of the cases. 9 Foci of squamous and/or ductal differentiation have been observed. 3 Immunohistochemically, HCCC cells demonstrate diffuse and intense positivity for high-molecular-weight keratins (34βE12), CK14, and p63. Focal positivity is noted for epithelial membrane antigen (EMA), CK7, CK19, and CK 8/18 (CAM5.2).3,4,10,11
In 2011, Antonescu et al 9 identified EWSR1 rearrangements in this tumor; these have been subsequently observed in 82% 9 to 92.3% 12 of the cases. This genetic change allows the distinction of HCCC from other salivary gland neoplasms with a clear cell phenotype.
Occurrence of HCCC in the nasopharynx is uncommon, with only 7 cases reported in the English literature. Herein, we report the clinical, histopathologic, and molecular characteristics of a nasopharyngeal HCCC that occurred in a 38-year-old Caucasian male and review pertinent literature.
Case Report
The patient presented with a 5-month history of nasal congestion, nasal voice quality change, and rhinorrhea. Treatment with antibiotics for presumed sinusitis was unsuccessful. Computed tomography (Figure 1) and positron emission tomography revealed a hypermetabolic 3.2 × 4.5 × 4.4 cm lobulated, expansile, nasopharyngeal mass. The tumor obliterated the lumen of the nasopharynx and extended into the left nasal cavity and masticator space. Bilateral involvement of the medial pterygoid lamina and posterior extension into the anterior aspect of the clivus were also noted. Superiorly, the tumor extended into the sphenoid sinus and the left side of the palate approaching the left greater palatine foramen. On the right aspect, the tumor involved the base of the skull and eroded the right foramen ovale. Slightly hypermetabolic lymph nodes were identified at levels IIA and IB on the left and IIA on the right side. There was no evidence of distant metastasis. Incisional biopsy of the tumor was performed.
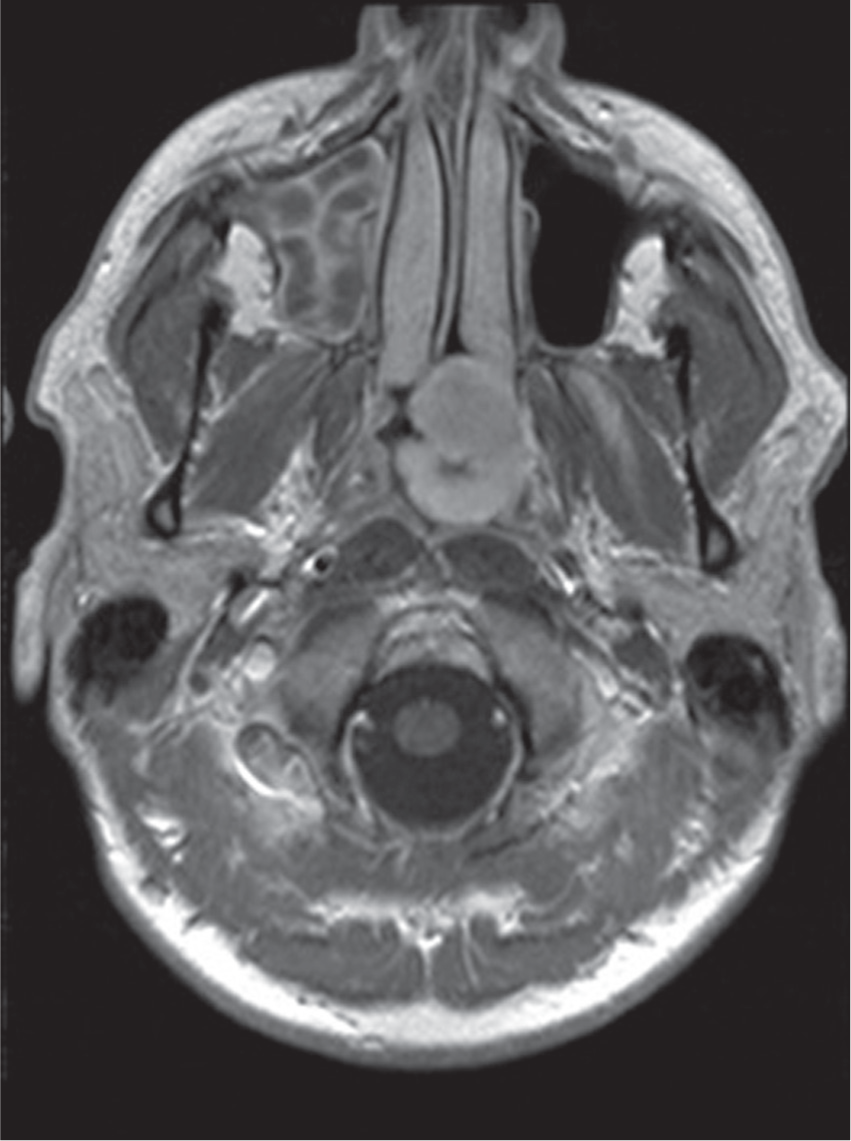
Computed tomography scan reveals a 3.2 × 4.5 × 4.4 cm lobulated, expansile, nasopharyngeal mass that obliterates the nasopharynx and extends into the left nasal cavity and masticator space.
Histopathologically, the tumor was unencapsulated, hemorrhagic (Figure 2A), and characterized by diffuse proliferation of predominantly clear round to polygonal epithelial cells with uniform small, central nuclei (Figure 3A). Rare mitotic figures were identified (Figure 3B). These clear cells were arranged in anastomosing trabeculae, thin interconnecting cords, and solid nests (Figure 2B). Focally, ducts containing amorphous eosinophilic material were noted (Figure 2C). Occasional cytoplasmic eosinophilic droplets (Figure 3D) were identified. A second population admixed with the previous was also noted; it consisted of smaller epithelial cells with eosinophilic cytoplasm and inconspicuous cytoplasmic borders (Figure 3C). The stroma consisted of highly vascularized, variably fibrous, fibromyxoid, and myxoid connective tissue; the latter characteristically exhibited areas of intense hyalinization and desmoplasia (Figure 3A-C). Interestingly, the desmoplastic stroma was predominantly associated with the smaller cells.
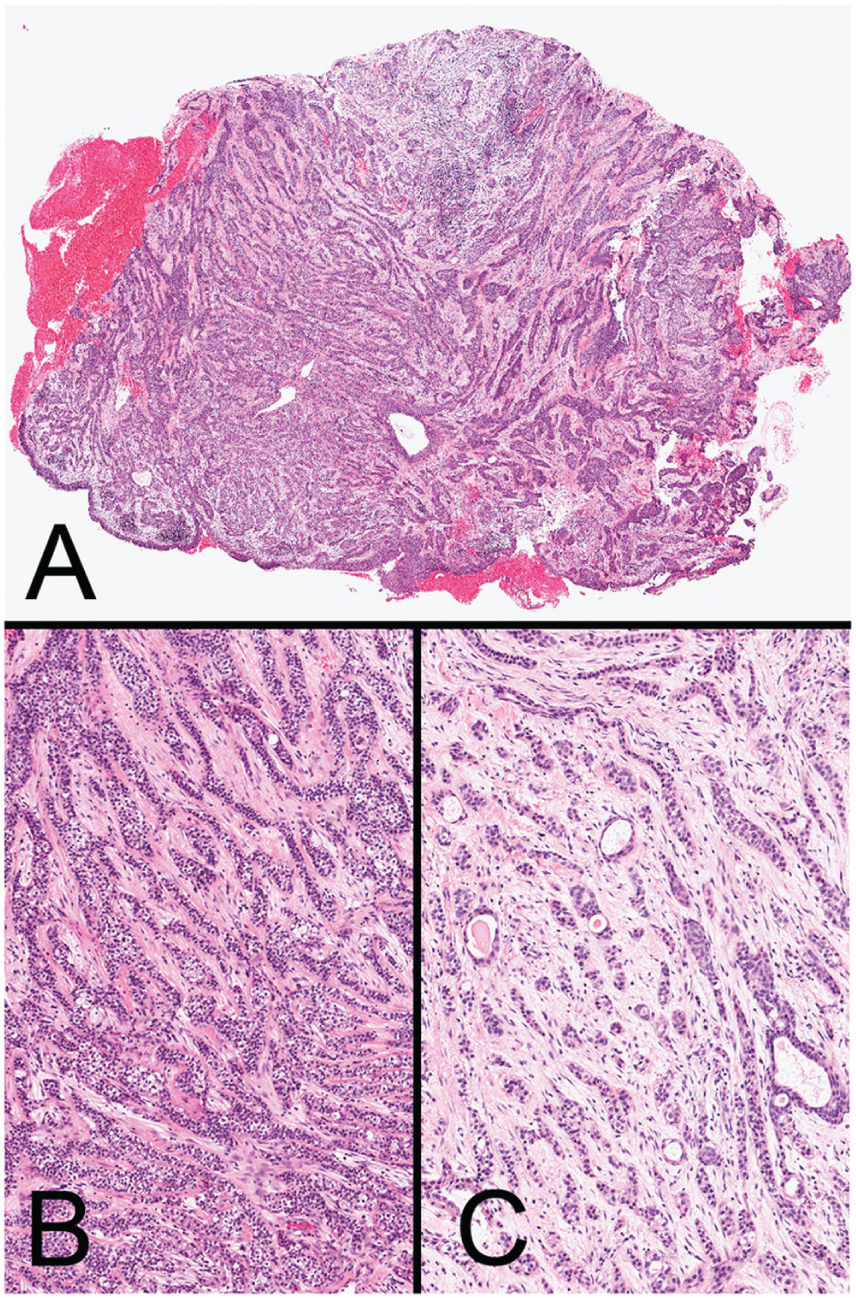
(A) Scanning magnification shows anastomosing trabeculae of neoplastic cells embedded in a fibromyxoid, hemorrhagic stroma (H&E, original magnification 16×). (B, C) Low-power photomicrographs depict various architectural patterns, including thin interconnecting cords, solid nests, and focal ductal differentiation (H&E, original magnification 100× and 150×).
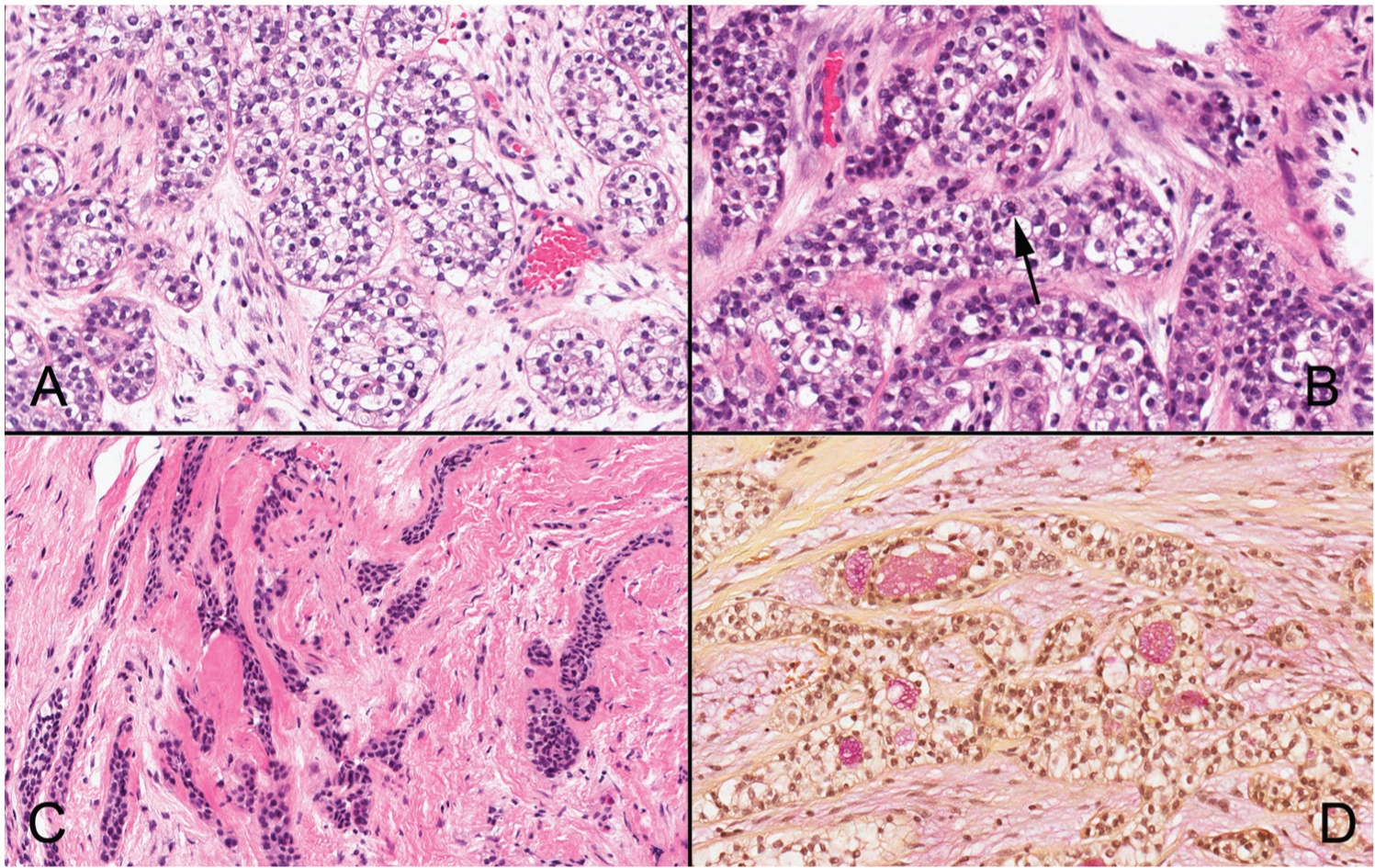
(A) Optically clear round to polygonal epithelial cells with uniform small, central nuclei are immersed in a loose fibrous or fibromyxoid stroma (H&E, original magnification 280×). (B) Rare mitotic figures (black arrow) were present (H&E, original magnification 350×). (C) Smaller, nonclear epithelial cells with eosinophilic cytoplasm and inconspicuous cytoplasmic borders in a hyalinized, desmoplastic stroma (H&E, original magnification 220×). (D) Cytoplasmic mucin observed in the clear cells (Mucicarmine, original magnification 240×).
Materials and Methods
Immunohistochemical evaluation was performed using antibodies against pancytokeratin (Dako; monoclonal; AE1, AE3), high-molecular-weight keratin (CK5/6; Ventana; monoclonal; D5/16B4), p63 (Biocare Medical; monoclonal; BC4A4), smooth muscle actin (SMA; Dako; monoclonal; 1-A4), S100 protein (Ventana; polyclonal), glial fibrillary acidic protein (GFAP; Dako; polyclonal), CD117 (Biocare Medical; monoclonal; Y145), calponin (Dako; monoclonal; CALP), and vimentin (Ventana; monoclonal; V9). All immunohistochemical stains were performed on a Ventana NexES automated system (Ventana Medical Systems, Tucson, AZ) according to the manufacturer’s instructions with appropriate positive and negative controls. Additionally, mucicarmine stain was performed for detection of cytoplasmic deposition of mucin.
Fluorescence in situ hybridization (FISH) was performed on formalin-fixed, paraffin-embedded tissue sections using a dual-color break-apart probe set (Abbott Molecular, Des Plaines, IL) to the EWSR1 (22q12) locus. Unstained 3- to 5-µm-thick paraffin sections were placed on positively charged slides. The slides were baked at 90°C for several hours, deparaffinized in SafeClear II (Fisher Scientific, Pittsburgh, PA), and dehydrated in a series of ethanol washes. After tissue digestion in a pepsin/hydrochloric acid solution, the slides were subjected to denaturation and hybridization with 8 µL probe/buffer mixture. After overnight hybridization, slides were washed, dehydrated in an ethanol series, and counterstained with 4′,6-diamidino-2-phenylindole dihydrochloride.
Results
Immunohistochemically, neoplastic cells revealed strong and diffuse reactivity for pancytokeratin AE1/AE3, CK5/6, and p63 (Figure 4A and B) and were negative for SMA, GFAP, S-100, CD117, calponin, and vimentin. Mucicarmine revealed aggregates of cytoplasmic mucin in the clear cells (Figure 3D). Finally, FISH confirmed disruption of the EWSR1 gene (Figure 5).
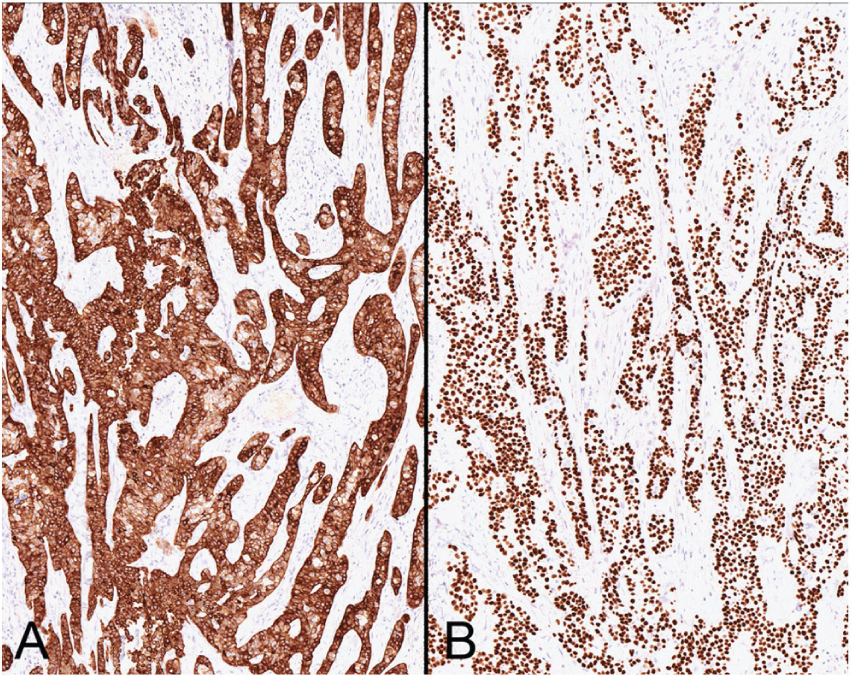
(A) Strong and diffuse cytoplasmic staining for CK5/6. (B) Diffuse nuclear staining for p63 (immunoperoxidase stain, original magnification 120×).
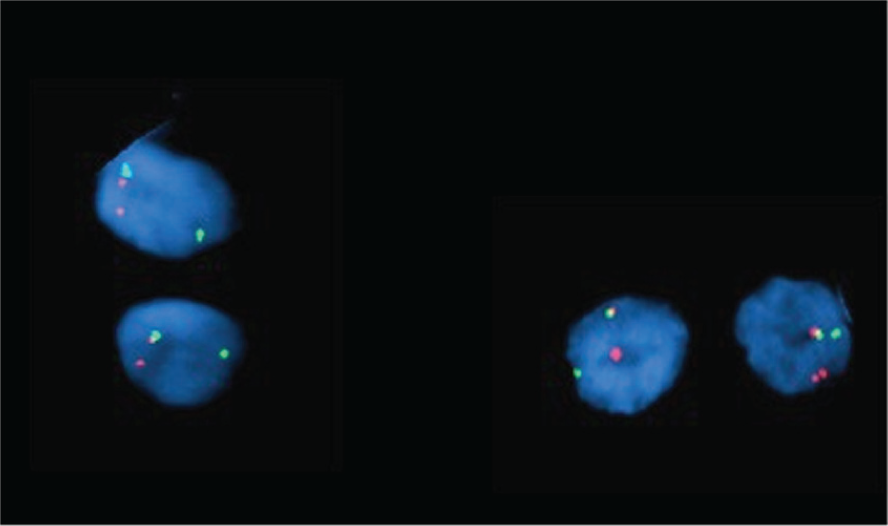
FISH for EWSR1 revealed one normal yellow signal (intact EWSR1 gene and one break-apart signal per interphase cell underscoring rearrangement of one EWSR1 gene). The break-apart probes show one separate red (5′ EWSR1) and green (3′ EWSR1) signal per cell.
The histopathologic and molecular features of the lesion were characteristic of HCCC. Surgical excision was performed; however, complete removal was not achieved due to proximity of the left carotid artery. The histologic features of the re-excised tumor were identical to those observed in the biopsy. Adjuvant radiotherapy and chemotherapy were administered.
Literature Review
A review of the English literature revealed 161 cases of HCCC,4,5,9,12 among which only 7 (4.3%) occurred in the nasopharynx. Available clinical information in the latter group is summarized in Table 1.5,6,9,12,13 Sufficient information was provided in 3 of 7 cases6,9,13; these 3 patients were women between 51 and 77 years of age.6,9
Previously Reported Cases of Nasopharyngeal HCCC and the Current Case.
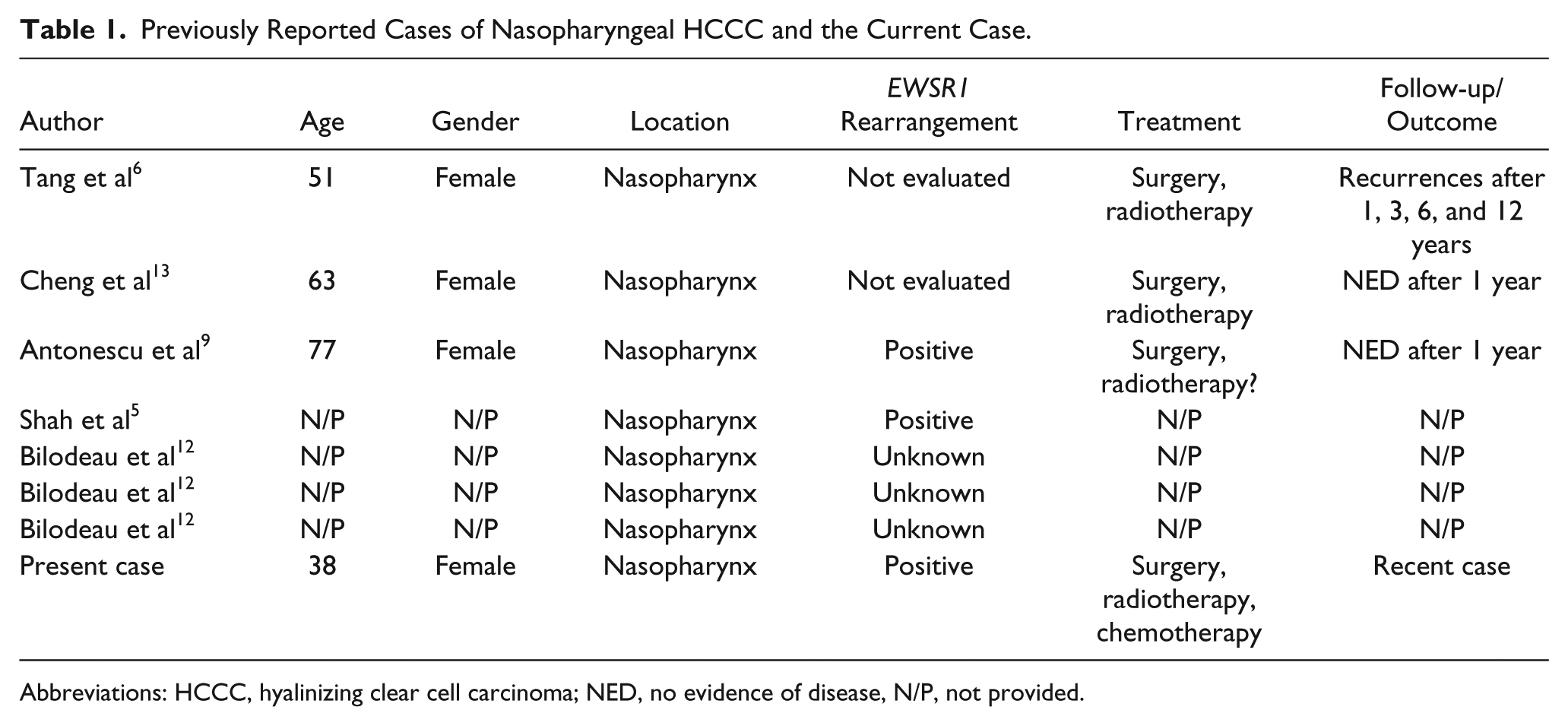
Abbreviations: HCCC, hyalinizing clear cell carcinoma; NED, no evidence of disease, N/P, not provided.
Microscopically, all 7 cases presented similar characteristics consisting of cords, sheets, and nests of clear cells embedded in a hyalinizing stroma. In the case published by Cheng et al, the cellular characteristics were those of HCCC, although no reference to the stroma was made. 13 At the molecular level, EWSR1 rearrangements were documented by FISH in 2 of 5 cases.5,9 In the series of Bilodeau et al, 12 FISH results of the 3 examples of nasopharyngeal tumors were reported collectively with tumors from other sites. EWSR1 rearrangements were seen in 92.3% of all cases. 12 Surgical excision and radiation therapy was the treatment of choice. Among patients with follow-up information, 2 were tumor-free after 12 months9,12 and one, reported by Tang et al, 6 recurred 4 times over 12 years.
Discussion
HCCC is a low-grade tumor arising predominantly in minor salivary glands of the oral cavity; it involves the palate (27.5%), tongue (25.5%), and floor of mouth (8.1%) and exhibits a slight predilection for middle-aged females (60.2%). 4 Occurrence in the nasopharynx is uncommon and accounts only for 4.3% of the cases.5,6,9,12,13
The histogenesis of HCCC is obscure. 3 CK5/6, 34βE12, and p63 positivity and the presence of intracytoplasmic glycogen, keratin tonofilaments, and desmosomes support squamous differentiation.12,14 However, occasional gland formation and the frequent presence of intracellular mucin support glandular differentiation. 15 Although this tumor displays features of squamous and glandular differentiation, it should be distinguished from the histologically and clinically more aggressive adenosquamous carcinoma.3,5
The differential diagnosis of HCCC includes clear cell oncocytoma, myoepithelioma, epithelial-myoepithelial carcinoma, myoepithelial carcinoma, clear cell variant of mucoepidermoid and acinic cell carcinoma, and metastatic renal cell carcinoma.3,4,12 Negative immunostains for myoepithelial markers in HCCC can be of help in this differential diagnosis.1-4,9
Dedifferentiation has been documented in 2 cases of HCCC; both tumors involved the base of the tongue.7,10 One occurred in a 57-year-old female 7 and the second in a 61-year-old male. 10 In the first case, widespread metastases and death occurred within 1 year of the initial presentation; in the second, local recurrence and pulmonary metastases occurred 10 months after radiation treatment.
Significant progress has been made in the identification of molecular events involved in salivary gland tumorigenesis, including the role of transcriptional coactivators, tyrosine kinase receptors, and transcription factors that control cell growth and regulate the cell cycle.9,16-18 Rearrangements of EWSR1 have been identified in 82% to 92.3% of HCCC, with ATF1 as the partner gene.9,12 The t(12;22)(q13;q12) observed in HCCC results in EWSR1–ATF1 fusion transcript; the latter is unique to this tumor and does not occur in other salivary gland neoplasms with clear cells. Hence, this molecular imprint is useful in excluding similar tumors, especially in small biopsies.
Bilodeau et al 12 investigated the molecular profile of clear cell odontogenic carcinomas of the jaws and concluded that 83.3% (5/6) of the cases harbored EWSR1 rearrangements. The aforementioned findings indicate a common histogenetic link for salivary and odontogenic neoplasms with clear cell features.
The EWSR1–ATF1 fusion is also encountered in a group of histopathologically and biologically diverse neoplasms of soft tissue origin such as angiomatoid fibrous histiocytoma, clear cell sarcoma of tendons and aponeuroses, clear cell sarcoma-like tumor of the gastrointestinal tract, as well as in a few cases of soft tissue myoepithelial tumors. 19 Therefore, although this translocation seems to play an important role in the development of HCCC, it is not unique to this tumor.
The recommended treatment for HCCC is wide local excision,2,4 followed by partial or modified neck dissection in the presence of cervical lymph node metastases.7,8 Adjuvant radiotherapy is recommended when total surgical removal of the primary tumor is not attained or for clinically aggressive tumors.7,20 The prognosis is generally good. Locoregional recurrence and distant metastases, particularly to the lung, have been recorded in 16.4% 11 to 21% 8 of the patients.
Footnotes
Acknowledgements
The authors are indebted to Dr Michelle Dolan from the Laboratory of Cytogenetics for performing the FISH study and providing the illustration and to Mr Brian Dunnette (University of Minnesota) for his assistance with the illustrations.
Authors’ Note
Drs Ceballos Sáenz and Urias Barreras were fellows at the Division of Oral and Maxillofacial Pathology, School of Dentistry, University of Minnesota, at the time of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.