
Abstract
Well-differentiated papillary mesothelioma (WDPM) affecting the tunica vaginalis testis is a rare tumor, and very little is known about the clinicopathological spectrum of this variant as a distinct entity. Most patients with WDPM suffer from scrotal pain or swelling, but hydrocele seems to be the most common presenting symptom. These lesions are usually not aggressive and are accompanied by an indolent clinical behavior. In this article, we report the first case known of WDPM in an undescended testis, and in addition, we review the literature for similar cases.
Keywords
Introduction
Well-differentiated papillary mesothelioma (WDPM) of tunica vaginalis is an uncommon mesothelial tumor. The majority of WDPM originate in the abdominal or pelvic peritoneum of young women. Occasionally, the tumor may involve the pleura, paratesticular area, or pericardium. WDPM of the scrotal sac was first described in the literature by Barbera and Rubino 1 ; only 17 cases have been reported so far. Compared with most other forms of mesothelioma, WDPM appears usually not aggressive and accompanied by an indolent clinical behavior. 2 Over the past years, the term benign mesothelioma has also been used to describe tumors with similar features. However, much controversy still exists as to whether WDPMs constitute a distinct entity. Common histological characteristics of WDPM include well-formed papillary structures lined by a single layer of cuboidal mesothelial cells with mild or absent atypia. 3 To our knowledge, we describe in this article the first case of WDPM arising in tunica vaginalis in an undescended testis. In addition, we have also performed a review of the literature for similar cases.
Case Report
In April 2013, a 26-year-old male was admitted to “Mater Salutis” Hospital (Legnago, Italy) for an unexpected solid-cystic mass detected, in an undescended intraabdominal testis, during a routine ultrasound examination (Figure 1A). Biochemical and hematological parameters were within normal ranges. The patient’s anamnestic history revealed no previous illness, trauma, or exposure to asbestos or ionizing radiation. The patient was submitted to surgery and the undescended testis with the cystic lesion were removed. On macroscopy, a paratesticular cyst of 48 mm in diameter was associated to a testis sized 5 × 2.5 × 1.5 cm. The patient’s postoperative course was uneventful. No medical therapy was performed after the surgery, and the patient is well and free from disease with a follow-up of 29 months.
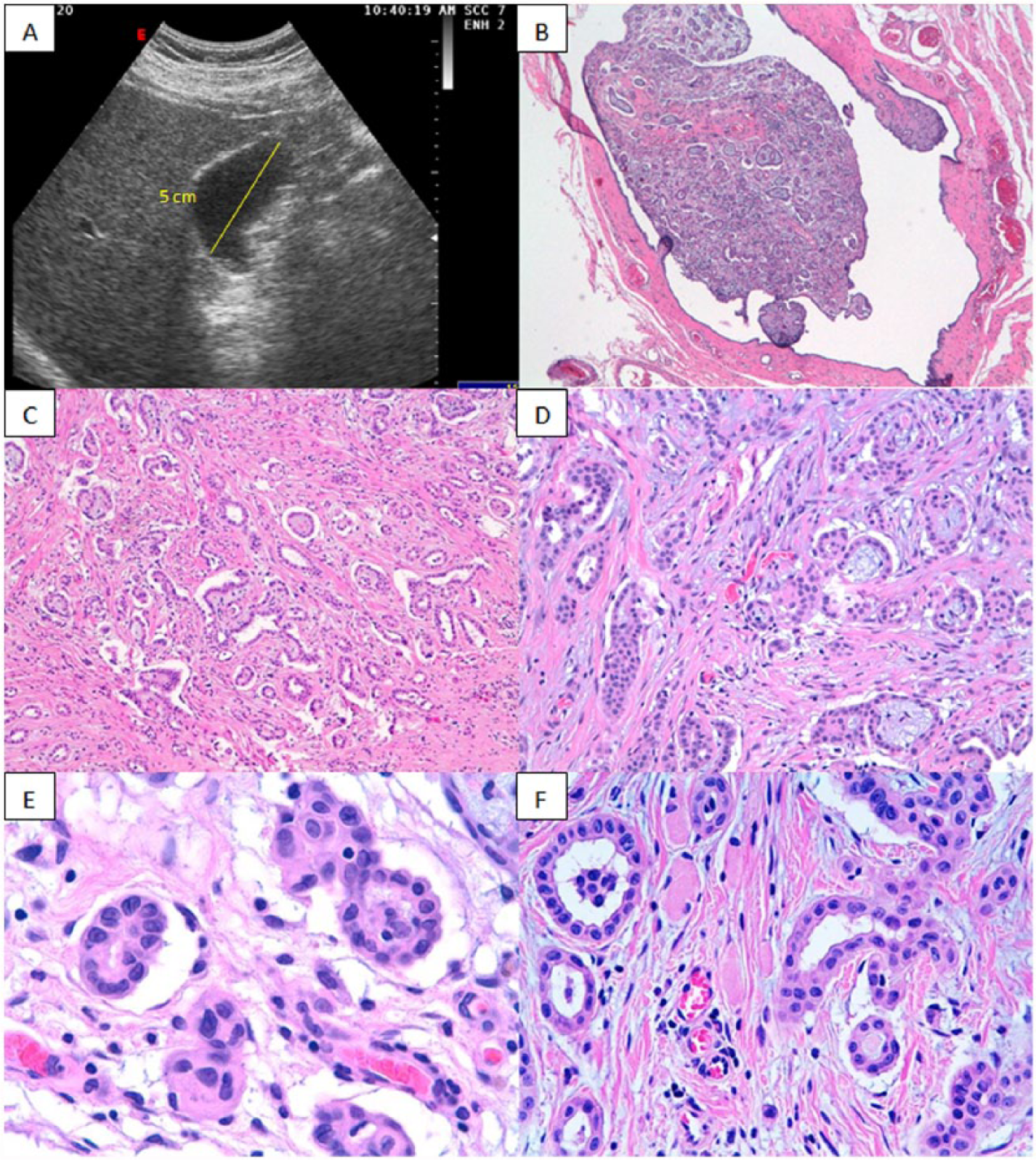
Ultrasound image reveals intraabdominal undescended testis (yellow line) without evident mesothelial lesion (A). Histologic examination shows intracystic proliferation (hematoxylin-eosin [H&E]; 100×; B) with a tubulopapillary growth pattern: H&E, 100× (C); H&E, 200× (D). The neoplasm consists of cuboidal cells with mild or absent atypia (H&E; 400×; E, F).
Pathological Findings
Three-micrometer-thick sections were cut from formalin-fixed paraffin-embedded tissues and routinely stained with hematoxylin and eosin (H&E). Histological examination showed a cystic lesion in the paratesticular tissue composed of cuboidal cells lining, in a single layer, the wall of the cyst. In focal area, the cystic wall was thickened by papillary structures and a pseudo-solid proliferation consistent with a tubulopapillary growth pattern (Figure 1B-D). The majority of neoplastic cells showed mild or absent atypia, nuclear pseudoinclusion, and rare nucleoli, but neither mitoses nor necrosis was observed (Figure 1E and F). Tumor cells were positive for markers such as CA125, calretinin, CK7, CK 5/6, and WT-1 (Figure 2A-D) but negative for CEA, CD10, CDX-2, CK20, and TTF1.
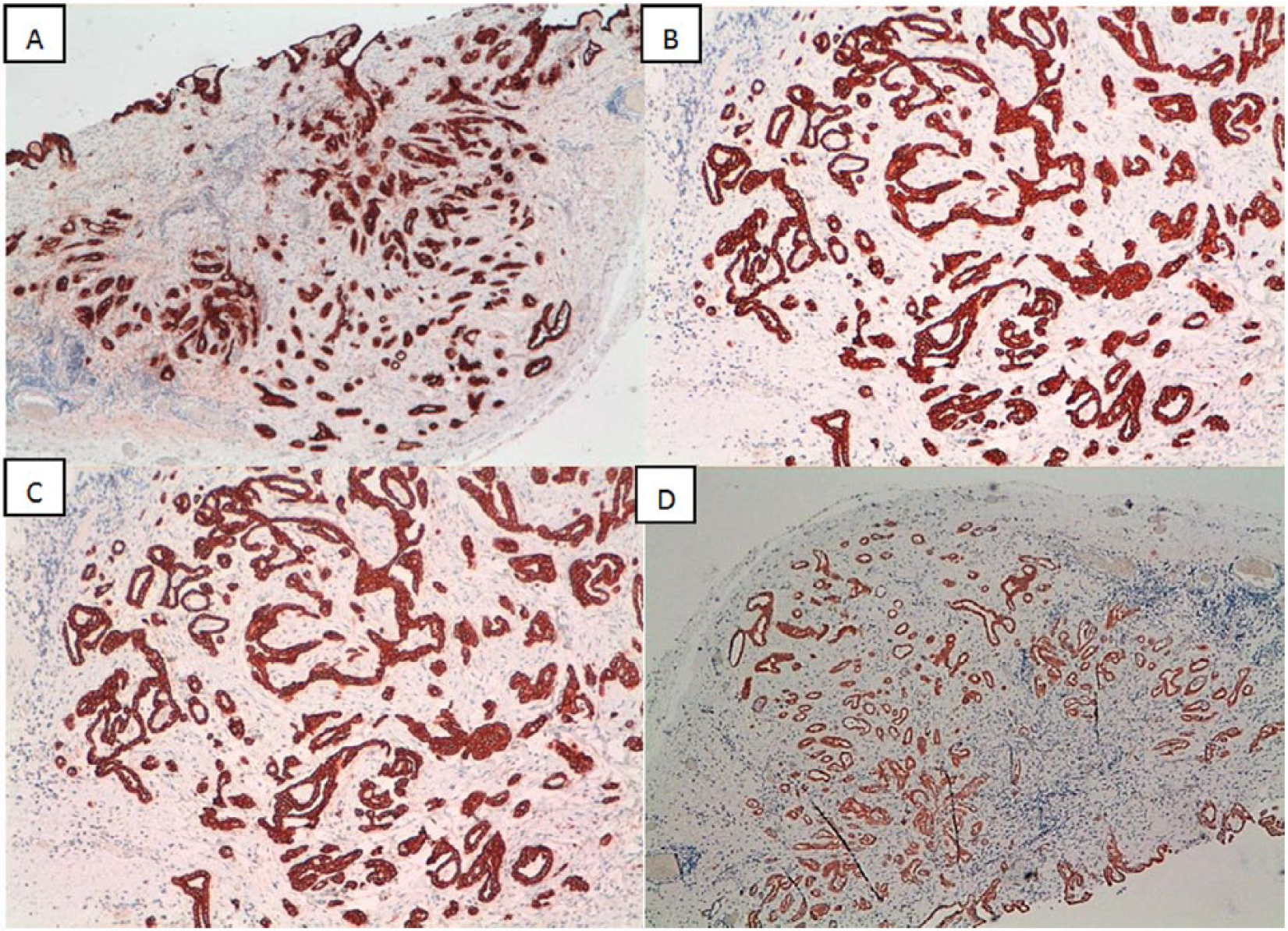
The immunohistochemistry shows strong and widespread expression of mesothelial markers in neoplastic cells: (A) Calretinin (100×), (B) CK7 (200×), (C) CK5/6 (200×), and (D) WT1 (100×).
Discussion
WDPM is an uncommon mesothelial neoplasm mainly affecting the pelvic peritoneum of women in the third and fourth decades. Tumors with similar characteristics can arise from multiple anatomic sites, among which is the paratesticular area. However, only 0.3% to 5% of cases of mesothelioma affect the tunica vaginalis. WDPM may affect the spermatic cord, epididymis, and the peritoneal mesothelium of inguino-scrotal hernia sacs. 4
To the best of our knowledge, only 17 cases of WDPM of the tunica vaginalis have been published to date in the literature. Clinical pathological data of the current case and of the series reported in the literature are summarized in Table 1.1-3,5-14 Patients’ age ranged from 18 to 70 years (mean = 43 years). Most patients with WDPM suffer from scrotal pain or swelling, but hydrocele is the most common presenting symptom as being reported in 82% of the cases. WDPM typically presents either as solitary, or less often, with a limited number of superficial small nodules on the surface of an hydrocele sac, ranging from a few millimeters to 3 cm size (as observed in the current case). 15 The prognosis of WDPM is generally considered good, but quite variable in the literature. Very little is known about this variant, making its classification as a distinct nosological entity still uncertain. 4 This suggests that the long-term behavior of the paratesticular WDPM remains uncertain. Typically, WDPM is composed exclusively of well-formed fibrovascular papillae, lined by a single row of cuboidal mesothelial cells with bland cytology and absent mitotic activity (≤1 × 10 HPF) without stromal infiltration or invasion of the adjacent tissues/organs. However, some WDPMs may show more complex pathologic features, such as areas of tubulopapillary differentiation and focal regions of solid sheets of cells.
Cases of Well-Differentiated Papillary Mesothelioma of Tunica Vaginalis Reported in the Literature.
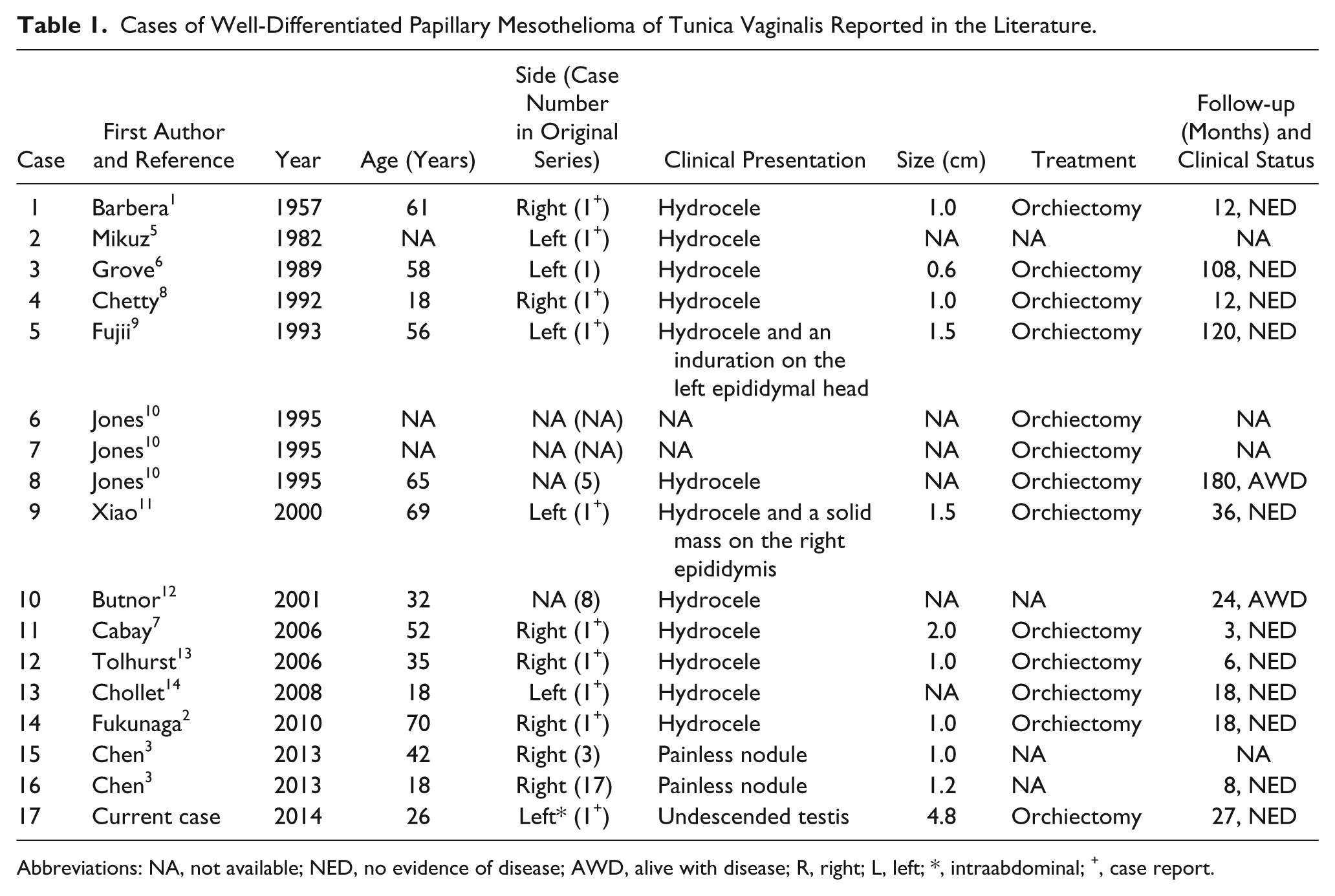
Abbreviations: NA, not available; NED, no evidence of disease; AWD, alive with disease; R, right; L, left; *, intraabdominal; +, case report.
In keeping with this, recently, the term “mesothelioma of tunica vaginalis of uncertain malignant potential” (MUMP) has been proposed to describe lesions with more complex tubulopapillary growth pattern. 16 Compared to WDPM, MUMP can be composed of a complex architectural morphology (including cribriform and condensed patterns), scattered mitotic figures, mild cell atypia, microfocal coagulative necrosis in the absence of signs of overt malignant transformation such as stromal invasion and atypical mitotic figures. 16 In these cases, hydrocele is the most common presenting symptom. A scrotal mass is only rarely present. However, such a morphological criterion does not necessarily imply a different clinical behavior. In clinical practice, except for surgical excision, there are no specific treatment recommendations for WDPM and MUMP. Thus, it is important that these uncommon tumors have to be well documented with a long-term follow-up. Some authors have also suggested that MUMP represents a morphological continuum between classic WDPM and diffuse malignant mesothelioma. To our knowledge, a total of 9 cases of MUMP have been reported in the literature and are summarized in Table 2.15,16
Cases of Mesothelioma of Tunica Vaginalis of Uncertain Malignant Potential Reported in the Literature.
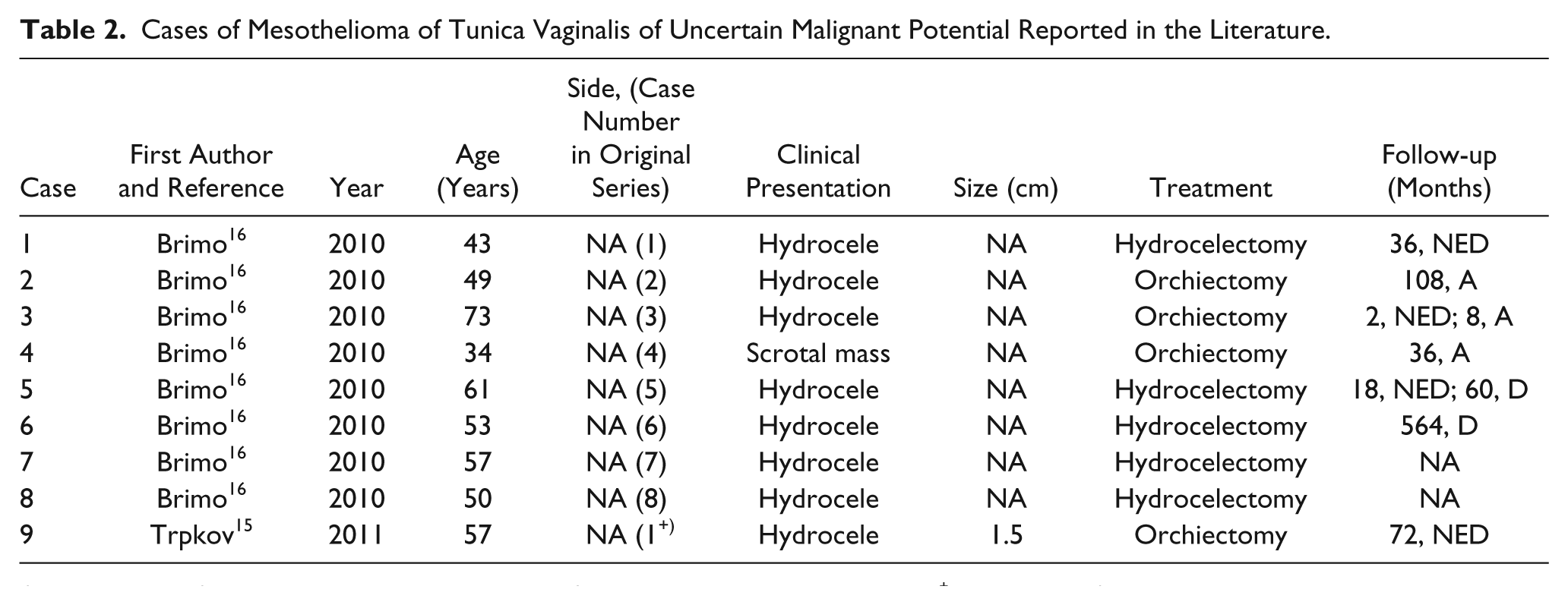
Abbreviations: NA, not available; NED, no evidence of disease; D, dead unknown causes; +, case report; A, alive.
The main WDPM differential diagnosis includes MM, which occurs most commonly in older men. Generally, patients with MM present local recurrence up to 60% of cases in the first 2 years from the initial treatment. Typically, MM can have focal areas composed of well-differentiated papillary structures “WDPM-like,” but they are often accompanied by infiltrative features, cells nuclear atypia, mitotic activity, and coagulative necrosis. Paratestis tubulopapillary neoplasms such as rete testis/epididymal carcinoma, serous carcinoma, and metastatic adenocarcinoma are also included in the differential diagnosis.
Rete testis carcinoma mainly occurs in elderly males with scrotal pain, swelling, or occasionally hydrocele. The diagnostic criteria for this variant include, according to Amin, 17 the absence of histologically similar extrascrotal tumor, tumor centered on the hilum, the morphology incompatible with any other type of testicular or paratesticular tumor, and the immunohistochemical results consistent with the immunopositivity for Wolffian-derived structures-associated markers, that is, CD10 and calretinin.
In patients with serous carcinoma, diagnostic signs and symptoms include dull pain, swelling, palpable mass, hydrocele, and elevated levels of CA125. The mean age for patients affected by borderline and invasive serous carcinomas was, respectively, 56 and 31 years. Borderline tumors are often encapsulated and cystic and contiguous with the tunica vaginalis, whereas carcinomas are usually noncystic and infiltrative. Finally, Mullerian papillary serous neoplasm-associated markers (WT-1, CA125) could be useful in the diagnosis of this variant. Metastasis to the paratestis occurs in patients older than 50 years, who present an anamnestic history of other primary carcinoma (mainly stomach and prostate). They are histologically multifocal with frequent vascular invasion and interstitial growth pattern. Specific markers are useful in the differential diagnosis to classify the metastasis of unknown origin. 17
Epidemiological studies indicate that cancer risk is 35 to 48 times higher in patients with an undescended testis compared to the overall population, and the risk for malignancy is about 6-fold higher in patients with abdominal testes. The incidence of testis tumors is higher in patient aged between 20 and 40 years, and the most common cancer types are seminoma and embryonal carcinoma. 18 To our knowledge, only one case of MM in an undescended (intraabdominal) testis associated with abdominoscrotal hydrocele has been reported in the literature. The risk for malignancy described above highlights the importance of performing surgical excision in patients with undescended testis. 19
We here report the first case known of WDPM arising in tunica vaginalis of an undescended intraabdominal testis. The neoplasm exhibited mostly a tubulopapillary architecture with neither mitoses nor stromal invasion. No residual or local disease progression was documented on follow-up of 29 months after surgery. Although appropriate treatment for WDPM appears to be the complete surgical excision, only a long-term follow-up will help fully understand the biologic behavior of this rare variant.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.