
Abstract
One of the most remarkable of human neoplasms, the yolk sac tumor, is reviewed, emphasizing its histologic diversity and differential diagnosis, occurrence at many sites, and the shared passion for this unique neoplasm of Dr Gunnar Teilum (who deserves almost all credit for delineation of the nature of the tumor and its features) and Dr Aleksander Talerman (who made his own contribution to our knowledge of it) and the friendship it helped forge between these 2 distinguished pathologists. In a unique series of articles, beginning in the early 1940s, Teilum delineated the distinctive features of the neoplasm and recognized that it was 1 of 2 initially included as “mesonephroma ovarii” by Dr Walter Schiller in 1939 (the second we now know as clear cell carcinoma). Teilum named the tumor “endodermal sinus tumor” because it came to his attention that papillary formations common in the yolk sac tumor resembled the endodermal sinuses of the rat placenta. He focused on the histogenesis of the tumor and its morphologic features culminating in a classic paper in Cancer in 1959. Although Teilum and others recognized that yolk sac tumor could be a component of mixed germ cell tumors, Talerman was one of the first to emphasize that, particularly in the testis, it was common to see yolk sac tumor as a component of a mixed germ cell tumor. Teilum, working in Copenhagen, and Talerman, when the former was alive, working in Rotterdam, developed a warm friendship in part due to their great interest in the yolk sac tumor, although it also extended to other areas of gonadal neoplasia and indeed beyond the boundaries of medicine when they shared time together. The typical histologic features of the yolk sac tumor are the reticular-microcystic patterns Teilum described, but various other patterns, including solid and even rarer ones such as glandular and hepatoid, are now well known. There are some interesting variations in the age distribution of this tumor at various sites: for example, vaginal examples are almost restricted to children under 2 years of age; those of the testis that are pure also occur mostly in young boys (average age about 20 months) but are occasionally seen in later years; ovarian examples peak at about 19 years of age; mediastinal forms are mostly restricted to young adult males. Brief consideration is also given to the occurrence of this tumor at well-known extragonadal sites such as retroperitoneum, mediastinum, and pineal as well as more exotic locations. Note is made of the recently emphasized occurrence of the yolk sac tumor on the background of a somatic neoplasm, most often endometrioid carcinoma of the ovary. Given the wide ranging and fascinating clinical and pathologic aspects of the neoplasm, it is no surprise that it continues to be a source of great interest to any pathologist who sees one or more examples, and we are indebted to Dr Teilum for his monumental studies and to Dr Talerman for his own contributions.
Background
Like many, the current writer has been intrigued by the yolk sac tumor from an early stage of his career. I was privileged to see many examples as part of the good fortune of looking at cases sent in consultation to the late Dr Robert E. Scully, and during my study of these cases with him, he would often refer with fondness to Dr Gunnar Teilum (Figure 1, left), whom he got to know largely as part of the first World Health Organization group that worked on the classification of ovarian tumors. During those years I also had the good fortune to get to know Dr Aleksander Talerman (Figure 1, right), then working in Rotterdam, but who later moved to the University of Chicago, in large part because Dr Scully brought Dr Talerman’s name to the attention of those in Chicago looking for an experienced gynecological pathologist to work there. Dr Talerman would visit Dr Scully on occasion, and I quickly became aware of his own great interest in the yolk sac tumor. I knew that Dr Talerman was friendly with Dr Teilum, but the nature and strength of their relationship was subsequently heightened in a manner marked by sadness. After Dr Talerman passed away, ironically, about a week before Dr Scully died, I was in contact with Dr Talerman’s widow, Margaretha, to send a letter of condolence from Dr Scully (likely the last words Dr Scully wrote). Several months later, Margaretha kindly invited me and my colleague Dr Esther Oliva to visit her home to see if material Dr Talerman had might be of interest to us because of her wish that it be appropriately utilized and not “cast to the winds” as sadly often happens with collections left upon the death of distinguished pathologists. We were generously allowed to take whatever books, slides, and other material of diverse nature Dr Talerman had, and this included significant correspondence between him and Dr Teilum, which heightened my knowledge of the friendship the two had that has prompted this review dedicated to their memory. My comments on Dr Teilum’s career and life are brief because a detailed essay on him recently appeared in the history series of the International Journal of Gynecological Pathology. 1 It is appropriate, albeit poignant, that that was the last contribution to the literature of Dr Talerman. He and I had for many years wanted an essay on Dr Teilum in that series and finally were able to accomplish it with the assistance of Dr Teilum’s daughter-in-law. I proceed by presenting a synopsis on Dr Teilum’s contributions to the field and then those of Dr Talerman, details on his life also being recently published. 2
Dr G. Teilum (left), Dr. A. Talerman (right).
Dr Teilum’s identification of the yolk sac tumor as a distinctive neoplasm of germ cell type represents one of the classic studies in the great legacy of morphologic pathology. His writings on it will remain forever the fundamental basis of our knowledge of the histopathology of the neoplasm, and I recommend his wonderful book in which not only yolk sac tumor but also other neoplasms in both gonads are compared (Figure 2). 3
Covers of Dr A. Talerman’s copy of Dr Teilum’s book inscribed by Dr Teilum (left), book of Dr F.F. Nogales (center), and of Dr Talerman and Dr G. Jacobsen (right).
His recognition of the yolk sac tumor (which he preferred to call endodermal sinus tumor for most, if not all of, his life) from among the cases of “mesonephroma ovarii” that Schiller had described in 1939 4 is a fascinating story. In brief, in the early 1940s, Dr Teilum noted a resemblance of many of Schiller’s cases to a testicular neoplasm with distinctive features but despite that had escaped the attention of other investigators. As the testicular tumors Teilum saw had other patterns of germ cell neoplasia, mostly seminoma, Teilum concluded that the pattern Schiller had highlighted was of germ cell type in most instances.
In a series of papers over the years (all cited in Young et al 1 ) and his beautiful book, 3 considered in detail elsewhere, 5 he gradually clearly established beyond doubt the nature of the tumor and most aspects of its morphology. Teilum coined the term “endodermal sinus tumor” because in the mid-1950s he became aware that papillary structures in the tumor he was interested in resembled endodermal sinuses of the rat placenta. In 1959, Pierce and Dixon6,7 proposed the term “yolk sac carcinoma” for this neoplasm based on experimental work. It was subsequently modified and introduced in routine diagnostic practice as the now widely accepted “yolk sac tumor” (YST). There were a number of reasons Teilum’s term was not ideal including that the “endodermal sinus pattern” is only one of many and for that matter the papillae (Schiller–Duval bodies) are conspicuous in only a minority of tumors. I am not sure who coined the term “Schiller–Duval bodies,” but it was certainly used as long ago as 1963 8 and may have been first used in the paper just cited. Dr Teilum did not like the eponym considering that Schiller “got it wrong” by thinking the YST mesonephric and Duval who worked in the 19th century had no experience with this tumor and surely never saw one. However, how eponyms come about in medicine has many quirks to it and this one is surely going to remain. On the subject of names, there is at least one book in which the YST is called “Teilum tumor,” 9 and although that term did not “catch on” it would be more appropriate than many eponyms in medicine. This tumor is so remarkable that it is one of the few with a book devoted to it, the outstanding work edited by Dr F. F. Nogales in 1993 (Figure 2). 10 The authority just noted has recently written his own review of the YST, which is also recommended. 11 He suggests that the name might be more appropriate and broader if it were “primitive endodermal tumor,” but provocative though that is, a change in nomenclature although perhaps considered advisable by an expert, might lead to more confusion than desirable. His book considers the yolk sac and YST in all aspects, experimental, clinical, and standard morphological. Other excellent reviews of the yolk sac and its neoplasms have been written over the years, and one worth highlighting is that of Dr Frank Gonzalez-Crussi. 12
Just as the essay on Dr Teilum noted above can be referred to for details of his life and career, so with regard to Dr Talerman may an obituary on him coauthored by Dr Lawrence M. Roth and myself. 2 Like many whose life was affected by the Second World War and events leading up to it, Dr Talerman had an arduous childhood, including time in Siberia. He also lost his mother at an early age. After the war, Dr Talerman and his father moved to England where Dr Talerman received his medical education and met his Swedish wife. After his early years, including time at the well-known Royal Free Hospital in London (2 years of that period being an assignment in the West Indies), Dr Talerman was appointed, in 1969, the head of pathology at the Institute of Radiotherapy in Rotterdam and held that position for 10 years. He then spent the rest of his career at the University of Chicago and at Thomas Jefferson University in Philadelphia. The Rotterdam years are the ones of particular interest to us here because it was during that time that he had the opportunity to spend time with Dr Teilum and had frequent correspondence with him.
Dr Talerman’s writings on the YST were focused more on testis than other sites as far as original contributions were concerned. Others had noted admixtures of YST with other germ cell elements in testicular neoplasms previously, as Dr Talerman noted in his first paper on this topic, in which he highlighted the association of some YSTs with seminoma, 13 interestingly the admixture Teilum had first noted. Among other things this shows the somewhat simplistic nature of the split that many use of seminomatous and nonseminomatous germ cell tumors of the testis. Dr Talerman reported 3 cases of seminoma with YST, all occurring in men in the typical seminoma age range, with his 3 patients being 37, 39, and 40 years of age. In a subsequent study, he found yolk sac elements in 38% of nonseminomatous germ cell tumors, the yolk sac component being predominant in about one third of the cases. 14 In a later paper, he compared the frequency of YST components in retrospective and prospective studies and found that in the prospective series they were found in 44% of the cases compared to 29% in the retrospective cases. 15 A contribution of Talerman and associates on ovarian pathology related to the YST is of historical interest in as much as in it 16 they revisited the problem that initially led Schiller to group YST and clear cell carcinoma together. They reported a series of clear cell carcinomas of the ovary that had features overlapping to some degree with those of YST. Of particular note with regard to the link between Drs Talerman and Teilum is an excellent book Dr Talerman wrote with Dr Grete K. Jacobsen, Atlas of Germ Cell Tumors (Figure 2). 17 They chose for the cover illustration a Schiller–Duval body, and the book was dedicated to Dr Teilum. Although this work was published a quarter of a century ago, it stands very well to contemporary scrutiny and contains a wealth of useful information and the illustrations are magnificent. One of the 16 chapters is on the normal yolk sac and another on the YST.
Beginning in the early 1970s, shortly after Dr Talerman took his position in Rotterdam, he had frequent correspondence with Dr Teilum, which continued to the death of the latter. While preparing this essay I read all the letters, kindly given to me, and the enthusiasm both had for the YST almost jumped off the pages. Many other tumors of diverse types were also mentioned, not surprisingly, given the broad interest of both investigators, and Dr Talerman would alert Dr Teilum to any new case he had of mixed germ cell-sex cord stromal tumor unclassified (sometimes referred to as the “Talerman tumor”), which Dr Talerman was becoming aware of during those years. The correspondence would also include mention of summer visits of Dr Talerman to spend time exploring in Denmark with Dr Teilum and his wife. Dr Talerman became aware of Dr Teilum’s great interest in art, and in letters mention is made of Dr Talerman’s gifts to Dr Teilum of books on Degas and Turner, both received with great gratitude. I also had the opportunity to look over a small number of letters between Dr Teilum and Dr Walter Schiller. The tone of those was somewhat different, not surprisingly, as Teilum had debunked Schiller’s mesonephroma ovarii. Nonetheless, although one could sense a slight edge in the correspondence both writers were courteous in their remarks. Given my close personal association with Dr Scully for several decades, I was pleased, albeit not surprised, to find that when Dr Scully’s name was mentioned in Dr Teilum’s letters it was always in a most praiseworthy and warm manner.
General Pathologic Features
Little comment is warranted on the gross aspects of the YST, which is usually, given its malignant nature, not surprisingly, a large solid neoplasm, sometimes with cystic degeneration, and often with hemorrhage and necrosis. As it may be associated with other germ cell tumor components at most sites, careful gross examination can be crucial in identifying the second component, such as a dermoid cyst in some ovarian examples. A striking contrast to the usual obviously malignant gross appearance is provided by testicular examples, which typically look less ominous than the neoplasm seen elsewhere (see below).
The microscopic features of the neoplasm are largely the same irrespective of the site. Given its nature this tumor has been extensively illustrated over the years and only selected microscopic features are chosen due to space constraints. All readers will be aware of the role that immunohistochemistry can play in the differential diagnosis of the neoplasm. Many original papers and outstanding reviews of this topic have appeared over the years, and space issues do not allow for consideration of it here, but I draw attention reader to one very good recent review, which can be a start to study of the topic. 18
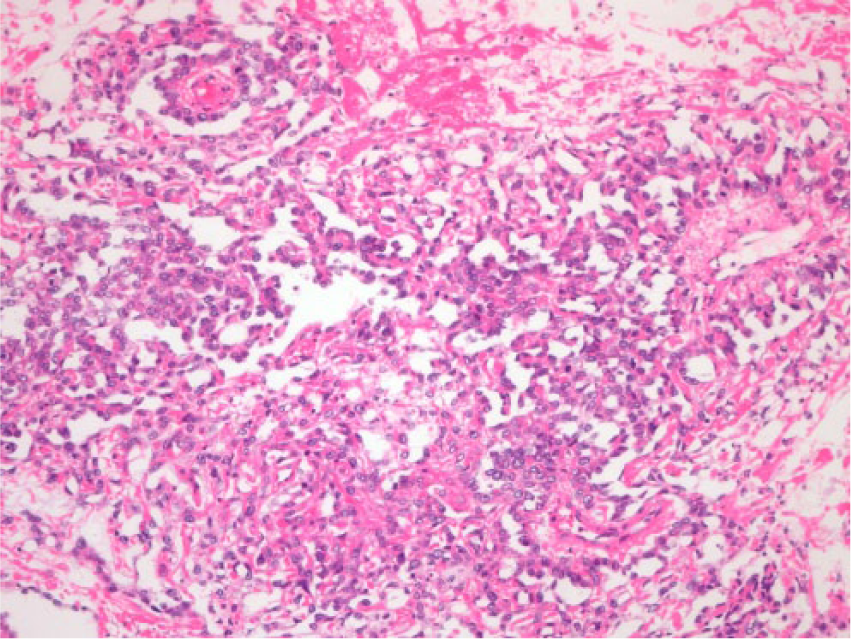
Almost all YSTs have 1 or more of 3 histologic features: a reticular (Figure 3) to microcystic pattern, Schiller–Duval bodies (Figures 4 and 5), and hyaline bodies; but the second is overemphasized and the third is nonspecific. 19 The reticular pattern consists of a loose meshwork of narrow communicating spaces lined by primitive tumor cells with variable amounts of cytoplasm that is typically clear, containing glycogen, and occasionally, lipid. When the reticular pattern produces spaces that communicate with each other in a somewhat orderly fashion, it probably accords to the labyrinthine structure that Dr Teilum described. The reticular pattern merges imperceptibly with a cystic pattern. The cysts vary from small to large and the latter may be lined by flattened, attenuated cells that appear deceptively benign. Other patterns of YST include festoon (Figure 4) and solid. 20 In the former undulating cords and columns of primitive germ cells are present at least focally in a drape-like arrangement (Figure 6). Dr Teilum mentioned a solid pattern in his writings, but to a relatively limited extent and seemed to be most taken with a pattern that had a blastema-like morphology. Recent work has emphasized a solid pattern that in the prior literature was sometimes referred to as “seminoma-like,” not unreasonably as this pattern may be difficult to distinguish on occasion from seminoma. As this issue has been discussed in detail in a recent original publication, 20 I will not belabor it here. Schiller–Duval bodies were present in up to 75% of YSTs in one series, 21 but they are not as common as this in our experience. These structures consist of papillae that vary from rounded to elongated depending on the plane of section, with a connective tissue core containing a single central vessel (Figure 5). They are covered typically by primitive columnar cells and lie in a space lined by cells that are cuboidal, flattened, or of hobnail type. These formations are usually sparsely distributed, but when numerous and closely packed, a distinctive and striking papillary pattern is created (Figure 4). The hyperchromatic, irregular large nuclei of YSTs contain variably prominent nucleoli; mitotic figures are numerous.
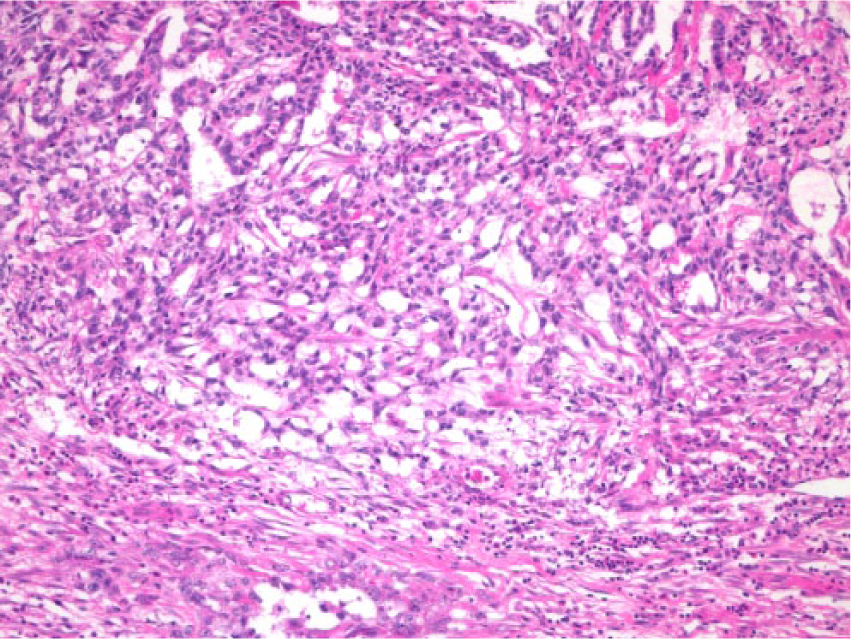
Classic reticular pattern.
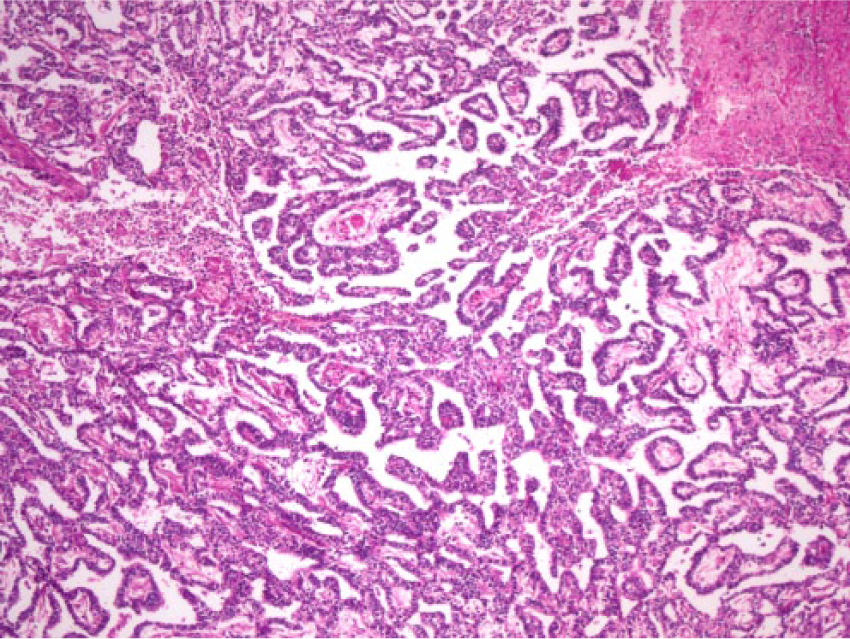
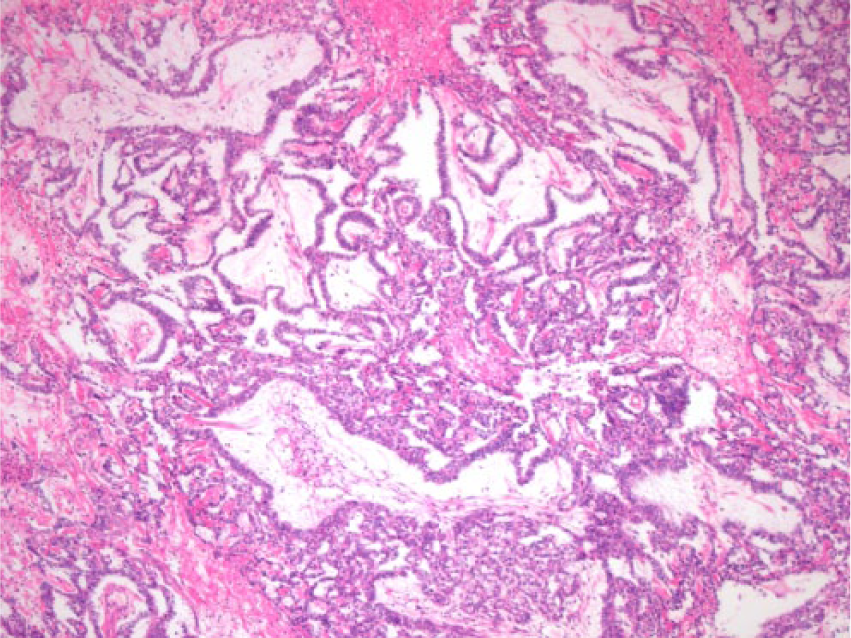
Striking papillary pattern. Some of the papillae have the features of Schiller–Duval bodies.
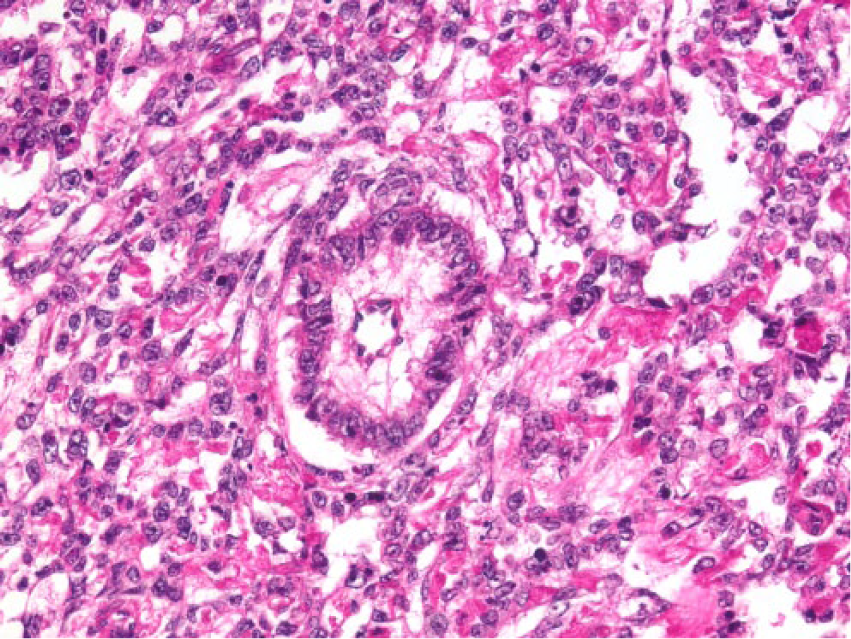
A classic Schiller–Duval body with a central blood vessel is seen in the midst of otherwise typical reticular YST.
Admixture of reticular and festoon patterns, the latter represented by the undulating cords that sometimes have a drape-like arrangement.
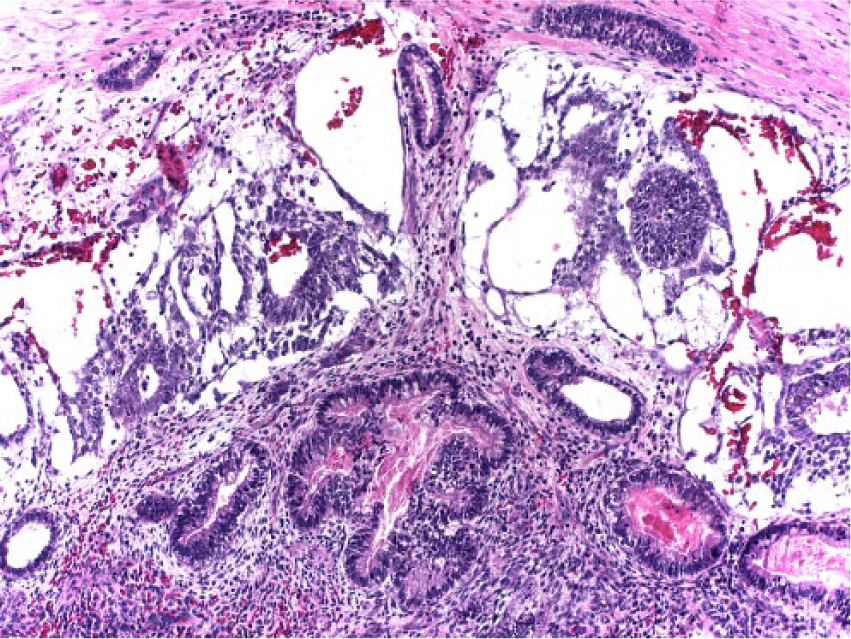
A variety of less common patterns may occur usually admixed with reticular foci, but rarely they predominate or occur in pure form. The polyvesicular vitelline pattern22,23 is typically characterized by cysts lined by columnar, cuboidal, or flattened cells and separated by a stroma that is often prominent and varies from cellular to acellular. However, nonspecific tubulo-glandular formations may also be seen (Figure 7). The cysts may exhibit eccentric constrictions simulating the division of the primary yolk sac vesicle into a larger component corresponding to the vestigial yolk sac of the embryo and a smaller component, which is the forerunner of the primitive gut. A hepatoid pattern, 24 characterized by the presence of large polygonal cells with abundant eosinophilic cytoplasm growing in compact masses separated by thin fibrous bands, resembles hepatocellular carcinoma. In some cases, glandular spaces filled with mucin impart a honeycomb pattern similar to that seen in some hepatocellular carcinomas. Since the hepatoid variant of YST was first described, we have seen few good examples indicating that it is distinctly rare, certainly less common than glandular patterns, which overall are much more problematic diagnostically.
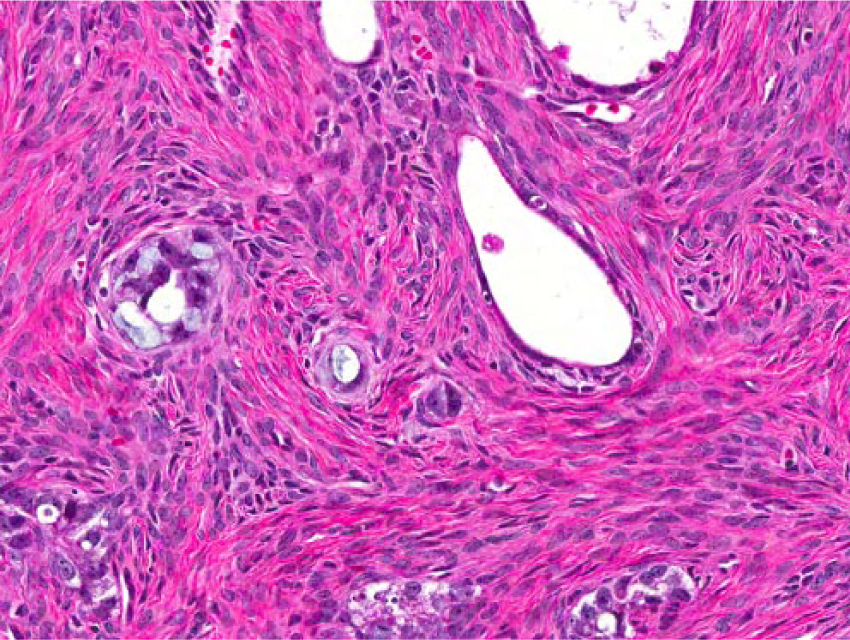
Polyvesicular vitelline pattern. A typical cyst of this pattern of neoplasia is present just off center, but the image is dominated by a tubulo-glandular pattern that falls within the spectrum of this variant.
YSTs not infrequently contain glands lined by nonspecific or vacuolated cells, and in rare tumors, a predominant glandular pattern resembling that of typical or secretory endometrioid carcinoma is seen; tumors of this type have been designated “endometrioid-like” YSTs. 25 Enteric-type glands occur in as much as 50% of YSTs but are rarely numerous. They appear as glands lined by bland mucinous columnar cells, goblet cells, and rarely, Paneth cells. In rare tumors glands of intestinal type predominate. 26
“Parietal” differentiation is characterized by extracellular accumulations of basement-membrane material, typically within reticular foci. 27 Occasional foci in YSTs are composed of tumor cells with large intracellular vacuoles that displace the nucleus (resembling liposarcoma to a degree) and some have a conspicuous loose, sometimes myxoid to collagenous stroma containing stellate spindle cells and thin walled blood vessels and rarely such foci may predominate, at least in regions. The great morphologic diversity of the YST can result in it focally or even sometimes in expansive regions, mimicking a variety of other tumors. One of the earlier papers after Schiller’s original contribution thought these neoplasms were in the family of malignant vascular tumors, so not surprisingly there may be a focal resemblance to angiosarcoma (Figure 8).
The diversity of appearances of yolk sac tumor is vast and includes foci such as that as depicted, which have some resemblance to angiosarcoma.
Immunohistochemical findings may be useful in confirming a diagnosis of YST, particularly in tumors with unusual or nonspecific histologic patterns. The cytoplasm of the tumor cells is almost always immunoreactive for α-fetoprotein (AFP) and α-1-antitrypsin, although the staining may be focal. The luminal contents of the glands and cysts in tumors with polyvesicular vitelline, hepatoid, and endometrioid-like patterns are also positive for these antigens. In recent years, glypican-3 has been established as a very helpful marker of YST, and we find it more reliable than AFP as does Dr Thomas M. Ulbright, who has great experience in this area (personal communication). Glycipan-3 is not specific but in the context of the overall differential and additional immunohistochemical results can be a very significant finding.
Yolk Sac Tumor of the Ovary
These account for approximately 20% of malignant primitive germ cell tumors and are almost as common as dysgerminomas under 20 years of age.28-31 They occur most commonly in childhood and adolescence (mean age 19 years) and are very rare over the age of 40 years when some are of somatic rather than germ cell origin (see below). Patients typically present with abdominal pain, frequently of sudden onset, and a large abdominal or pelvic mass. Almost all the patients have an elevated serum level of AFP preoperatively; measurement of its level is also useful in monitoring the effects of therapy and detecting recurrent tumor. YSTs are rapidly growing, highly malignant tumors with evidence of extraovarian spread of tumor to the peritoneum, retroperitoneal lymph nodes, or both, in approximately one third of the patients. However, the prognosis is now greatly improved due to an excellent response in most cases to chemotherapy.
The tumors are typically large with a median diameter of 15 cm. The external surface is usually smooth and glistening, although 25% have ruptured. The sectioned surfaces are typically solid and cystic and composed of soft, friable, yellow to gray tissue; very rare tumors are entirely cystic. Extensive areas of hemorrhage and necrosis are common. A honeycomb appearance due to the presence of many small cysts may indicate the presence of a polyvesicular-vitelline pattern. YSTs are virtually never bilateral unless the opposite ovary is involved as part of generalized peritoneal spread. Occasional tumors are associated with a dermoid cyst or coexist with a dysgerminoma. In both these circumstances the 2 components are often grossly recognizable, although in some cases there may be only microscopic evidence of a non-YST component.
Clear cell carcinoma is the ovarian tumor most commonly confused with a YST as shown by the initial grouping of the 2 types as one. 4 The differing age distribution of clear cell carcinoma and YST is an initial helpful aspect of many cases. The gross can also be helpful in some cases should clear cell carcinoma be associated with an endometriotic cyst or recognizable adenofibroma component or, conversely, YST associated with a dermoid cyst. One reason the 2 types of tumor may be confused microscopically is that clear cell carcinoma may have a loose, edematous appearance simulating the reticular pattern of a YST and both tumors may be papillary and contain hyaline bodies. The nuclei in YSTs, however, are almost always more primitive in appearance than those of a clear cell carcinoma, and their papillae typically contain a central vessel and lack the hyalinized eosinophilic core that is characteristic of the papillae in some clear cell carcinomas. Other typical patterns of clear cell carcinoma or endometrioid foci (assuming the glands are not primitive and the endometrioid-like glands of YST) of course help exclude the diagnosis of a YST. Conversely, the presence of foci of other types of germ cell neoplasia exclude the diagnosis of clear cell carcinoma. The immunohistochemical demonstration of AFP or glypican-3 favors the diagnosis of YST but occasional clear cell carcinomas may stain similarly,32,33 so this finding is not absolute. Another neoplasm that may be in the differential diagnosis is the Sertoli–Leydig cell tumor. This is in part because the latter occurs usually in young females and occasionally a Sertoli–Leydig cell tumor has microcysts that can potentially suggest the reticular-cystic pattern of YST. Further confusion may be caused rarely by the clinical background inasmuch as occasional Sertoli–Leydig cell tumors are associated with an elevation of the serum AFP, although it is rarely to the level seen in cases of YST. Despite limited morphologic overlap as just noted, there are so many differences in the morphology of the 2 tumors that any thoroughly sampled neoplasm in either category should be readily distinguished from the other. Another rare issue in differential diagnosis with a sex cord tumor occurs in some cases in which cystic neoplastic follicles of a juvenile granulosa cell tumor may impart a superficial resemblance to the polyvesicular vitelline pattern of YST. However, thorough sampling will enable a distinction between these 2 neoplasms to be made and if necessary of course immunohistochemistry will show overt different staining results. Yet another issue in differential diagnosis with sex cord-stromal tumors is related to the fact that many of the latter neoplasms, just like YST, occur in young people and occasionally such persons will be pregnant. Specifically, when sex cord-stromal tumors are discovered in pregnancy, they often have a variety of changes that can make the differential diagnosis challenging. The one of specific interest here is intercellular edema, which may impart a loose arrangement of the cells confusable with the reticular pattern of YST. 34 Awareness of this problem and judicious sampling should show distinctive features, and if necessary immunohistochemistry may again be applied. Distinction from the exceedingly rare embryonal carcinoma of the ovary should be relatively straightforward based on standard well-known differing features of the 2 neoplasms. An occasional gland in a YST may out of context look like a gland of embryonal carcinoma and is allowable for YST, but of course if there is any confluent aggregate of such glands, in addition to typical YST, a diagnosis of malignant mixed germ cell tumor would result.
The distinction between hepatoid YST and the rare hepatoid carcinoma of the ovary is based on both clinical and pathologic differences. The hepatoid carcinoma has occurred in older women with an average age of 63 years in contrast to the young age of patients with hepatoid YST. The hepatoid carcinomas have not been associated with typical foci of yolk sac neoplasia or any other neoplastic germ cell component. The hepatoid carcinomas also may have small foci in the primary or metastatic tumor indicative of a tumor of common epithelial origin rather than a yolk sac nature. Clinical findings, bilaterality of these ovarian tumors, and lack of foci of typical yolk sac neoplasia generally help distinguish a metastatic hepatoma in the ovary from a hepatoid YST.
Yolk Sac Tumor of the Testis
The first testicular tumor recognizable as YST (it occurred in a 15 month old) was reported in 1910. 35 However, YST of the testis essentially went unrecognized as an entity until Teilum became aware of it during the early to mid-1940s as part of his detailed observations as discussed in detail elsewhere. 1 The distinctive features of this tumor appeared to escape the keen eye of the distinguished pathologists who contributed so much to testicular pathology in the decade after the Second World War, it being considered, if noted at all, just a variant of embryonal carcinoma, the so-called infantile form or even just infantile adenocarcinoma. It was only in 1951 and again in 1956 that Magner and colleagues36,37 contributed first 2 cases and then a series with 5 additional tumors to this type to the literature and in their second paper referenced the observations of Teilum. They and other writers 38 for some years used various terminologies before the yolk sac designation became settled upon in the late 1960s to early 1970s. 39 In the paper just noted, it is pertinent to mention that one of their patients with an apparently pure YST was an 82-year-old man, in great contrast with the predominant occurrence of pure tumors in very young boys. It is of some historical interest that in the next good paper on this topic after that of Magner, the authors, Teoh et al, 38 had the opportunity to study the case reported by White, it having been passed onto them by an illustrious figure in the history of gonadal pathology, Albert Peyron, who made seminal contributions to our knowledge of polyembryoma (see below).
There are some differences between testicular and ovarian YSTs. Testicular examples peak at about 2 years of age, being progressively less common as children move through the first decade, being uncommon in the second decade, and rare thereafter, but of course in older patients, seen as part of a mixed germ cell tumor. There is some evidence in the literature that YSTs in young boys (under 2 years) have a natural history that is more indolent than in older males and in females. It is conceivable that in some of the older series confusion of YST with juvenile granulosa tumor (see below) explained the good outcome, but that can surely not explain the entirety of the difference in prognosis between the tumor in young boys and older patients and females.
YSTs of the testis are usually well circumscribed and dominantly solid and characteristically tan-yellow to gray.37-41 They may have a mucoid quality and occasionally small cysts are present. They may be indistinguishable on occasion from seminoma, which is however exceptionally rare in the first decade. The microscopic spectrum for practical purposes is as already described, although perhaps based on our anecdotal experiences glandular patterns may be sometimes more common in the testis.
There are also some differences in the differential diagnosis of testicular YST compared to the ovarian form because in the testis one does not for practical purposes see clear cell carcinoma, which is one of the more common issues in the ovary. In young boys the differential diagnosis with juvenile granulosa cell tumor can be problematic but the latter neoplasm occurs even earlier, usually before 6 months, than YST. The majority of juvenile granulosa cell tumors have obvious follicular differential, enabling distinction from YST, but when follicles are absent or inconspicuous the mitotic activity, which is characteristic of the juvenile granulosa cell tumor of the gonads in general, can potentially result in an error in diagnosis, particularly if there is some separation of the tumor cells somewhat reminiscent of reticular YST. Of course, immunohistochemistry will be definitive if obtained. It is highly likely that before the juvenile granulosa cell tumor of the testis was popularized occasional examples were misdiagnosed as YST. We have not seen a pure example of polyvesicular vitelline YST in the testis. Other differential diagnostic considerations are mainly with other forms of germ cell neoplasia, particularly embryonal carcinoma and seminoma in the case of so-called solid YST. Both are rare in children, and these issues have been addressed in many sources in the literature and are not repeated here. Other aspects, including the behavior of YST of the testis, are reviewed elsewhere. 42
Mixed Malignant Germ Cell Tumors
Mixed malignant germ cell tumors account for approximately 8% of malignant primitive germ cell tumors of the ovary. 43 They account for an even greater percentage (approximately 33%) of germ cell tumors of the testis, and it is very common in mixed germ cell tumors of the testis to find minor foci of YST as Talerman’s work cited earlier indicates. In females, the commonest malignant mixed germ cell tumor is probably the admixture of dysgerminoma with YST. The 2 components may be grossly recognizable in some cases, but in many it is only microscopic evaluation that discerns minor foci of one or the other. The intriguing association of some YSTs of the ovary with a dermoid cyst does represent a “mixed germ cell tumor,” broadly speaking but it is not a mixed malignant germ cell tumor because, obviously, the dermoid cyst is benign. This admixture of benign and highly malignant is yet another intriguing aspect of the pathology of the YST. Another form of mixed germ cell tumor with a YST component is when it is associated with an immature teratoma. This is probably the second commonest form of malignant mixed germ cell tumor, after YST and dysgerminoma, in the ovary. Any high-grade immature teratoma of the ovary should be rigorously sectioned to exclude minor foci of YST, and if embryoid bodies are present, finding YST on rigorous sampling is even more likely for the reasons noted in the next section. In both gonads a YST component can be seen with essentially any admixture of any other germ cell tumor components in varying amounts.
Polyembryoma
This neoplasm has its own interesting story, and just as Teilum is largely responsible for knowledge on the YST so the French investigator Alfred Peyron is largely responsible for the foundation knowledge on this intriguing entity. 44 After his initial observations, Peyron continued to work on this neoplasm for the rest of his life and wrote many additional papers as summarized in one of a number of excellent original contributions on the topic that have sporadically appeared over the years. 45 One of these 46 appeared in a supplement to one of the major journals honoring Dr Gunnar Teilum and as the fundamental unit of the polyembryoma, the embryoid body, contains yolk sac epithelium linkage is appropriate. Embryoid bodies must be one of the most fascinating of all structures in neoplasia, and those interested in learning more about them may consult yet another paper, 47 which is beautifully and profusely illustrated.
The polyembryoma48-50 is characterized by a dominant content of embryoid bodies resembling to varying degrees normal early embryos (Figure 9). Embryoid bodies have as part of their structure yolk sac epithelium, but they are also associated with embryonal carcinoma-type epithelium in the germ disc. This leads some to consider the polyembryoma a special form of mixed germ cell tumor, a not unreasonable position, but their special nature puts them in a unique category. The issue of the approach to this rare neoplasm is made further debatable by the fact that in the vast majority of cases that have been encountered to date there is a component of teratoma (Figure 9). It is for that reason that Dr Robert E. Scully felt these represented the most high-grade of all possible high-grade forms of immature teratoma and that approach is gaining some traction. Because these tumors contain trophoblast, they may be associated with elevated levels of HCG and related endocrine manifestations; the serum AFP level may also be increased.
Polyembryoma. Numerous embryoid bodies (top), which when imperfectly formed, often appear as cysts lined by yolk sac epithelium, but punctuated by darker staining epithelium of embryonal carcinoma-type. Teratomatous glands (bottom) are usually present in this neoplasm and are why some consider polyembryoma an extremely immature teratoma.
Extragonadal Yolk Sac Tumors
I now note a few aspects of this topic based on a review I coauthored with Dr Philip B. Clement in the book edited by Nogales. 10 We listed in that contribution all the known sites (as of that time) of extragonadal YSTs, and although there have been sporadic reviews and case reports since that time it is doubtful if anything of note has changed. By far the greatest number of tumors occurred in the presacral and sacrococcygeal region with the next most common sites being the thorax (almost all the mediastinum), female reproductive tract outside the ovary (the great majority the vagina), brain (mostly pineal), and retroperitoneum. Rare sites that accounted for more than 3 examples included the orbit (6), face (5), stomach (6), and liver (4). If the perplexing features of the YST were not already plentiful given the diversity of its histopathology, it is even more added to by some remarkable differences in the age distribution of certain of the extragonadal neoplasms. For example, the YST of the vagina is a distinctive tumor of very young girls being exceptionally rare in patients beyond 2 years of age. 51 Sacroccygeal examples also occur in very young children for the most part. On the other hand, mediastinal examples, virtually restricted to males, typically occur in young adults. As would be anticipated the differential diagnosis of extragonadal tumors varies in a site-specific manner. For example, in the vagina a limited biopsy sample showing only solid YST in which the cells have scant cytoplasm could conceivably suggest a possibility of embryonal rhabdomyosarcoma, a differential that rarely comes up at other sites. In the mediastinum, the differential diagnosis in a biopsy between YST and germinoma is not uncommon, particularly as germinoma of the mediastinum is a neoplasm encountered with some frequency.
Yolk Sac Tumor of Somatic Type
This final aspect enhances the remarkable nature of the YST. Just as choriocarcinoma is well known to occasionally arise from carcinoma, now it is appreciated that less often YST arises out of carcinoma. Although this potential probably exists anywhere it is documented most in the ovary, and the single largest experience is a report of 6 cases complicating endometrioid carcinoma. 52 Cases of this type, which tend to be seen in the postmenopausal age group because endometrioid carcinomas are usually seen in those years, are an exception to the rule that YST is usually a neoplasm of the young. One can occasionally get nonspecific patterns in endometrioid carcinoma that might at first glance simulate a YST to a limited degree and immunohistochemistry is particularly warranted in these cases to exclude YST.
Concluding Remarks
It has only been possible in the space available to “scratch the surface” of the numerous intriguing clinical and pathologic aspects of the YST. For example, 2 upcoming publications will discuss among other things a sarcomatoid morphology of likely yolk sac derivation, in some cases being seen after chemotherapy.53,54 As more experience with treated YSTs accumulates over the years doubtless other vagaries of morphology will be encountered. As long as morphologic observation plays a major role in guiding clinical care, those who encounter examples of this remarkable neoplasm will be intrigued by its remarkable diversity, overlap with aspects of embryology and anatomy, and remarkably broad differential diagnosis. That this tumor, with the exception of a subset occurring in the testis of young boys, is in the great majority of cases inherently aggressive, is now in most cases curable, represents one of the great advances in medical therapy of the past several decades.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.