
Abstract
Sinonasal adenocarcinoma is a rare tumor of the head and neck accounting for 10% to 20% of all primary malignancies of the nose and paranasal sinuses. There tumors are classified as salivary, intestinal and nonintestinal, nonsalivary. Low-grade nonintestinal nonsalivary are rare tumors whose diagnosis is essentially that of exclusion. Here we present the first case of one such tumor associated with an exophyic Schneiderian papilloma. A 71-year-old retired aerospace engineer presented with a 1-year history of severe nasal obstruction. Endoscopy and compted tomography imaging demonstrated a polypoid lesion occupying his entire right nasal cavity extending into and filling the nasopharynx. Biopsy suggested adenocarcinoma, at least in situ and the patient subsequently underwent complete resection. Pathologic evaluation demonstrated polypoid tumor consistent with a low-grade papillary adenocarcinoma with micropapillary architecture associated with a small amount of residual exophytic Schneiderian papilloma. Immunohistochemistry revealed diffuse expression of CK7, CK 5/6, and S100 protein in tumor cells. Expression of p63 was seen in basal cells only. Tumor cells did not show expression of CK20, CDX2 (intestinal markers), mammaglobin, GATA3 (salivary markers), PAX8, WT1, nor estrogen, progesterone, or androgen receptors confirming its nonintestinal nonsalivary differentiation.
Introduction
Sinonasal adenocarcinoma (SNAC) is a rare tumor of the head and neck accounting for less than 1% of all head and neck malignancies and 10% to 20% of primary malignant neoplasms of the nose or paranasal sinuses. 1 These tumors represent a wide array of pathologies that, historically, resulted in variable reporting and diagnosis. In 2005, the World Health Organization classified SNACs into 2 broad categories: salivary- and nonsalivary-type SNACs. 2 Salivary-type SNACs are further subdivided into low and high grades. High-grade lesions, with the exception of adenoid cystic carcinoma, are rare and the low-grade lesions, including mucoepidermoid carcinoma, polymorphous low-grade adenocarcinoma, and acinic cell carcinoma, rarely form in this region. 3 Nonsalivary types are divided into intestinal and nonintestinal types. The intestinal type is the most common SNAC and represents 6% to 13% of all primary neoplasms in this region. They arise from intestinal metaplasia of the ciliated respiratory epithelium lining the Schneiderian membrane. These classically occur in the ethmoid sinuses of older men with occupational exposure to wood dust, leather, nickel, chrome, and a number of other agents.1,3 The nonintestinal, nonsalivary type lesions are a relatively new diagnostic entity. They are presumed to arise from seromucinous glands, but lack intestinal features. Histologically, they have heterogeneous morphology that precludes a precise definition and, because of this, are a diagnosis of exclusion. 4 Here we report the first case, to our knowledge, of a low-grade nonsalivary, nonintestinal type SNAC associated with an exophytic Schneiderian papilloma.
Case Report
A 71-year-old male retired aerospace engineer presented with a 1-year history of nasal obstruction. The patient complained of bilateral nasal congestion, dry mouth, anosmia, and was noted to have a hyponasal voice. He denied any visual changes or history of chronic sinus disease. His medical and surgical histories were noncontributory. Nasal endoscopy revealed a polypoid lesion along the floor of the nose arising under the right middle turbinate and obstructing the choana. The left nasal cavity was clear of any mass anteriorly, but the right sided lesion could be seen in the nasopharynx obstructing the left choana. A high-resolution computed tomographic image of sinus was obtained and showed partial opacification of most of the right paranasal sinuses with the right maxillary completely opacified. A soft tissue mass completely filled the right nasal cavity and the nasopharynx. There was no bony obstruction or expansile changes in the pterygopalantine fossa (Figure 1A and B).
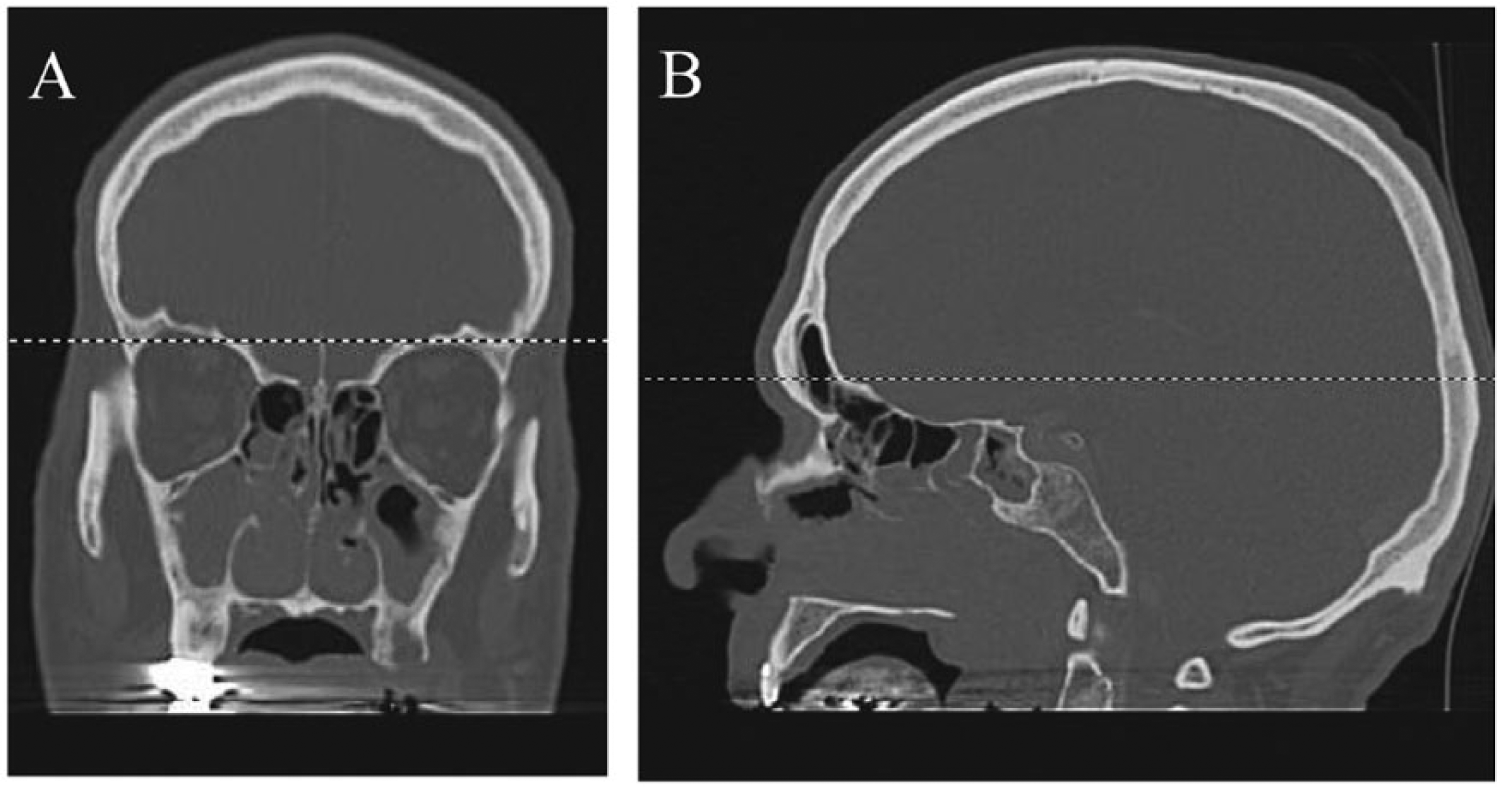
Coronal and sagittal computed tomography images in a bone window (A and B, respectively) demonstrating complete obstruction of the right nasal passageway, opacification of the right maxillary sinus and extension into the nasopharynx.
The initial biopsy was concerning for adenocarcinoma at least in situ and the patient subsequently underwent complete endoscopic resection of the mass. Intraoperatively, the mass was found to be distinct from the middle turbinate and attached to the medial maxillary sinus wall. A clearly delineated stalk was identified at this attachment and was resected along with the surrounding area. The mass was pushed into the nasopharynx and delivered through the mouth due to its size. A total ethmoidectomy, wide maxillary antrostomy, and frontal recess exploration were then performed to ensure complete resection. Multiple biopsies were taken from several areas throughout the sinuses and sent for frozen section. All were negative for carcinoma.
Grossly, the bulk of the mass was 7 × 4.8 × 3.2 cm and 21 g. The mass’ outer surface ranged from smooth tan/pink and gelatinous to pink/white with 70% papilliferous. Sectioning revealed a gelatinous tan cut surface partially surrounded by pink/white papilliferous tissue. Specifically, the specimen was a polypoid tumor grossly and microscopically covered with a low-grade papillary adenocarcinoma with micropapillary architecture. The large papillae showed a fibrovascular core with numerous broad branching papillae (hierarchical branching) that progressively become smaller. Tufts of free-floating tumor cells were also present on the surface. The tumor cells showed mild nuclear atypia and no mitosis. Focal mucin production was seen (mucicarmine positive). And, although the tumor was predominately on the surface, multiple lobules of tumor were seen within the stroma. The tumor was also associated with a small amount of residual papilloma that appeared to be exophytic schneiderian papilloma with squamous metaplasia. Immunohistochemistry revealed diffuse expression of CK7, CK5/6, and S100 protein in tumor cells. Expression of p63 was seen in basal cells only. Tumors cells did not show expression of CK20, CDX2, mammaglobin, GATA3, PAX8, WT1, and estrogen, progesterone, and androgen receptors. The final pathology was a low-grade micropapillary adenocarcinoma, nonintestinal, nonsalivary type, associated with exophytic Schneiderian papilloma (Figures 2 and 3).
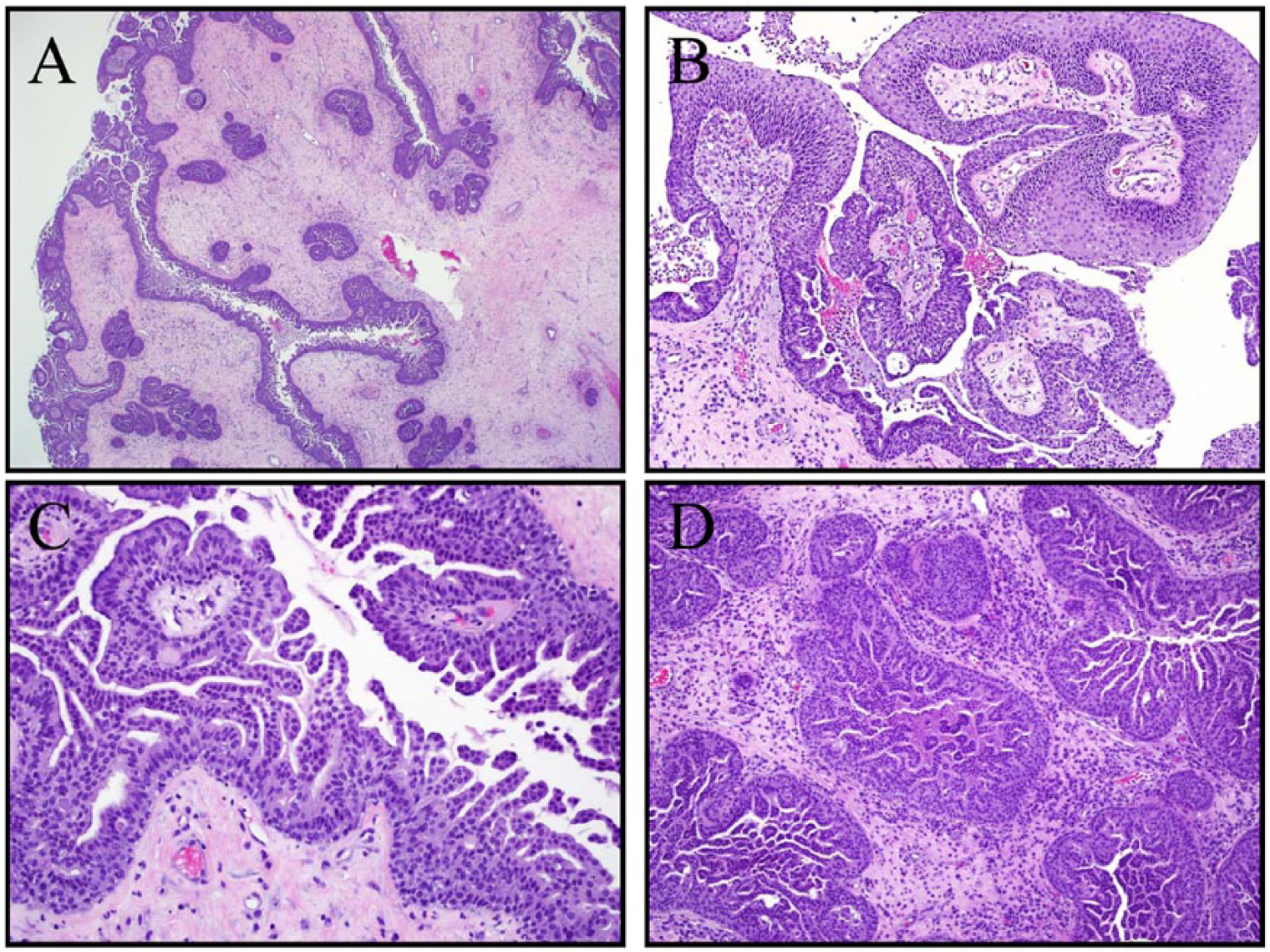
(A) Low-power (hematoxylin and eosin [H&E], 2×) view of tumor showing a tumor surface covered with micropapillae that extend into the crypts and gland. (B) Area of exophytic Schneiderian papilloma with squamous metaplasia (H&E, 10×). (C) Higher magnification of tumor showing broad papillae intermixed with delicate micropapillae without fibrovascular cores and apparently free-floating epithelial tufts (H&E, 20×). (D) Stromal invasion with desmoplasia and chronic inflammation. Comedo-type necrosis and micropapillae with epithelial tufting is seen within invasive tumor lobules (H&E 20×).
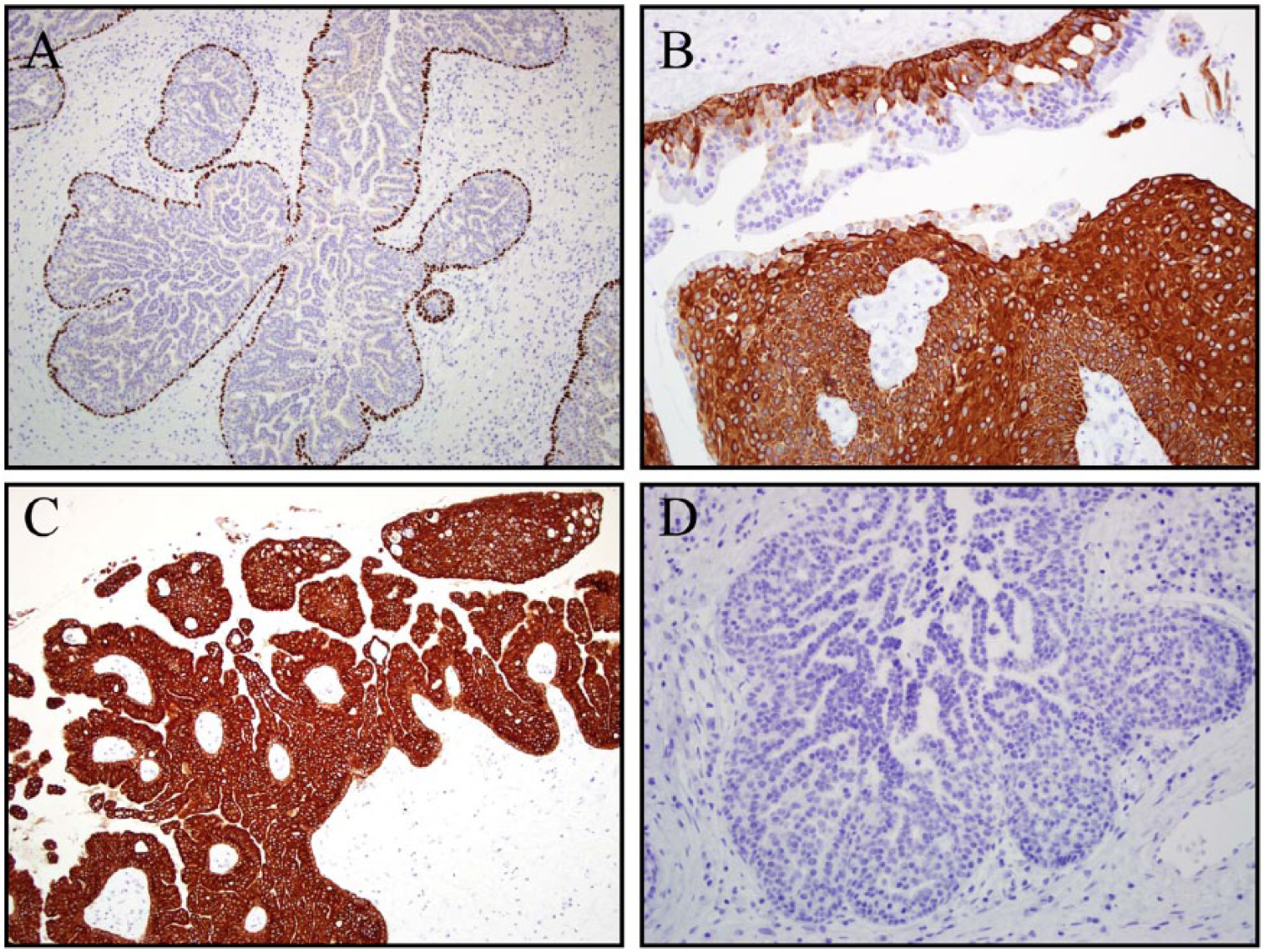
(A) Immunohistochemistry shows that the basal cells are positive for p63 (10×). (B) CK5/6 shows a basal expression in the adenocarcinoma and a more diffuse expression in the Schneiderian papilloma with squamous metaplasia (20×). Tumor is diffusely positive for CK7 (C, 10×) but completely negative for CK20 (D, 20×).
The patient tolerated the procedure well and had an uneventful postoperative course. Follow-up endoscopic examinations did not reveal any evidence of recurrence. His case was discussed at our multidisciplinary tumor board and, because of the tumor’s low-grade features, no adjuvant therapy was recommended.
Discussion
The World Health Organization broadly defined SNACs into 2 groups, salivary and nonsalivary. The salivary-type carcinomas are further subdivided into high and low grades. The nonsalivary-type carcinomas are also subdivided into intenstinal and nonintestinal. Histologically, the low-grade nonsalivary, nonintestinal type SNACc are a difficult entity to classify and are essentially a diagnosis of exclusion. Our case represents one such diagnostic challenge and is the first reported case of a low-grade nonsalivary nonintestinal type SNAC associated with an exophytic Schneiderian papilloma.
The majority of sinonasal tract lesions are benign and consist mainly of inflammatory polyps and Schneiderian papillomas. However, low-grade lesions do arise with histological features that make it difficult to define whether they are truly benign or malignant, especially when the biopsy shows a low-grade glandular proliferation. In these cases, the differential diagnosis includes reactive proliferations, hamartomas, for example, respiratory epithelial adenomatoid hamartoma (REAH), seromucinous hamartoma, and low-grade SNAC. 5
As mentioned, deciphering malignancy in low-grade sinonasal tumors is difficult, but, in this case, despite the low nuclear grade and the absence of mitoses, several features pointed to its malignant nature. Specifically, the tumor demonstrated necrosis, stromal invasion with desmoplasia and chronic inflammatory reaction. 5 The complex glandular architecture, epithelial tufting, and micropapillae were reminiscent of borderline serous tumors of the ovary; however, the tumor cells were negative for PAX8 and WT1 (generally positive in serous carcinoma of Mullerian origin), and the patient was a man. Once identified as an adenocarcinoma, the tumor needed classification in accordance with the World Health Organization system. This tumor did not express GATA3, mammaglobin, and the steroid receptors (estrogen, progesterone, and androgen), as most salivary adenocarcinomas do, and it did not express intestinal markers, CK20 and CDX2. Thus, this low-grade SNAC did not demonstrate salivary or intestinal differentiation.3,6
Low-grade SNACs are frequently incidental findings identified in resected specimens of patients presenting with nasal obstruction, and clinically thought to have inflammatory polyps or chronic sinusitis. There are no known occupational or environmental factors associated with these tumors and there is no definitive precursors identified. However, Jo et al, 5 in 2009, presented a series of 6 low-grade SNACs associated with REAHs and suggested a potential link. However, the tumors in their series were described as tubular in nature instead of the micropapillary architecture of our case. Additionally, REAH shows a p63 and 34bE12 positive basal layer and diffuse positivity for CK7, and should be negative for CK20, CDX2, and S100, 5 whereas our tumor was S100 positive.
Malignant transformation of exophytic Schneiderian papilloma is exceedingly rare with only 3 cases reported in the literature as opposed to inverted or oncoytic papillomas that have a nearly 10% risk of malignant transformation. 7 In 1962, Norris, 8 in a report of 28 cases of nasal papillary lesions, noted 1 patient who had an exophytic Schneiderian papilloma of the septum, floor of the nose and inferior turbinate that contained squamous cell carcinoma (SCC) adjacent to an area of papillary metaplasia. Buchwald et al 9 described another case of SCC arising within an exophytic Schneiderian papilloma of the nasal septum and vestibule. This case presented 16 years after a resection and was HPV6 and HPV11 positive. Last, Terada 7 reported the most recent case of a malignancy in an exophytic Schneiderian papilloma. He demonstrated a tumor with a largely noninvasive, nonkeratinizing SCC component with gradual merges between the SCC and the Schneiderian epithelium. 7
Unlike intestinal-type or high-grade SNACs, the low-grade lesions portend a much better survival. Complete resection is the treatment modality of choice and, with negative margins, these tumors are unlikely to recur and have a low risk of metastasis. There is no race or sex predilection, tend to occur in people older than 50 years and can arise from anywhere in the sinonasal tract with the nasal cavity being more common than the ethmoid or maxillary sinuses. 3
Here we report the first case of a low-grade, nonintestinal, nonsalivary SNAC associated with an exophytic Schneiderian papilloma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.