
Abstract
Appendiceal pneumatosis is rare, reported either in the context of acute appendicitis or enterocolitis. Here, we report the case of an elderly adult in whom the acute appendicitis was associated with pneumatosis and occurred in the context of a malformed appendix with pathogenic organism remnants. A 72-year-old man presented with abdominal pain 3 weeks after posttraumatic dorsolumbar surgery. The computed tomography scan showed acute appendicitis and 2 diverticula. On microscopy, the appendix showed acute appendicitis along with a Cave-Wallbridge type A duplication. In addition, several optically clear spaces were observed in the entire appendiceal wall consistent with pneumatosis of the appendix. Focally, calcified structures suggesting pathogenic organisms such as Schistosoma were noted as well. In conclusion, we report a case of appendiceal pneumatosis occurring in the context of acute appendicitis in a duplicated appendix, with presence of calcified structures suggestive of pathogenic organisms.
Introduction
Appendiceal pneumatosis is a rare condition, occurring either in the context of acute appendicitis or as part of enterocolitis-related pneumatosis.1-5 Here, we report the case of an elderly man in whom acute appendicitis was associated with pneumatosis, occurring in the context of appendiceal duplication associated with calcified structures suggestive of pathogenic organisms.
Case Report
A 72-year-old man presented with arterial hypotension, confusion, and urinary tract infection treated with levofloxacin for 2 weeks. Two days after this episode, the patient developed low-grade fever and abdominal pain associated with biological inflammatory response. The computed tomography (CT) scan showed 2 appendiceal diverticula and distal appendicitis with a possible tip perforation (Figure 1). The cecum was normal. The patient’s past medical and surgical history revealed sigmoid diverticulosis treated by surgery (date unknown), left humeral prosthesis (4 years prior), C6 corporectomy, and complete paraplegia after trauma in the context of spondylarthropathy (3 weeks prior) treated with T10-L2 fixation, T12 laminectomy, and anterior basicervical osteosynthesis. The patient also showed fluctuating arterial hypertension (treated with Hytacand and Esidrex) and atrial dysrhythmia. An appendectomy was performed.
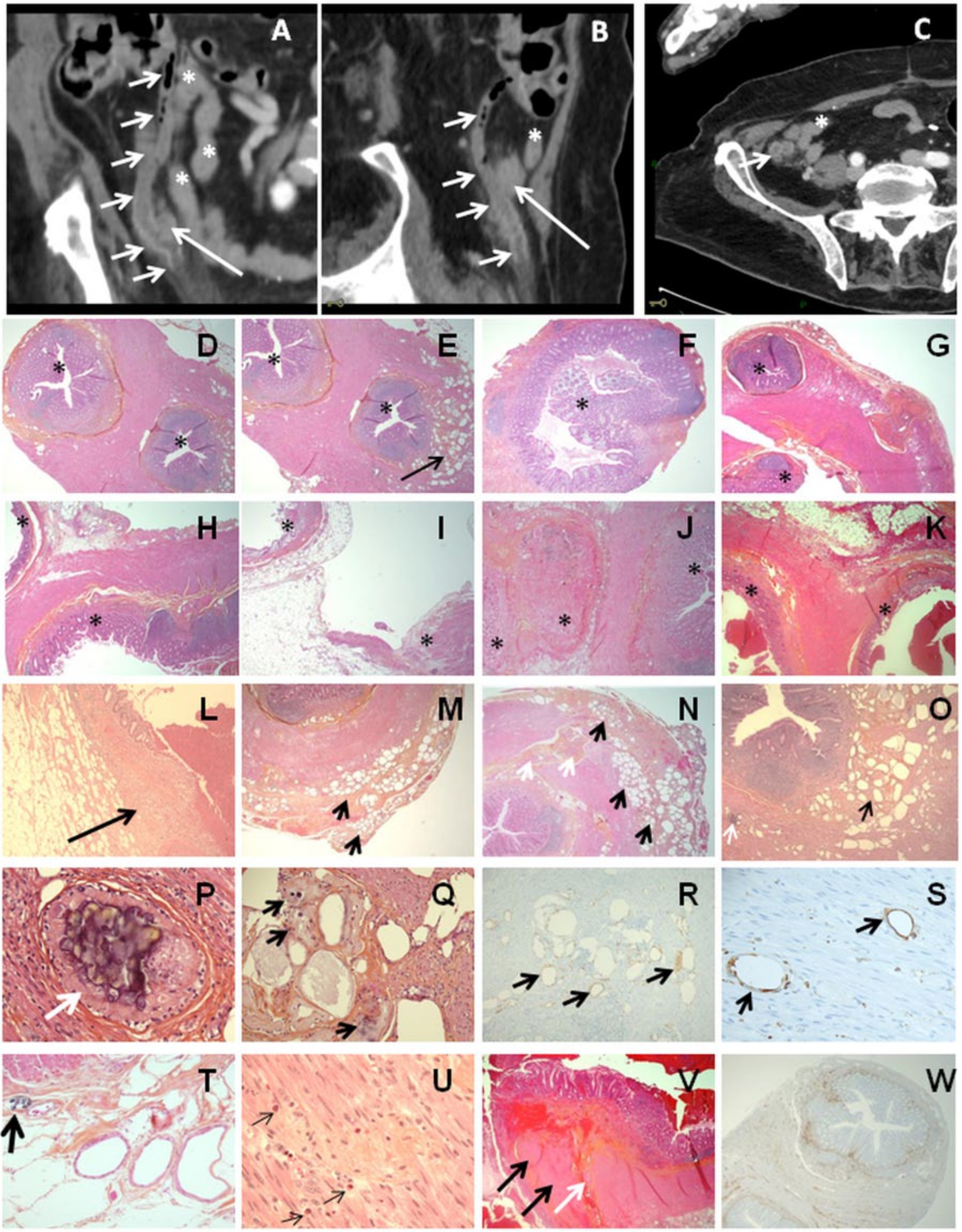
The computed tomography scan showed a tortuous appendix with 2 diverticula in the middle (A, B: white arrows for diverticula, black arrows indicate possible wall fusions, asterisks indicate the small intestine). On axial section at the middle third of the appendix, there was a suggestion of 2 diverticular cavities (C). On microscopy, the appendiceal wall showed 2 mucosae and submucosae and 2 muscle walls (D, E, G-K: asterisks for appendiceal mucosa/wall). Wall fusions were observed at the proximal resection margin (D, E: same site/section; asterisks for the appendiceal mucosa/wall; F, Gerlach fold seen on a serial section in the same tissue block with D-E) in the cecal half of the appendix (G-I; H and I are multistep sections in the same block: asterisks for the appendiceal mucosa/wall) and possibly associated with a kink/tortuosity (J: asterisks for 3 sites of appendiceal mucosae). Based on the microscopic examination, the findings indicated appendiceal duplication rather than diverticula because 2 muscle layers were seen (D, E, J, K). Areas of transmural acute appendicitis with complete wall destruction were seen in the distal half of the appendixes (K, L: asterisks for appendiceal mucosa and arrow for wall inflammation). Appendiceal pneumatosis was observed in the pericecal location (E, M, N, O: black-arrows; N: white arrows for a vascular hiatus). Calcified, round structures were seen proximal to the optically clear cavities (O, P: white arrow for the same calcified structure at different magnifications; Q, T: black arrows for pathogen calcifications). CD68-positive macrophages were seen around the intramuscular optically clear spaces of pneumatosis (R, S: black arrows). Several eosinophils were seen in the muscle wall (U: black arrows). The appendix wall also showed nodular muscular hypertrophy (V: black arrows, vascular hiatus/white arrow) and segmental mucosal neural hyperplasia, S100-protein positive (W: black-arrows).
The appendix measured 7.0 cm in length and was tortuous and nodular, measuring 0.4 cm in diameter in the middle part. The entire specimen was submitted for microscopic examination after formalin fixation. Multistep and serial hematoxylin-and-eosin sections and special stains (PAS, Congo Red) were performed. The appendix showed multiple sites of duplication, characterized by fusion of 2 appendiceal segments, either at the level of the internal and external muscle wall layers or at the subserosa level, on varied lengths (Figure 1). There was a proximal fusion at the resection surgical margin, continuous with a Gerlach fold toward the cecal lumen. In addition, there were 4 wall fusions noted in the middle third of the appendix and a separate one distally at the appendix tip. The presence of double muscle layers in these areas suggested the presence of appendiceal duplications rather than diverticula, although the presence of focal communications between the 2 lumens was noted.
In addition, a rim of fibrous tissue containing several optically clear, irregular cavities was noted at the base of the appendix, including the cecal resection margin. On one section, these lesions were continuous with a transmuscular vascular hiatus. The rim of fibrous tissue was located in the subserosa, muscularis, and very focally in the submucosa of the appendix and measured 1.5 cm in length. The optically clear, irregular cavities measured up to 0.1 cm in diameter and were surrounded by CD68-positive multinucleated giant cells at the periphery. These findings were consistent with pneumatosis of the appendix.
Furthermore, the intramuscular fibrous reaction was focally micronodular with calcified material suggestive of Schistosoma remnants. Inflammatory cells, including eosinophils, were seen in the vicinity. Several minute foci of multinucleated giant cells or macrophages were noted in the mesoappendix, at a distance from the aforementioned appendiceal lesions.
The distal half of the appendix, including the areas of duplication, showed transmural acute inflammation with peritonitis and preperforation. The submucosa and mucosa at the base of the appendix showed, over a length of 0.25 cm, focal neural and Meissner plexus hyperplasia (confirmed by S100-protein positivity). There were no cytokeratin-positive cells in the appendiceal submucosa, muscularis, and subserosal layers. Focally, hypertrophy of the muscularis propria protruding within the appendiceal lumen in a polypoid fashion was noted. These areas measured 0.1 to 0.4 cm in length and alternated with areas of muscle atrophy.
At 8 months postoperatively, the patient was doing well. Serology test showed anti-Schistosoma mansoni antibodies at 0.4 (significant level >1.2).
Discussion
Here, we report a peculiar case of appendiceal pneumatosis associated with acute appendicitis and occurring in a dysmorphic appendix. In general, appendiceal pneumatosis is observed either associated with intestinal, enterocolitis-related pneumatosis or in the context of perforated appendicitis.1,3,4 However, in our case, the origin of pneumatosis is difficult to establish. Both prior trauma- or diverticulosis-related surgical procedures and repetitive episodes of perforating appendicitis could possibly be involved.
The histological analysis allowed us not only to diagnose the appendiceal pneumatosis, but also to precisely characterize the nature of the lesions identified on the CT scan. First, we observed a subserosal and perimuscular fibrous reaction around several optically clear spaces lined by multinucleated giant cells, which dissected the appendiceal muscle layer into the submucosa. An adenocarcinoma was not considered, based on microscopic examination and lack of cytokeratin-positive epithelial cells around these cavities. A foreign-body reaction to surgical material used for bone consolidation was ruled out because of the absence of birefringent foreign material and based on the site of prior orthopedic surgery.
Second, we noted the presence of nodular fibrosis with calcifications associated with the presence of eosinophils in the adjacent tissue and foci of multinucleated giant cells and macrophages in the mesoappendix. These findings were most suggestive of Schistosoma (Pr S. Ahmed and Pr M. Botonne, personal communications, 29 August 2014 and 24 October 2014). In addition, the serological studies identified the presence of Schistosoma mansoni antibodies, although not at a significant level.
Third, the microscopic analysis of the resected specimen allowed us to correctly identify the malformative lesions in the appendix, identified as diverticula on the preoperative CT scan and appearing as a nodular, tortuous appendix on gross examination. 6 Although the imaging procedures might have suggested a triplication at the site of the 2 diverticula, the microscopic analysis could not completely eliminate a kink (without the congenital fibrous band at this site) or tortuosity. However, microscopy was suggestive of a complex type of dysmorphic appendix with partial duplications of appendiceal walls. Two other cases with similar appendiceal lesions were identified in the literature. One case from 1904 reports on a newborn male, in which the appendix was extensively studied on more than 570 serial sections. 7 The second case from 1931 reports on a 7-week-old baby girl. 8 In both reports, the dysmorphic appendices were associated with umbilical hernia and fistula. Cave, in his 1936 review, 9 included these malformations, overlapping with the condition known as congenital diverticulosis, 10 in the type A malformations of appendix duplex type, which later remained type A in the Cave-Wallbridge classification. 11
In our case, other muscle wall lesions were also observed, such as multiple polypoid, nodular areas of muscle hypertrophy alternating with muscle atrophy, and segmental mucosal neural and Meissner plexus hyperplasia.
The pathogenesis of all these lesions observed in the appendix of a 74-year-old patient remains difficult to establish. In general, appendiceal duplications are compatible with a normal existence, unless associated with other more serious abnormalities. 12 We can hypothesize that the duplication zones, the muscle layer irregularities, and the neuronal hyperplasia could have favored fecal stagnation, backgounding to perforated appendicitis with pneumatosis.
In conclusion, appendiceal pneumatosis may occur in elderly patients, as revealed by acute appendicitis. The extensive microscopic examination of the appendix is important not only for the diagnosis of such a lesion, which may remain undetected on imaging studies, but also for a precise diagnosis of other lesions such as appendiceal malformations or presence of pathogenic organisms.
Footnotes
Acknowledgements
The authors thank Dr L. Larnaudie, Dr G. Nasr, Dr C. Berber, Dr Goussef, Dr F. Mecheri, Dr B. A. Gaffar, Pr S. Ahmed, and Pr M. Bottone. We also thank the NCA/Avicenne, BIUM and CDMP/APHP teams and N. Akdim, C. Almeida, V. Ipotesi, F. Bouchard, N. Delva, V. Guzal, L. Jovanov, I. Pluchart, F. Spindler, C. Van Vetteren, S. El Sayeh, L. Delagarde, J. Raleche, B. Mechekour, and L. Lefebure.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.