
Abstract
Conjunctival melanoma is the second most common conjunctival malignancy. Its differential diagnosis with other conjunctival melanocytic neoplasms is inherently difficult. The presence of epithelial cysts is a useful feature in conjunctival tumors and favors a benign lesion. Herein 2 cases of conjunctival melanoma with cysts are presented. To the best of our knowledge, this is the first series of conjunctival melanoma with epithelial inclusion cysts. This series emphasizes the importance of considering several malignant features when reviewing conjunctival melanocytic lesions, as malignancy can exist even in the presence of epithelial inclusion cysts.
Introduction
Conjunctival melanocytic tumors are the most frequent conjunctival neoplasms, reaching up to 53% of all conjunctival tumors. 1 They are classified according to the Armed Forces Institute of Pathology into nevus, primary acquired melanosis (PAM), and melanoma. 2 Nevi are the most common, accounting for 28% of all tumors of the conjunctiva. 1 In conjunctival pigmented lesions, PAM corresponds to 38.8% of the cases, while conjunctival melanoma (CM) represents only 9.4% of the lesions. 3 However, its importance lies in its relatively high capability of metastasizing to local lymph nodes, which is estimated to be 27% at 10 years for T1 lesions. 4
The diagnosis of conjunctival melanocytic lesions is a challenge. Histologically, conjunctival melanocytic nevi are classified similarly as in the skin, including junctional, compound, and subepithelial nevi. 5 Histologically, PAM are subclassified as without atypia when melanocytic hyperplasia is limited to the basal layer and no atypia is present in the form of nuclear enlargement nuclei, prominent nucleoli, or nuclear membrane irregularity. PAM with atypia is defined histologically as an intraepithelial melanocytic proliferation showing any degree of melanocytic atypia and/or increased cellularity, usually with infiltration of the superficial layer of the conjunctival epithelium (pagetoid infiltration). 5 CM can be difficult to diagnose, even for experienced pathologists familiar with this anatomic location. The diagnosis of melanoma is rendered when malignant cells are present within the stroma. Features present in melanoma that may help to differentiate from a nevus are: the presence of atypical mitotic figures in the deeper portion of the melanocytic proliferation; the loss of maturation; asymmetry of the lesion; and invasion of adjacent structures, such as the cornea or sclera. 5 Moreover, an architectural feature classically described in benign conjunctival melanocytic lesions is the presence of conjunctival inclusion cysts (IC) lined by conjunctival epithelium with goblet cells. 6 Usually, presence of IC is associated with nevi, being present in up to 50% of the cases and when present, follow-up with pictures is recommended. 7 IC are likewise considered to be absent in primary acquired melanosis and melanoma. It has also been shown that IC develop progressively over time and that they are rare in recently developed lesions.5,6,8 In summary, clinical and histopathological recognition of tumor cysts is considered a key point in differentiating conjunctival nevus from malignant melanoma as many other features may overlap. 7
Herein is presented the first case series of CM with conjunctival inclusion cysts. In the first case, the cystic structures are located in the adjacent PAM with atypia, while in the second case, the cystic structures are present within the bulk of the tumor.
Case 1
A healthy 51-year-old Caucasian woman from Brazil referred a 20 × 10 mm slowly growing palpebro-conjunctival pigmented nodule occupying the central part of the upper eyelid and affecting the palpebral edge, impeding the growing of the eyelashes. The lesion had been present for 2 years but rapidly grew in the past 8 months (Figure 1A). At this time, a flat pigmented lesion in the adjacent palpebral conjunctiva extending to fornix and bulbar conjunctiva was noted (Figure 1B). Another flat pigmented lesion was observed in the lower palpebral conjunctiva extending to the fornix (Figure 1C). At examination, her best-corrected visual acuity (BCVA) was 20/20 in both eyes. Intraocular pressure (IOP) was 10 mm Hg in both eyes. Slit-lamp biomicroscopy of the right eye and fundus biomicroscopy of both eyes were unremarkable.
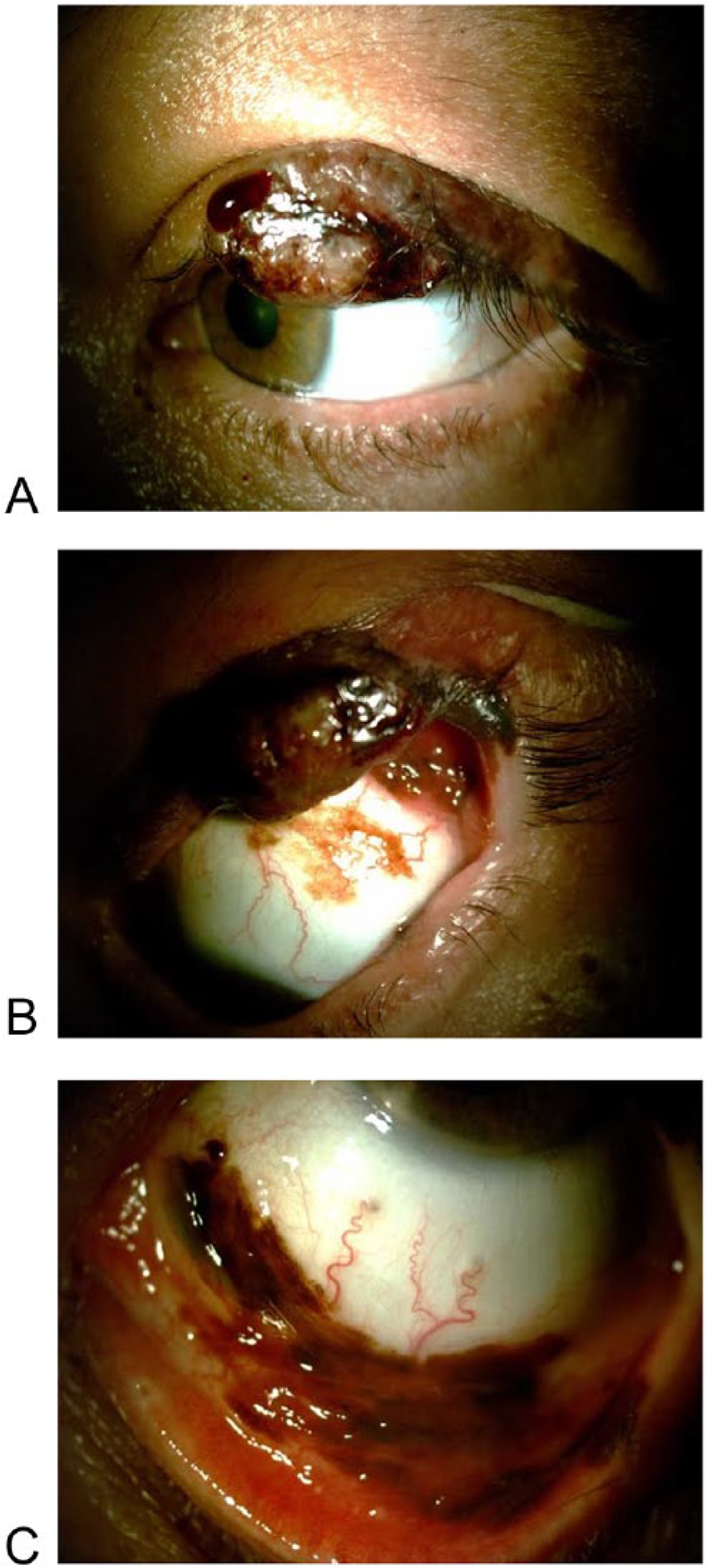
Left eye clinical images. (A) A nodular partially pigmented, ulcerated 20-mm tumor with madarosis, compromising the mid third of the palbebral margin of the upper eyelid is seen. (B) After eversion, a 23 × 16 mm patchy, slightly nodular pigmented tumor occupying the superior bulbar, fornix, and palpebral conjunctiva is seen. (C) A 22 × 9 mm pigmented, patchy tumor compromising the inferior bulbar, fornix, and palpebral conjunctiva is observed.
Incisional map biopsy of the eyelid and conjunctiva were performed. In the eyelid, a melanocytic proliferation of large cells with large, irregular, and pleomorphic nuclei infiltrating the dermis and the epidermis was observed (Figure 2A). The malignant cells were also positive for melan-A and HMB-45, which is consistent with malignant melanoma. The conjunctival biopsies (Figure 2B and C) showed an intraepithelial atypical proliferation of melanocytes arranged in nests or in a lentiginous spread formed by pigmented large cells with hyperchromatic, irregular, and pleomorphic nuclei with prominent nucleoli. The final diagnosis was consistent with PAM with atypia high grade.
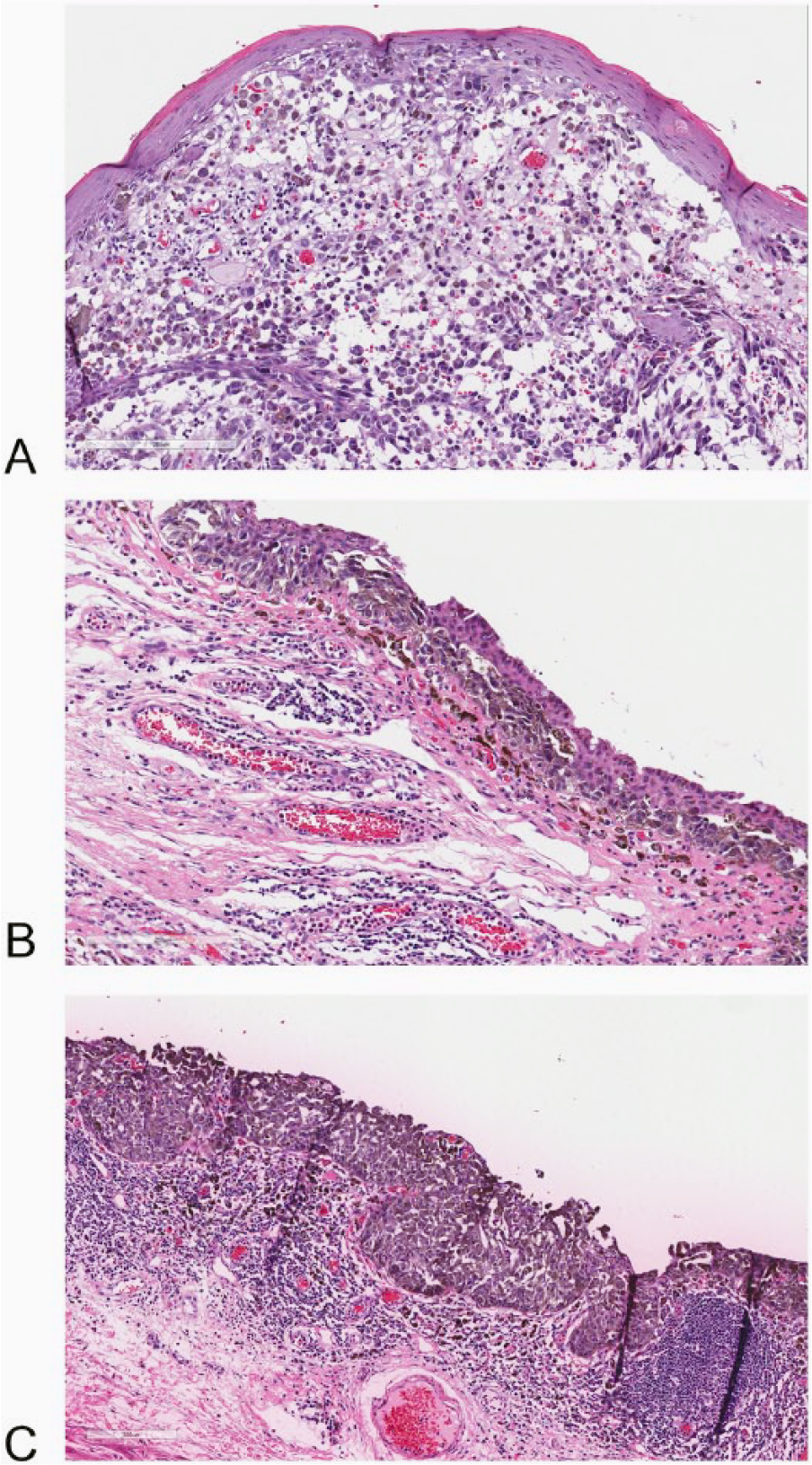
Incisional map biopsy of the eyelid and conjunctiva: (A) A fragment of skin infiltrated by a discohesive tumor. The neoplastic cells are large with an irregular and hiperchromatic nuclei. The cytoplasm present pigmented granules. The tumor infiltrate the epidermis and the dermis. (B and C) A fragment of conjunctiva showing an infiltration of large cells with pigmented cytoplasmic granules and large irregular nuclei in lentiginous spread, nest, or occupying the full thickness of epithelium. In the stroma, a dense inflammatory reaction is present.
Because of these findings, imaging studies were performed to evaluate the extension. Orbit and skull magnetic resonance imaging showed no extension into the orbit, bone erosion or intraocular involvement. Computed tomographic scans of the neck, thorax, and abdomen were also negative for metastatic disease.
Exenteration was performed due to the presence of an eyelid melanoma accompanied by a large PAM with atypia. Gross examination revealed the aforementioned lesions. No intraocular or orbital extension was noticed. Microscopically, the elevated tumor was composed of large epitheloid cells with nuclei that were large, pleomorphic, irregular and with prominent nucleoli. These were consistent with melanoma. The malignant cells infiltrated the conjunctiva, the tarsal plate, the skin, and the skeletal muscle (Figure 3A). Moreover, the adjacent conjunctiva showed an extensive intraepithelial infiltration of melanocytic cells with large, irregular and pleomorphic nuclei with prominent nucleoli. These morphological findings were consistent with PAM with atypia. The malignant cells also infiltrated epithelial inclusion cysts (Figure 3B). The rest of the conjunctiva showed multifocal extensive PAM with atypia, while the margins were free of neoplastic involvement. After a year of follow-up, no recurrences were noted. The final diagnosis was conjunctival melanoma infiltrating the conjunctiva, the tarsal plate, the skin, and the skeletal muscle. The Breslow index was 5.4 mm.
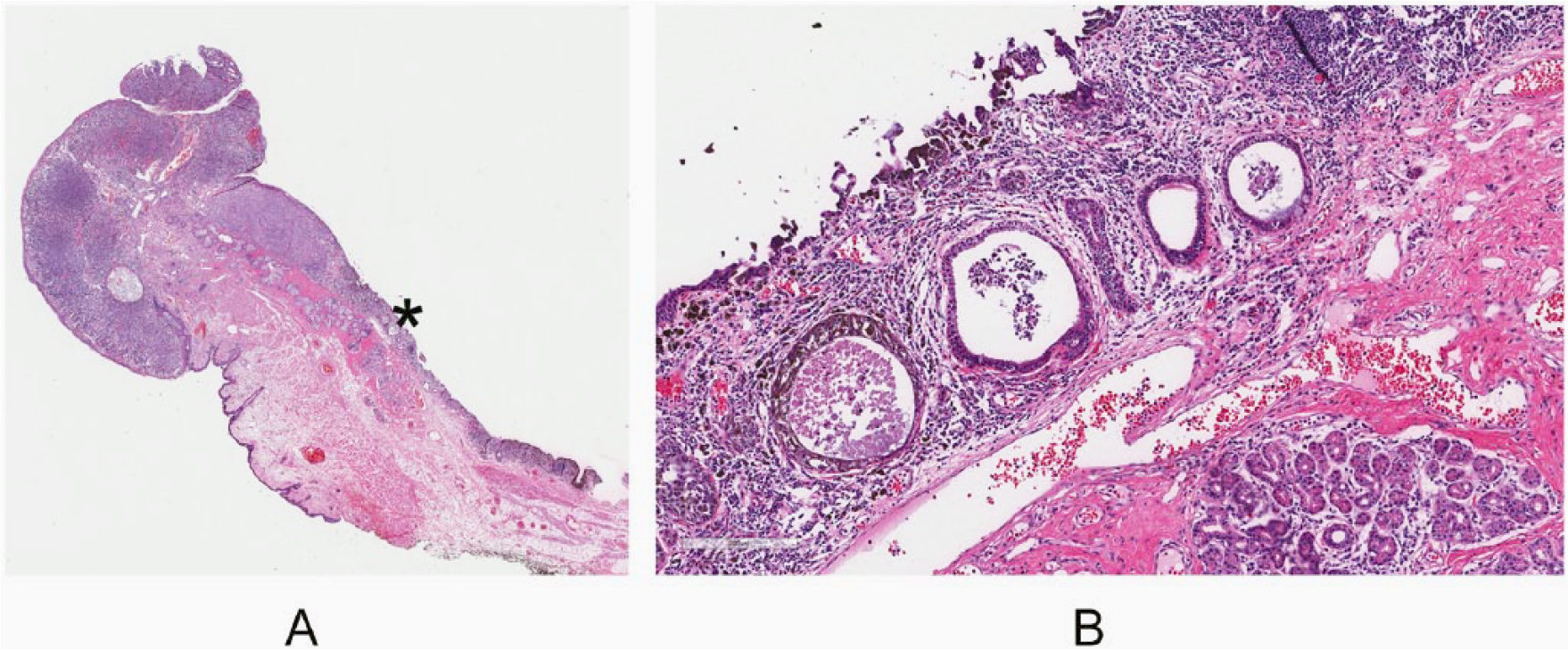
Exenteration specimen findings: (A) Segment of eyelid with a pigmented tumor infiltrating the skin, the palpebral edge, conjunctiva and tarsal plate. An asterisk (*) shows the area highlighted in figure B. (B) A fragment of conjunctiva adjacent to the bulk of the tumor showing an infiltration of large cells with pigmented cytoplasmic granules within the superficial epithelium and the epithelium lining the conjunctival inclusion cyst.
Case 2
A 37-year-old Caucasian man presented with a 6 mm pigmented lesion of the nasal conjunctiva. He has had this lesion for 15 years but noticed rapid growth in the past 6 months. The lesion was excised and cryotherapy was applied to the surgical margins. Histopathologically, the lesion was composed of large epitheloid cells with large irregular and pleomorphic nuclei (Figure 4A and B). The cytoplasm was pigmented and numerous mitotic figures were observed (Figure 4C). In addition, conjunctival epithelial cysts were noticed within the bulk of the lesion (Figure 4D). The tumor infiltrated the deeper conjunctival stroma and the margins were free of neoplastic involvement. The Breslow index was 2.1 mm. The diagnosis of conjunctival melanoma was rendered. Adjuvant therapy with 2 cycles of mitomycin C 0.02% (MMC) 4 times daily for 14 days per cycle was administered. After 4 years of follow-up, no recurrence was noted.
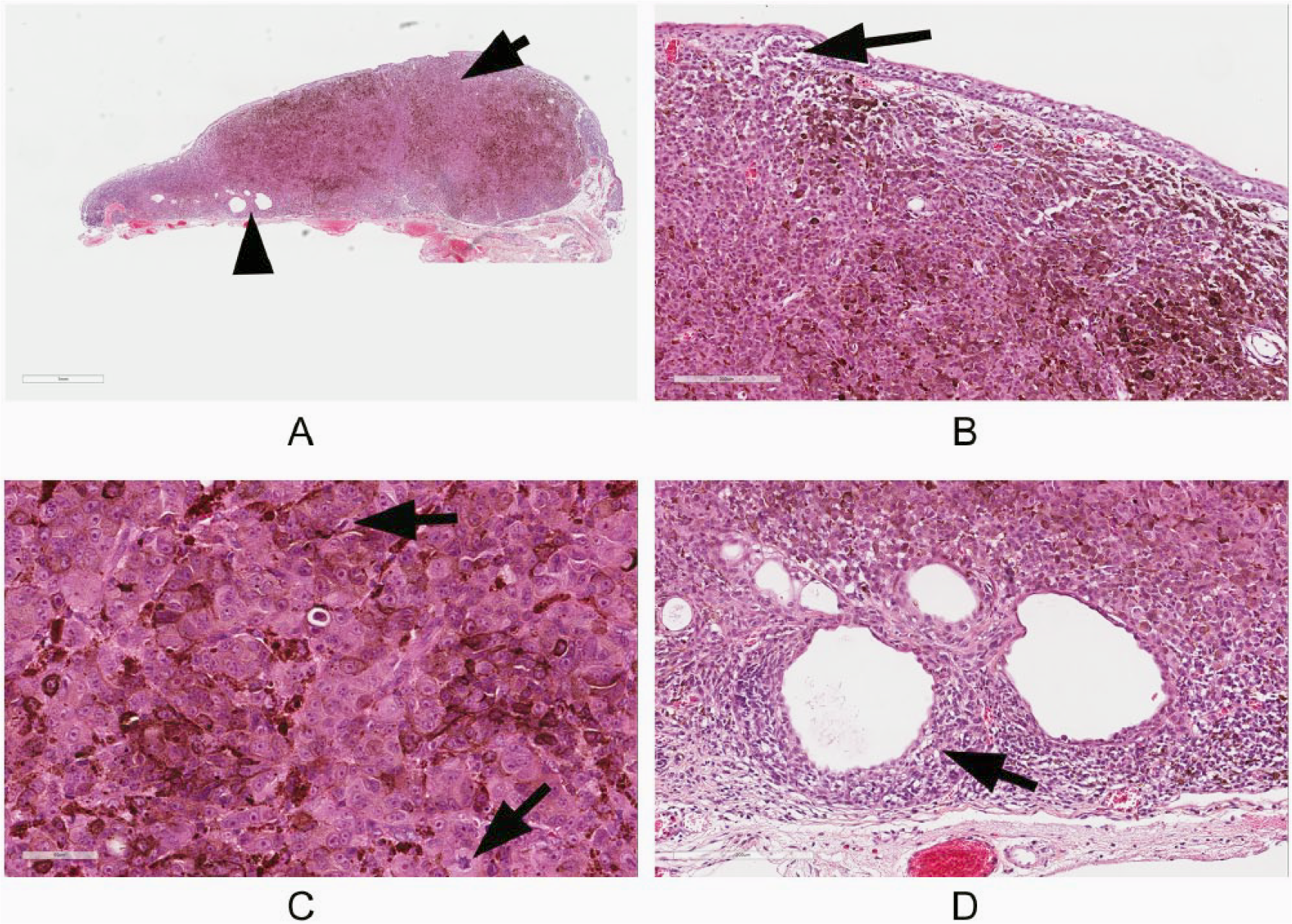
Excisional biopsy of the conjunctival tumor. (A) Low power view of a pigmented tumor infiltrating the conjunctiva. The arrow shows the area highlighted in figure B and the arrowhead highlights the area illustrated in figure D. (B) The tumor is composed by large cells with pigmented granules and large, hypercromatic nuclei. Note the intraepithelial infiltration (arrow). (C) High-power view of the tumor cells showing an irregular nuclei with prominent nucleoli and numerous mitotic figures (arrows). (D) Epithelial inclusion cyst in the bulk of the lesion infiltrated by neoplastic cells (arrow).
Discussion
We report on 2 cases of CM with IC that can lead to a misdiagnosis of a benign melanocytic lesion either clinically or histopathologically. The first case represented a patient with a 2-year enlarging conjunctival pigmented tumor in which the diagnosis was made in an advanced stage of the disease. The patient consulted late probably due to inadequate access to specialized care. The second patient presented with a long-standing lesion that suddenly started growing. Fortunately, this case was diagnosed early, which resulted in a more conservative treatment with a better prognosis.
Our cases comprised patients aged 51 and 37 years, emphasizing the fact that this lesions may appear in adults at any age, although CM are frequently seen in middle-aged to elderly patients with fair skin, with 72% incidence after 50 years of age.4,9 Moreover, in our series both cases arose from PAM with atypia; this is the most common scenario, corresponding to about 53% to 75% of CM. Nevertheless, 18% to 30% of the cases arise de novo and only 5% arises from nevi.2,10 It is important to note that, while unlikely, in both cases a preexisting subepithelial nevus with cysts could have been overrun by the melanoma.
The diagnosis of conjunctival melanocytic tumors is usually difficult for the general pathologist due to infrequent exposure to these specimens and to the difference in the nomenclature between the pigmented tumors of the conjunctiva and skin. To facilitate understanding, a parallel with morphologically similar skin conditions is represented in Table 1.
Correlation Between Skin and Conjunctival Melanocytic Lesions.
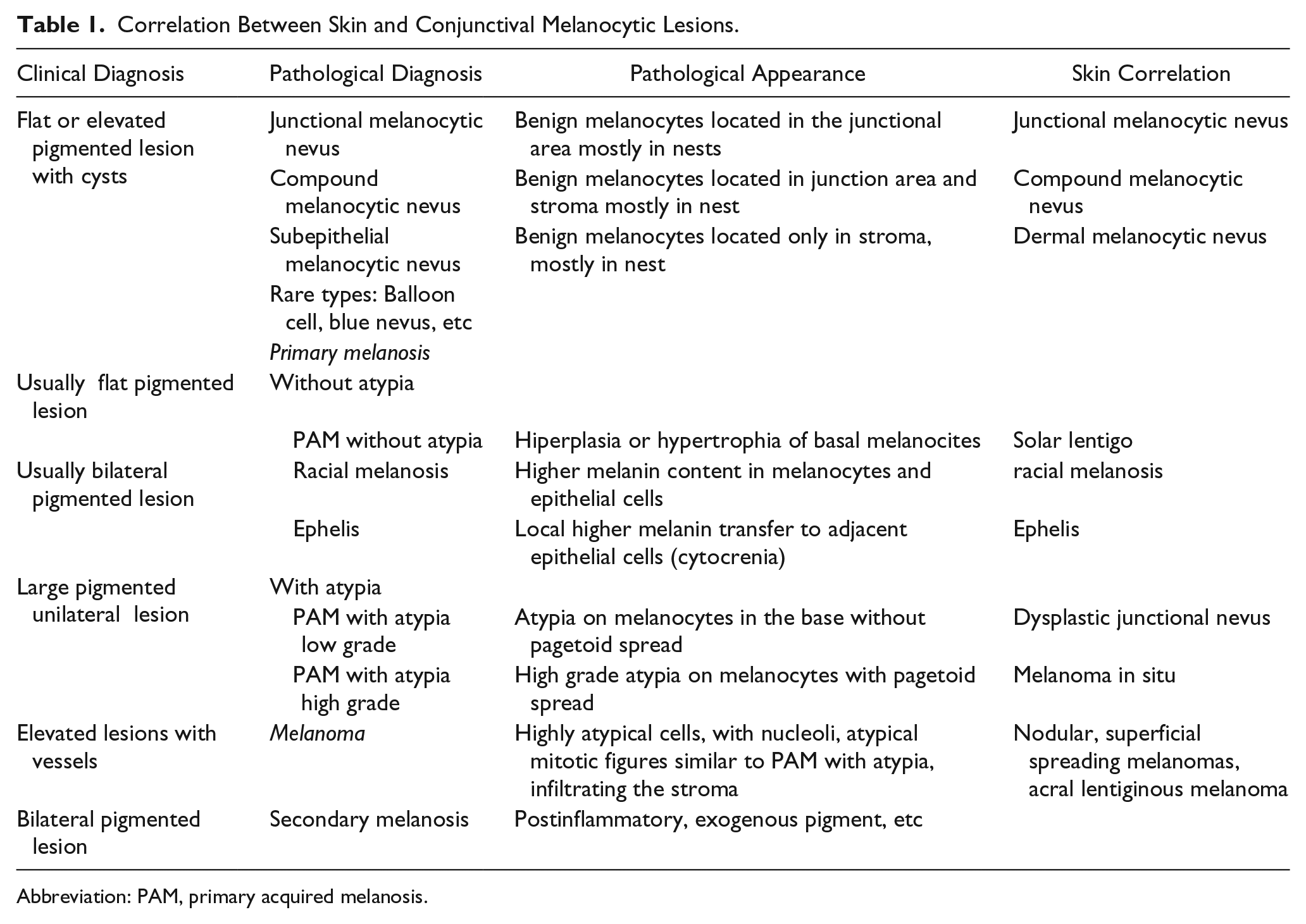
Abbreviation: PAM, primary acquired melanosis.
In this series, the presence of IC raised to a new level the inherently difficult diagnosis of conjunctival melanocytic lesions. A review of the literature was performed to find reports of CM with epithelial cysts, and 2 series were encountered. One was by Reese 11 in 1937, describing submucosal cysts in a so-called premalignant lesion. Unfortunately, pictures were lacking and the description did not clearly define the epithelial nature of the cyst; furthermore, it seemed that they were more likely to be pseudocysts of nevoid cells. The second one, reported by Daxecker et al 12 in 1988, described a CM with inclusion cysts arising from a melanocytic nevus. On review of the images, it seemed that a nevoid component was displaced and compressed by the melanoma, similar to what had been reported in our first case. However, in this case, instead of a nevus, it was PAM with atypia. The significance of this is that an incisional biopsy in the nevoid area could lead to a misdiagnosis. It was fortunate that in our case, malignant cells surrounding the cyst could aid in the correct diagnosis. To avoid insufficient sampling, incisional biopsies in the conjunctival melanocytic lesion must include 3 areas: the periphery, the thicker, and another random region. 13
When difficulties are encountered in defining the malignancy of a melanocytic lesion, ancillary studies might be helpful. In cases of melanocytic origin the red chromogen subtract for immunohistochemistry is advised in order to avoid misinterpretation with melanin pigment. 14 Immunohistochemical studies show that HMB-45 is more abundantly expressed in malignant tumors than in benign lesions. 15 Furthermore, S100A1 positively stains conjunctival nevi (89%), PAM (71%), conjunctival melanomas (100%), and all uveal melanoma (100%). 16 High Ki-67 nuclear expression index is another useful marker to support the malignant nature of the tumor. 14 Finally, the loss of p16 expression in CM when compared with the markedly high levels seen in PAM with atypia and nevus may aid in the diagnosis. 17
The reported cases showed other interesting features. In the first case, the melanoma was present in both the skin and the conjunctiva, but the presence of PAM with atypia in the adjacent conjunctiva and the absence of intraepithelial involvement in the adjacent skin favored the diagnosis of CM extending to the skin.
From a clinical standpoint, all melanocytic lesions that are rapidly growing must be excised. 18 In these kind of lesions, complete surgical resection of the conjunctival and corneal components with tumor-free margins supplemented by conjunctival cryotherapy and alcohol corneal epitheliectomy is advised. This was performed in the patient in case 2 who had a localized tumor and free margins, so that the excisional biopsy with the MMC treatment was curative. Unfortunately, the patient in case 1 was staged as T3b (The American Joint Committee on Cancer, 2010) due to the eyelid invasion. 4 It is estimated that in patients with melanomas staged as T3b, there is recurrence in 75% after 5 years of follow-up; distant metastases in 39%, regional lymph node metastasis in 45% and melanoma-related death in 15%. 10 In case 1, positive map biopsy for PAM with atypia was the indication for the exenteration, and no recurrence after a year was seen.
Conclusions
This series documents evidence of 2 extraordinary cases of conjunctival melanoma with epithelial inclusion cysts. This finding could lead clinicians or pathologists to render a misdiagnosis. Furthermore, close follow-up with imaging is advised in all melanocytic lesions, even if inclusion cysts are present, to detect the infrequent cases that undergo malignant transformation in an early stage.
Footnotes
Acknowledgements
We want to specially thank Dr Jade M. Lasiste for her invaluable collaboration in the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.