
Abstract
Peritoneum is a site for both primary and secondary tumors. Primary peritoneal tumors are fairly rare. The most common primary tumors of the peritoneum are malignant mesothelioma and serous papillary adenocarcinoma. Clear cell carcinoma of the peritoneum is extremely rare and often misdiagnosed as mesothelioma, serous carcinoma, or metastatic adenocarcinoma, so it represents a diagnostic challenge for both clinicians and pathologists. Up to date, to the best of our knowledge, only 11 cases of primary peritoneal clear cell carcinoma have been reported in the English literature. Distinguishing this tumor of the peritoneum versus ovarian carcinoma can be problematic. Herein, we report a rare case of primary peritoneal clear cell carcinoma occurring in a 49-year-old woman, along with a review of the literature.
Keywords
Introduction
Clear cell carcinoma (CCC) is common in the ovary and endometrium; it shows a typical morphology, characterized by large tumor cells with clear cytoplasm and hobnail features, arranged in tubulo-cystic, papillary, or solid-sheets patterns. It usually arises from foci of endometriosis and is considered a high-grade tumor with a poor prognosis at diagnosis. 1
Primary peritoneal clear cell carcinoma (PPCC) is very rare. It was firstly described in 1990, 2 and so far only 11 cases have been reported in the English literature.2-11 Therefore, very little is known about the biological behavior of this lesion, and the appropriate patient management is not straightforward. Herein we report a new case of PPCC along with a review of the literature.
Material and Methods
On February 2013, a 49-year-old woman was referred to our hospital for an abdominal mass.
Her family history was negative for cancer, and 3 caesarean sections and an appendectomy were reported in her past medical history. Moreover, she had undergone to a right salpingo-oophorectomy 15 years before, with a histological diagnosis of benign ovarian cyst. The patient presented with a painful, asymmetric, irregular, upper abdominal solid mass, with an overlying erythematous skin. An abdominal ultrasonography and a computed tomography scan revealed a huge, polylobulated mass, 10 × 12 cm in size, with both solid and cystic features on section, close to median raphe, infiltrating the left rectus muscle and compressing small bowel. The patient underwent debulking surgery removing the mass, the adherent ileal segment, the left colic omentum, and the left ovary. Grossly, a 9.5 × 9 × 7 cm mass, adherent to the external surface of the ileum, was found; on cut section, the tumor showed microcystic and solid features (Figure 1).
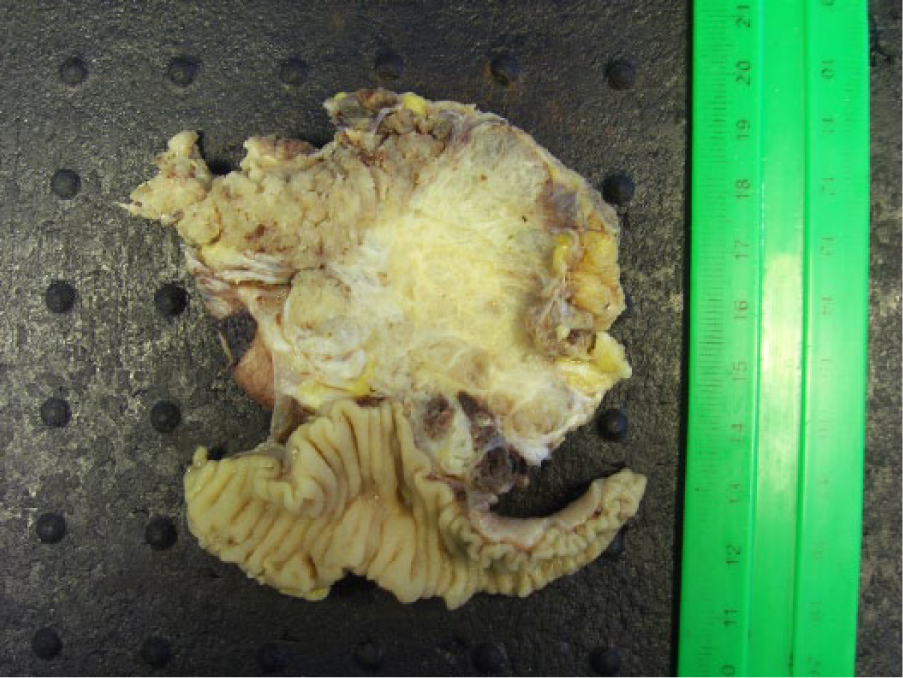
On cross section the tumor mass showed microcystic and solid features adherent to the ileum segment.
No gross evidence of tumor involvement was found in the other specimens (omentum and left ovary). Histologically, the tumor was composed of neoplastic cells with clear cytoplasm and hobnail features, with cystic and papillary growth pattern. In the papillary areas, the tumor cells showed slightly pleomorphic nuclei, with increased mitotic rate (Figure 2). Immunohistochemically, the neoplastic cells were strongly positive for Ck7 (Figure 2) and focally positive for PR and vimentin; they were negative for thrombomodulin, Ber-EP4, Ck5/6, CA19-9, Leu-M1 (CD15), Ck20, ER, WT-1, CA125, CD10, RCC, and TTF1. The tumor infiltrated the serosa of the ileum; neither tumor was found in the left ovary and in the omentum; extensive sampling of the specimen did not identify any focus of endometriosis. The morphology and immunophenotype were consistent with a CCC that we hypothesized primary of the peritoneum. To confirm this diagnosis, all slides of the previous right oophorectomy were reviewed in consultation in our Laboratory of Surgical Pathology, and the diagnosis of benign ovarian cyst was confirmed. So a definitive diagnosis of PPCC was made. Six months later, on follow-up, a positron emission tomography (PET) detected an involvement of a left inguinal lymph node. The patient underwent to a total hysterectomy, and the left inguinal lymph node was excised. Histologically, the lymph node showed a metastasis from CCC (Figure 3); the uterus was free of neoplasia. On August 2013, the patient started 6 cycles of carboplatin and taxol chemotherapy. On the last follow-up in July 2014, the patient was still alive and disease-free.
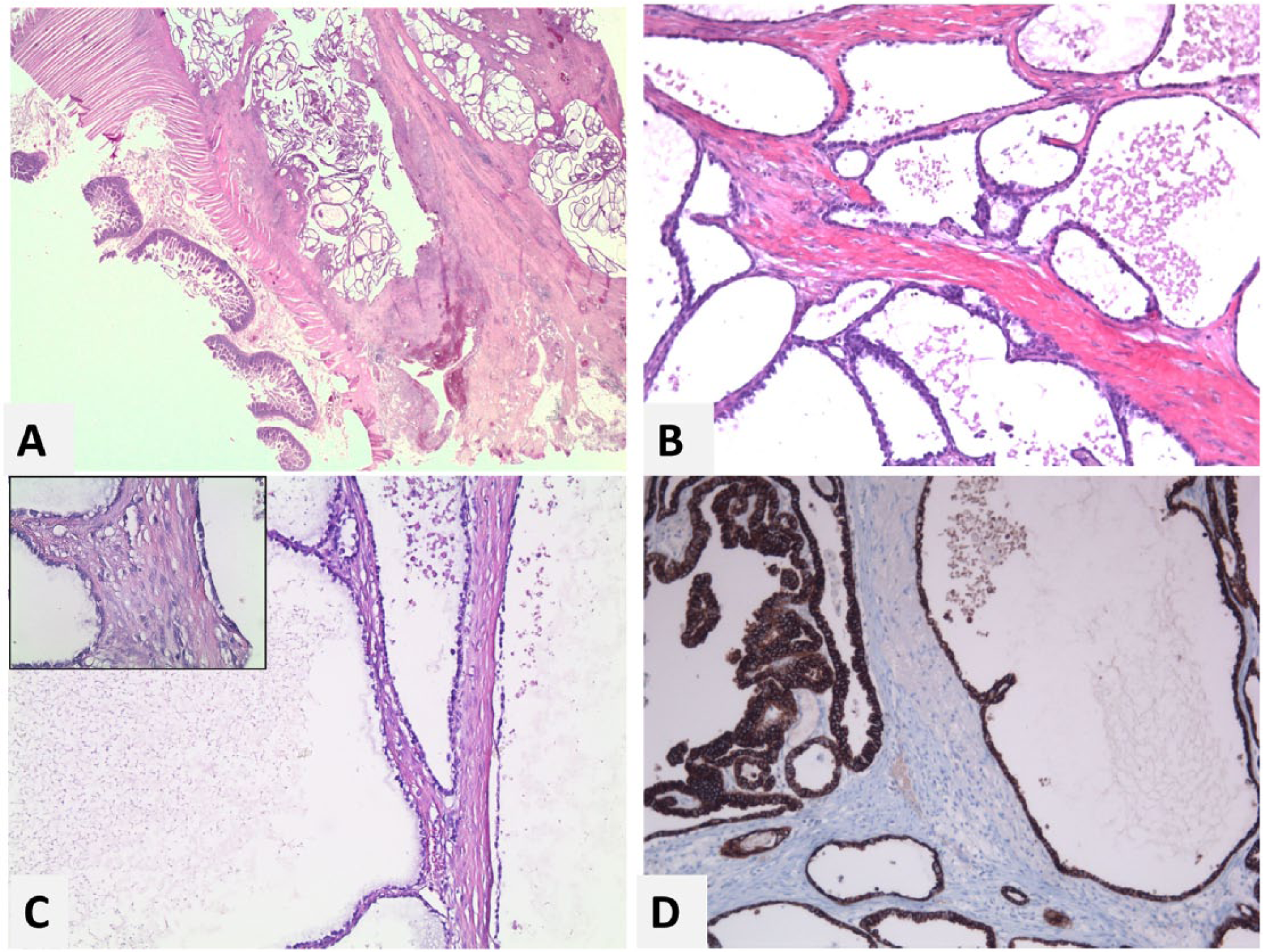
(A) The mass infiltrated the serosa of the ileum (hematoxylin–eosin stain [H&E], 10×). (B, C) The tumor showed a cystic clear cells tumor (H&E, 106×; inset 630×). (D) Immunohistochemically the neoplastic cells were strongly positive for Ck7 (106×).
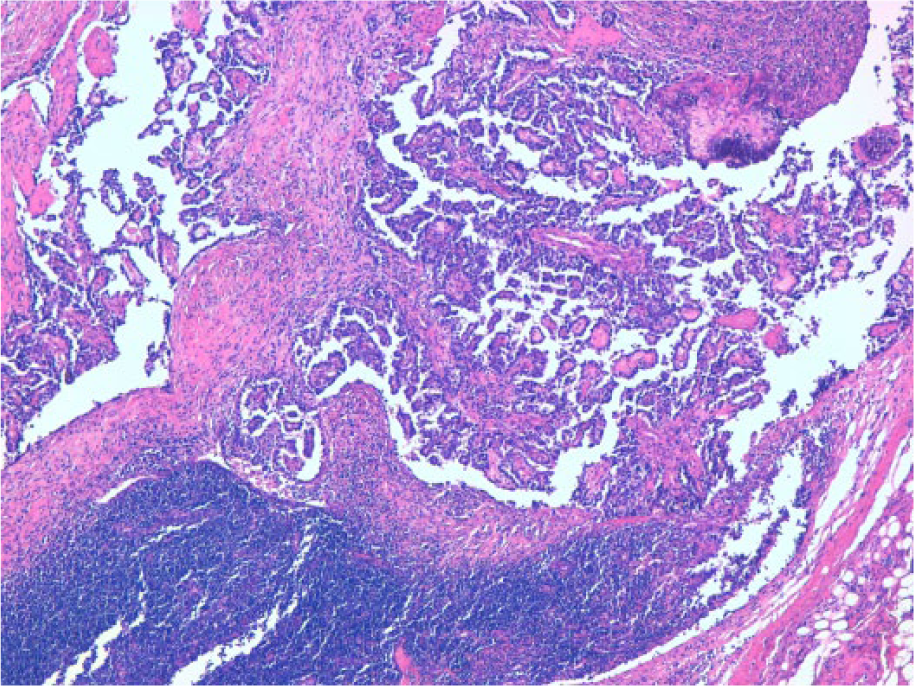
Metastatic inguinal left lymph node (H&E, 200×).
Discussion
Primary peritoneal tumors are uncommon neoplasms that arise from the mesothelial or submesothelial layers of the peritoneum. The most frequent tumors of the peritoneum, although rare, according to the new World Health Organization classification of tumors of female reproductive organs, are mesothelial tumors, epithelial tumors of Mullerian type, and, among these, primary peritoneal serous carcinoma, leiomyomatosis peritonealis disseminata, and desmoplastic small round cell tumor. 12 PPCC is extremely rare, accounting for about 3% of primary peritoneal carcinomas. 11 Distinguishing this tumor of the peritoneum versus carcinoma of ovarian origin can be problematic. The diagnosis of primary peritoneal tumors is based on the Gynecology Oncology Group criteria originally described for primary adenocarcinoma of the peritoneum. 13 The same criteria can be applied to the PPCC and are as follows:
Both ovaries should be normal in size or enlarged by benign condition.
The involvement in extraovarian sites must be greater than that on both ovarian surfaces.
Microscopically, the ovarian findings should be as follows: Ovaries should not be involved by disease The ovarian involvement must be confined to surface epithelium with no evidence of cortical extension The disease involves ovarian surface and the cortical stroma, but with tumor size must be less than 5 × 5 mm2
The histological and cytological features of the tumors should be predominantly of serous type, that is, similar or identical to ovarian serous papillary adenocarcinoma.
In cases with prior oophorectomy, the previous pathology report stating that the ovaries were normal should be available, and if possible, all slides should be reviewed. 14
According to the traditional model of ovarian carcinogenesis, the ovarian surface mesothelium, in case of ovarian tumors, and the mesothelium, in case of primary peritoneal cancers, was considered the cell of origin for serous neoplasia, through a Mullerian metaplastic change and subsequent neoplastic transformation.12,15 Recently, based on studies on salpingo-oophorectomy specimens in women with BRCA mutations, 16 origin from tubal epithelium has been proposed for serous carcinomas, as alternative etiopathogenetic theory. 17 Serous tubal intraepithelial carcinoma has been considered the epithelial precursor lesion of ovarian carcinoma, and it is thought to be the earliest known manifestation of most pelvic serous cancers.12,18 Another pathogenetic hypothesis is represented by the possibility of a field change in native or metaplastic tubal-type epithelium resulting in multifocal lesions.12,19 Pathogenesis of CCC is yet unknown, but it has been, now, well established with a strong association between endometriosis and the development of the tumor. 14 Malignant transformation of endometriosis was, first, well documented by Sampson who proposed 3 criteria for the diagnosis of this process: (a) the endometriosis is closely associated with the tumor, (b) the histology suggests an endometrial origin, and (c) no other primary neoplasm sites are found. 20 The data in the literature established that malignant tumors arising in endometriosis often show clear cell or endometrioid histopathology.8,21-23 Regarding the pathogenesis of PPCC, interestingly in 1000 cases of endometriosis, it was identified in approximately 1% of the cases with extraovarian endometriosis, and CCC and adenosarcoma as the most common histotypes. 22 Moreover, in a study of 115 cases of endometriosis with concurrent intraperitoneal tumors, 21 were extraovarian cancers: clear cell and endometrioid morphology were the most frequently patterns. 23 Recently, it has been well established by morphologic and molecular genetic studies that CCC of the ovary develop from endometriotic cysts. In particular, ARID1A mutation occurs in approximately 50% of ovarian CCC and in 40% of ovarian endometrioid carcinoma, as well as in 30% of uterine endometrioid carcinomas.24-28 ARID1A encodes for BAF250a, a chromatin remodeling protein responsible for several nuclear activities involving transcription, DNA methylation, DNA synthesis, and damage repair. 24 Loss of ARID1A expression has been demonstrated in CCC and in the adjacent so-called “atypical endometriosis,” considered a precursor of Endometriosis-related Ovarian Neoplasms (ERON)24,27 and is an early molecular event in tumor progression from endometriotic cyst to CCC, together with other molecular alterations such as activating mutation of PIK3CA.29-31
The precise origin of endometriosis is yet unestablished, whether it develops in situ in the peritoneum or from retrograde menstrual flow. However, very interesting is the observation that eutopic endometrium in women with endometriosis shows intrinsic molecular abnormalities, including activation of oncogene pathways that presumably permit the endometrial tissue to implant, and invade ovarian and peritoneal tissue. 17 Finally, in a very recently described article, the authors reported some very important guidelines for assigning the primary site of origin of the tumor. Accordingly, the present case should be categorized as primary peritoneal carcinoma. 32
Table 1 shows a summary of the 11 previously reported PPCCs along with our case. The average age was recorded as 54.41 years, ranging from 37 to 67 years. Endometriosis was present in 4 cases (33.3%). On imaging, 8 cases, including our case, showed a cystic mass with solid components.
Clinicopathologic Findings of the Patients With PPCC.
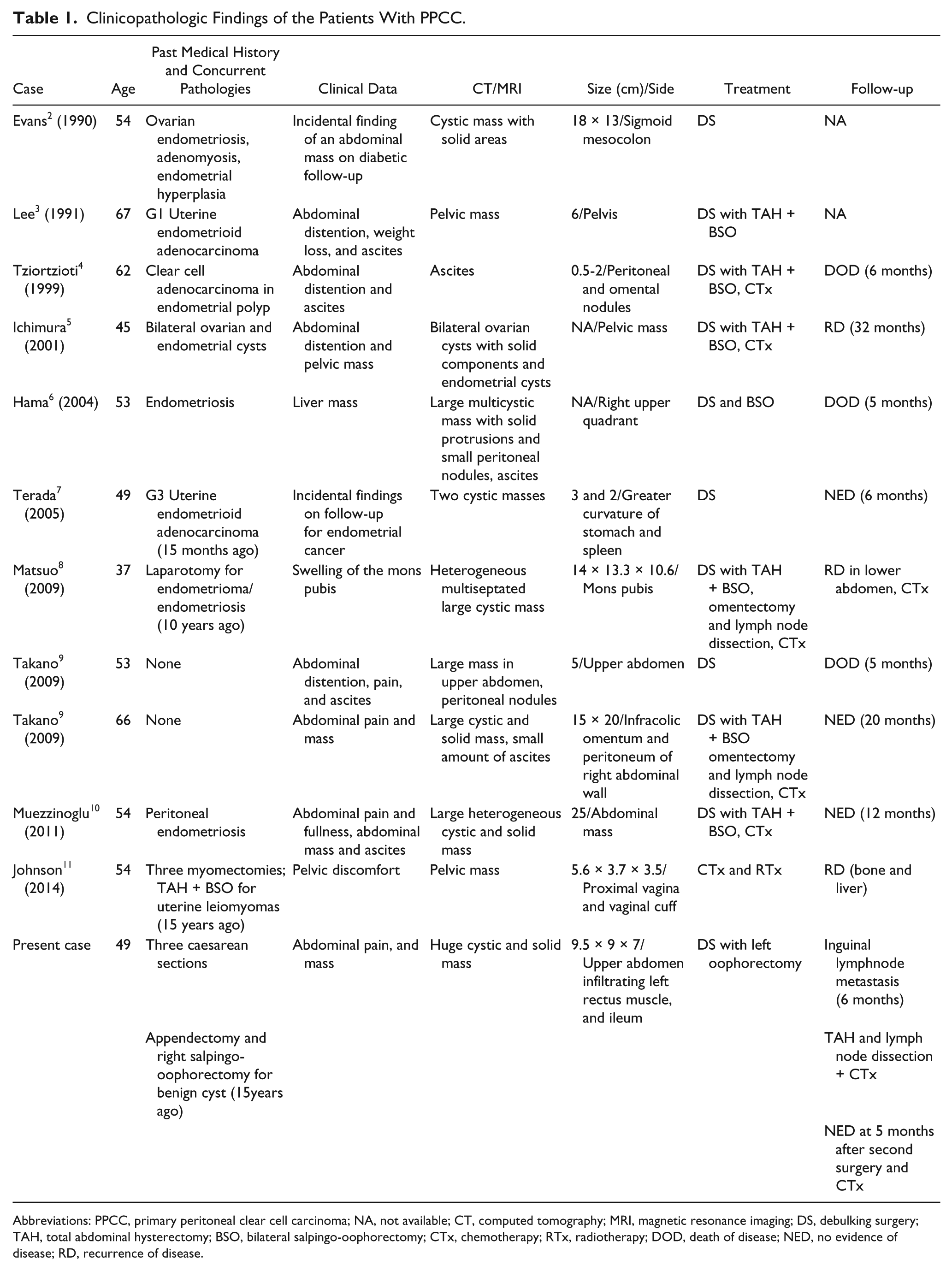
Abbreviations: PPCC, primary peritoneal clear cell carcinoma; NA, not available; CT, computed tomography; MRI, magnetic resonance imaging; DS, debulking surgery; TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; CTx, chemotherapy; RTx, radiotherapy; DOD, death of disease; NED, no evidence of disease; RD, recurrence of disease.
In every case, the treatment consisted of debulking surgery, followed by chemotherapy, except in one case that was considered inoperable and was treated with chemotherapy and radiotherapy.
The differential diagnosis of PPCC is with mesothelioma, peritoneal serous adenocarcinoma, metastatic yolk sac tumors, and metastatic renal cell carcinoma. Mesothelioma occurs in the elderly or middle-aged women, shows a tubular and papillary growth pattern with cuboidal cells, characterized by scanty to moderate eosinophilic cytoplasm and slight nuclear atypia. Immunohistochemistry is essential to support the diagnosis; in fact, calretinin, Ck5/6, and thrombomodulin are the best positive markers for differentiating epithelial malignant mesothelioma from ovarian carcinoma diffusely infiltrating the peritoneum being strongly expressed in malignant mesothelioma.8,33 Serous adenocarcinoma shows an extensive papillary appearance, may contain psammoma bodies, and generally expresses WT1.
Yolk sac tumors often have a festoon pattern of growth with Schiller-Duval bodies, 8 they stain focally with AFP, but are negative for CK7 and EMA (diffusely positive in PPCC). 34 Renal cell carcinomas show less common pleomorphism and hobnail cells and express RCC, CD10, and PAX8. 8 Peritoneal carcinomas are believed to behave similarly to ovarian carcinomas; therefore, their treatment is similar, with debulking surgery followed by chemotherapy or neoadjuvant chemotherapy and second-look surgery. These tumors are characterized by poor prognosis with a median survival of approximately 24 months and 5-year survival rate of 18%. 11 Unfortunately, a few data about outcome of PPCC are available because of its rarity. In the reported cases, the recurrence and metastatic rate were about 33% and 3 patients (25%) died of disease within 6 months (Table 1). When dealing with a primary peritoneal tumor, a diagnosis of PPCC should be kept in mind. New treatment strategies are necessary to improve local control and decrease mortality for patients with primary peritoneal clear cell carcinoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.