
Abstract
Hyperplastic polyps of the stomach are routinely encountered during upper endoscopy and often arise in the setting of abnormal surrounding mucosa, particularly Helicobacter pylori, autoimmune gastritis, and reactive gastropathy. Not infrequently gastroenterologists fail to biopsy the surrounding mucosa, thus determining the underlying etiology of the gastric hyperplastic polyp can be difficult. Recently, the Rodger C. Haggitt Gastrointestinal Pathology Society published guidelines on the use of special stains. The society guidelines indicate that H pylori are not usually present in hyperplastic polyps and special stains in this setting may have limited utility. We analyzed the histologic features of 32 gastric hyperplastic polyps in which the nonpolypoid mucosa demonstrated H pylori gastritis. A consecutive series of 50 hyperplastic polyps in which no surrounding mucosa was sampled was also analyzed. When H pylori are identified in biopsies of the nonpolypoid mucosa, it is also commonly present within the polyp tissue (22/32, 69%). The majority of H pylori organisms were identified on routine hematoxylin and eosin stain (16/22, 72%). In contrast, H pylori were only seen in 2/50 consecutive hyperplastic polyps in which the surrounding mucosa was not sampled. Compared with the hyperplastic polyps that lack the organisms, H pylori associated hyperplastic polyps more commonly had dense lymphoplasmacytic inflammation (P = .0001) and neutrophils within gastric epithelium (P = .036). Polyp location, number, size, and presence of intestinal metaplasia was not associated with H pylori. These results provide empirical data to guide evaluation of hyperplastic polyps for H pylori.
Keywords
Introduction
Gastric hyperplastic polyps are relatively common polyps encountered during endoscopy.1-3 They usually occur as single polyps predominantly located in the antrum, but may be multiple and found throughout the stomach. Histologically, hyperplastic polyps are characterized by dilated, elongated, and tortuous foveolae. The foveolar epithelial cells often show fairly prominent regenerative epithelial changes due to the inflammatory cells that are often present.4-6 The inflammatory infiltrate often consists of a mixture of lymphocytes, plasma cells, and neutrophils. The lamina propria is edematous, and in areas of ulceration, there may be marked stromal atypia. Up to 15% of hyperplastic polyps may have small foci of intestinal metaplasia, and dysplasia has been reported in 2% to 19% of cases.4,5,7,8 Adenocarcinoma arising in hyperplastic polyps is less common ranging from 0.6% to 2.1%; however, hyperplastic polyps do confer an increased risk of neoplasia in the surrounding mucosa.8-10 Patients with hyperplastic polyps of the stomach usually complain of dyspepsia, heartburn, abdominal pain, or may present with anemia due to upper gastrointestinal bleeding.5,6,11-13
Importantly, hyperplastic polyps are often associated with an abnormal surrounding gastric mucosa. There is a strong association with various types of gastritis, particularly autoimmune and Helicobacter pylori gastritis.14-17 Thus, when endoscopists are expecting a hyperplastic-type polyp, extensive sampling of the background mucosa is helpful to determine the underlying etiology 11 ; however, isolated biopsies of gastric hyperplastic polyps without sampling of the adjacent mucosa are quite common. 15 In this setting, determining the underlying etiology that gave rise to the hyperplastic polyp may be quite difficult. This may be important, as hyperplastic polyps associated with H pylori gastritis may regress on eradication of the organism.18-21
Recently, the Roger C. Haggitt Gastrointestinal Pathology Society published guidelines on when to use special stains to help identify H pylori. 22 In the discussion of gastric hyperplastic polyps, the authors suggest that, although hyperplastic polyps in the stomach are commonly associated with H pylori, organisms are not usually present in the actual polyp tissue. They suggest that ancillary studies for H pylori may be useful when applied to chronically inflamed hyperplastic polyps, but are otherwise unhelpful.
Given the uncertainty regarding the detection of H pylori within gastric hyperplastic polyps, we undertook a study to determine how often hyperplastic polyps arising in the setting of H pylori contain the organism. Furthermore, we determined the prevalence of H pylori in 50 consecutive gastric hyperplastic polyps where the surrounding mucosa was not sampled. To this end, we determined the utility of performing H pylori stains on hyperplastic polyps and to identify the histologic features within hyperplastic polyps that can guide the use of special stains.
Methods
Case Selection Criteria
Gastric hyperplastic polyp(s) where the nonpolypoid gastric mucosa was also biopsied and showed evidence of H pylori infection (n = 32) were identified. In addition, 50 consecutive cases were also selected in which the only biopsy from the stomach consisted of a gastric hyperplastic polyp.
Demographic and Clinical Variables
Patients medical charts were reviewed and data were collected on demographic and endoscopic variables, including indication for endoscopy, patient’s age, gender, and polyp location, size and polyp number.
Pathology Review
Histology slides were retrieved, and the diagnosis was confirmed. Histological variables, such as presence or absence of dense plasma cell infiltrate, intraepithelial neutrophils, surface erosion, intestinal metaplasia, and H pylori on hematoxylin and eosin (H&E)–stained slides were identified in a blinded fashion. If not previously ordered, an immunohistochemical (IHC) stain for H pylori was performed (clone SP48, Ventana Roche, Tuscon, AZ).
Statistical Analysis
Categorical variables were summarized as count and proportion and compared using Fisher’s exact test. Continuous variables were summarized as mean and standard deviation and compared using unpaired t test. A P value <.05 was considered statistically significant. Statistical analysis was performed using GraphPad Prism 6 (GraphPad Software, Inc, La Jolla, CA, USA).
Results
Prevalence of Helicobacter pylori in Gastric Hyperplastic Polyps
Thirty-two cases of gastric hyperplastic polyp were identified, where the nonpolypoid gastric mucosa was separately biopsied and showed evidence of H pylori infection. In this group, 22 polyps (69%) were positive for H pylori by IHC in the polyp and in 16/22 (73%) polyps, the organisms was also recognizable on H&E-stained slides (Figure 1). In contrast, in 50 consecutive gastric hyperplastic polyp where the nonpolypoid gastric mucosa was not biopsied, H pylori was only recognized in 1 hyperplastic polyp on the H&E-stained slide with an additional case demonstrating immunohistochemical evidence of H pylori (2/50; 4%). One patient was a 65-year-old white woman referred from an outside hospital for antral nodules found on her previous esophagogastroduodenoscopy. The patient received treatment for H pylori at the outside institution after the histologic diagnosis of H pylori infection. There was no follow-up after H pylori treatment. The other patient was an 83-year-old white man who was referred for heart surgery from Saudi Arabia and complained of abdominal bloating, gas, and abdominal distention. These symptoms had been ongoing for many years, but were worse before this esophagogastroduodenoscopy. No other laboratory tests were done for H pylori and there was no follow-up.
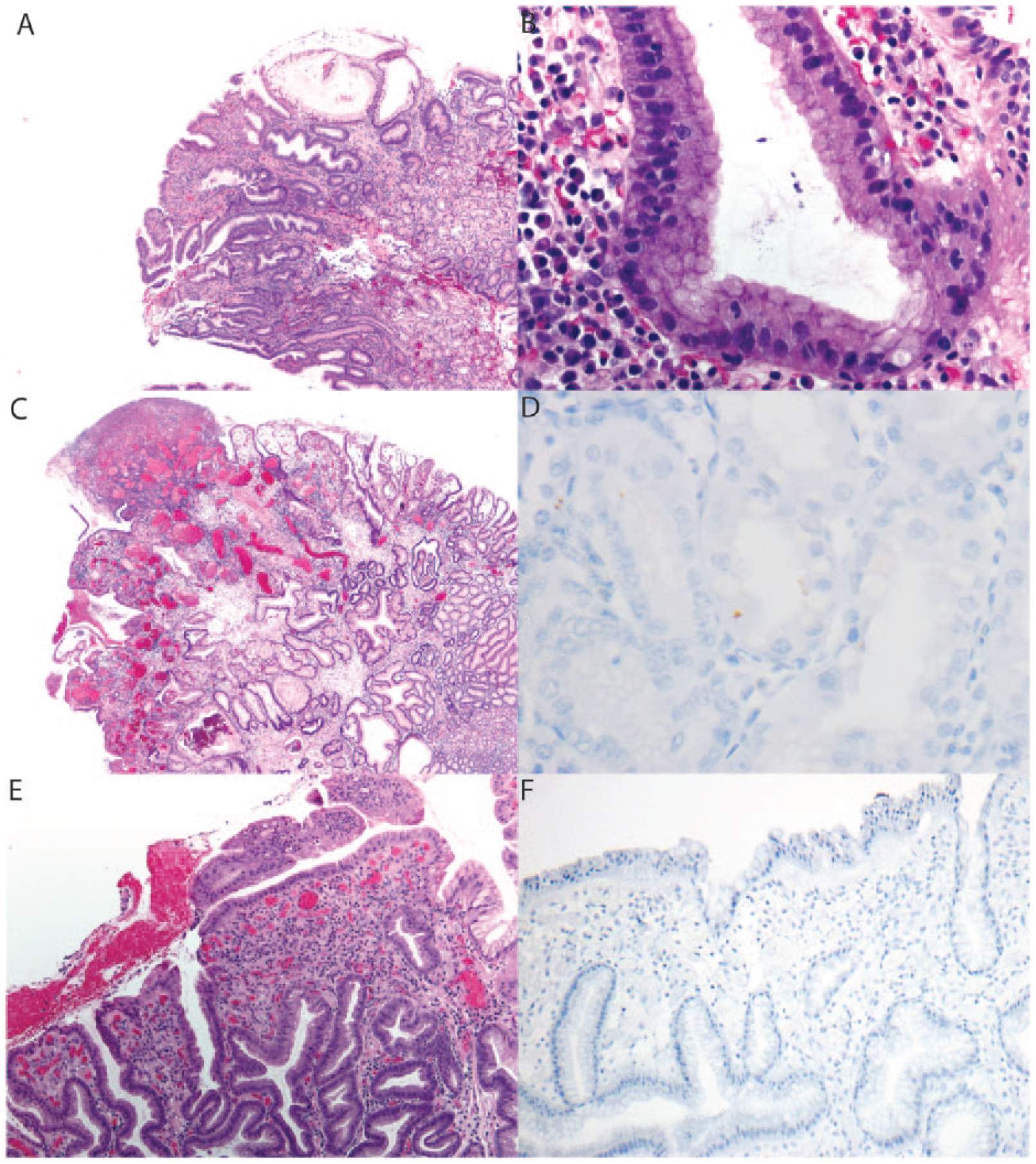
Hyperplastic polyps with and without Helicobacter pylori. (A) A hyperplastic polyp containing H pylori organisms characterized by dense lymphoplasmacytic inflammation. (B) Helicobacter pylori are readily identified on hematoxylin and eosin. (C-D) A hyperplastic polyp associated with H pylori in which organisms were only identified on immunohistochemistry for H pylori. (E) A hyperplastic polyp not associated with H pylori. In this example, there is a lack of dense lymphoplasmacytic inflammation but active (neutrophilic) inflammation is readily apparent. (F) An immunohistochemical stain for H pylori is negative.
Predictive Value of Demographic, Endoscopic, and Histologic Variables for Helicobacter pylori in Gastric Hyperplastic Polyps
The 82 cases of gastric hyperplastic polyp were divided into 2 groups based on the presence or absence of H pylori. Twenty-four polyps contained H pylori organisms. The majority of these polyps were located in the gastric body and the antrum (12 and 7 cases, respectively), 2 polyps were located at the gastroesophageal junction, and 1 in the cardia. The group which did not show the organism, consisted of 58 cases in which almost half (28 cases) were from the antrum, 11 from the gastric body, 8 from the fundus and 1 case each from the cardia and the gastroesophageal junction. Demographic, endoscopic, and histologic variables were retrieved and compared between these 2 groups (Table 1). Indications for endoscopy were similar between the 2 groups with the most common indication being abdominal and/or epigastric pain. Statistical analysis revealed that dense plasma cell infiltrate was associated with the presence of H pylori in the polyp (66% vs 16%, P = .0001) (Table 1). An association was observed between the presence of intraepithelial neutrophils and the presence of the organism (87% vs 64%, P = .0357). Features of mucosa prolapse were assessed given the recent description of gastric mucosal prolapse hyperplastic polyps. 15 Seven polyps had prominent mucosal prolapse, 5 of which were located in the antrum similar to the previous description. Only one of these polyps (located in the antrum) with prominent prolapse was positive for H pylori (P = .6673). Patient’s gender, age, polyp size, the presence or absence of intestinal metaplasia, surface erosion, and multiplicity of the polyp(s) did not correlate with the presence of H pylori.
Comparison of Demographic, Endoscopic, and Histologic Parameters in Gastric Hyperplastic Polyps With and Without Helicobacter pylori.
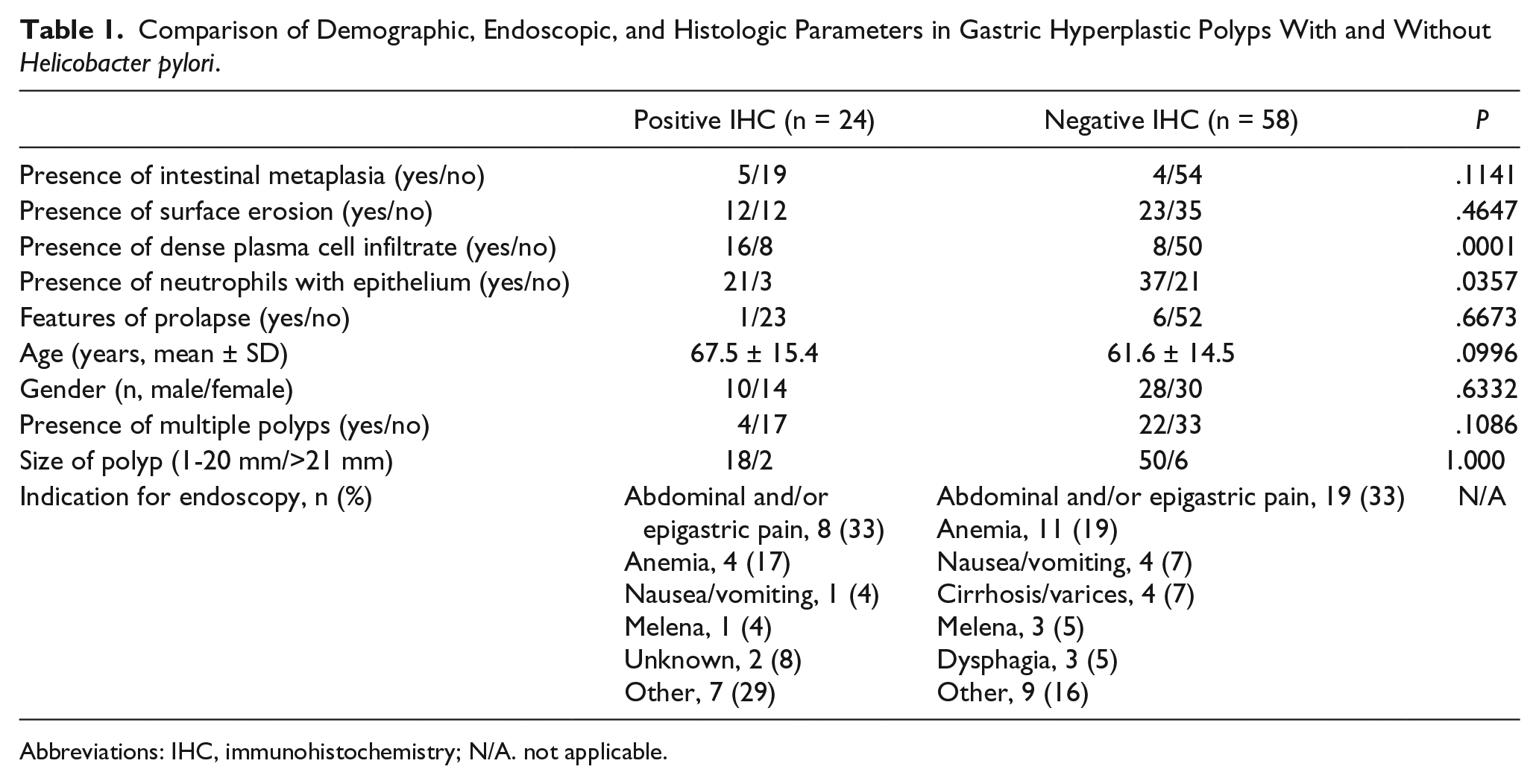
Abbreviations: IHC, immunohistochemistry; N/A. not applicable.
Discussion
Abraham et al 14 analyzed the background mucosa from patients with gastric hyperplastic polyps and demonstrated that 25% arose in the setting of active chronic H pylori gastritis, 21% arose in reactive/chemical gastropathy, and 12% arose in autoimmune gastritis. 14 However, in this study, the presence of H pylori was not evaluated in the hyperplastic polyp. Recently Gonzalez-Obeso et al 15 analyzed 41 confirmed cases of gastric hyperplastic polyp. The surrounding mucosa was sampled in only 10 cases (24%). Evidence of H pylori infection (pathologic or clinical) was present in 20.6% of cases. No mention of the presence of H pylori within the hyperplastic polyp was made in this study. Given that gastroenterologists infrequently biopsy the surrounding mucosa in patients with hyperplastic polyps it is unclear if pathologists should perform special studies to evaluate for H pylori when only the hyperplastic polyp is biopsied. Gastric hyperplastic polyps can be symptomatic and may progress to cancer7,8,10; thus, identifying the cause of gastric hyperplastic polyp formation is of clinical importance given that eradication of H pylori results in regression of these polyps.
Recently, the Rodger C. Haggitt Gastrointestinal Pathology Society published guidelines on when to test for H pylori.
22
According to these guidelines,
H. pylori organisms are not usually present in hyperplastic/regenerative polyps, and, if detected on a polyp surface, they are also present in the background mucosa. We suggest that application of ancillary stains to gastric polyps be limited to certain circumstances. We suggest that application of ancillary stains to gastric polyps may provide useful information when applied to chronically inflamed hyperplastic/regenerative polyps, but are otherwise unhelpful.
However, no data exist on the prevalence of H pylori within the gastric hyperplastic polyp to support or refute these recommendations. We undertook this study to determine how often H pylori are identified in hyperplastic polyps caused by H pylori infection. Furthermore, we determined how often H pylori is identified in biopsies of gastric hyperplastic polyps in which the surrounding mucosa was not sampled. We also identified useful features that can guide H pylori testing in gastric hyperplastic polyps.
Approximately 70% of the hyperplastic polyps arising in H pylori gastritis contain the organisms. Most of these organisms were easily identifiable using routine H&E-stained slides. In contrast, only 2 hyperplastic polyps from 50 consecutive cases in which the nonpolypoid mucosa was not sampled contained H pylori. Of the 24 gastric hyperplastic polyps containing H pylori organisms, a dense plasma cell infiltrate and presence of neutrophils within gastric epithelium were more common than in polyps without the organisms. However, 33% lacked dense lymphoplasmacytic inflammation, and neutrophilic inflammation was commonly seen in the absence of H pylori (64%). Other features including intestinal metaplasia, polyp number, and polyp location were not associated with the presence of H pylori. The Gastrointestinal Pathology Society guidelines state that hyperplastic polyps “near the gastroesophageal junction are virtually never associated with H. pylori infection” 22 ; however, in this study 3/24 (12%) gastric hyperplastic polyps with H pylori arose in the gastroesophageal junction/cardia.
Pathologists often encounter gastric hyperplastic polyps and determining the etiology by which the hyperplastic polyp arose can help guide therapy. Given that the nonpolypoid mucosa is infrequently sampled, determining the algorithm by which one assesses for H pylori organisms would be helpful. Our results demonstrate that when H pylori is the underlying cause of gastric hyperplastic polyps, the organisms are often present within the gastric polyp. The presence of dense plasma cell infiltrate and intraepithelial neutrophils can help guide the pathologist to hunt carefully for organisms or perform special stains although these features are not entirely sensitive or specific for the organism. To our knowledge, this is the first study to specifically evaluate for the presence of H pylori within gastric hyperplastic polyps and provides empirical data to guide the use of special stains for H pylori in this setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.