
Abstract
Ciliated foregut cysts typically arise in the liver and pancreas, with rare cases reported to arise in the gallbladder wall. Herein, we describe an unusual case of a patient with a ciliated foregut cyst arising from the wall of the common hepatic duct, which has not been reported previously. As a result of its unique anatomical location, the cyst was mistaken for a type II choledochal cyst on preoperative imaging. The cyst caused intermittent biliary obstruction that resolved following surgical resection.
Introduction
Ciliated foregut duplication cysts are defined by the presence of a respiratory type of epithelial lining, characterized by pseudostratified ciliated columnar epithelium. Ciliated foregut cysts have been well described in the liver and pancreas.1,2 A few case reports describe ciliated foregut cysts arising from the gallbladder wall.3-5 To our knowledge, however, there are no reports of ciliated foregut duplication cysts arising in the extrahepatic biliary tree. Here, we report an unusual case of a ciliated foregut cyst arising from the wall of the common hepatic duct, clinically and radiologically mimicking a type II choledochal cyst.
Case
A 57-year-old woman reported a long-standing history of recurrent, brief, and self-limited episodes of jaundice and right upper quadrant pain. These episodes were accompanied by decreased appetite, nausea, vomiting, and early satiety. Progression of the patient’s symptoms motivated a presentation to the emergency room and admission to hospital for workup of jaundice. At presentation to the emergency room, her total bilirubin was 100.0 µmol/L (normal 0-20 µmol/L), direct bilirubin 58.5 µmol/L (normal 0-5.1 µmol/L), alanine transaminase (ALT) 255 U/L (normal 0-41 U/L), alanine aspartate transaminase (AST) 171 U/L (normal 0-38 U/L), and alkaline phosphatase 260 U/L (normal 40-129 U/L). Her white blood cell count, hemoglobin, international normalized ratio, urea, and creatinine were all within the normal range.
Abdominal ultrasound (Figure 1A) and magnetic resonance imaging (MRI; Figure 1B and C) including magnetic resonance cholangiopancreatography (MRCP) demonstrated a cystic lesion arising next to the common hepatic duct. The cystic lesion contained debris that was of different echogenicity and MRI signal intensity than that of normal bile. Although neither imaging study showed definite communication with the biliary tree, the preoperative imaging findings were considered typical for a type II choledochal cyst.
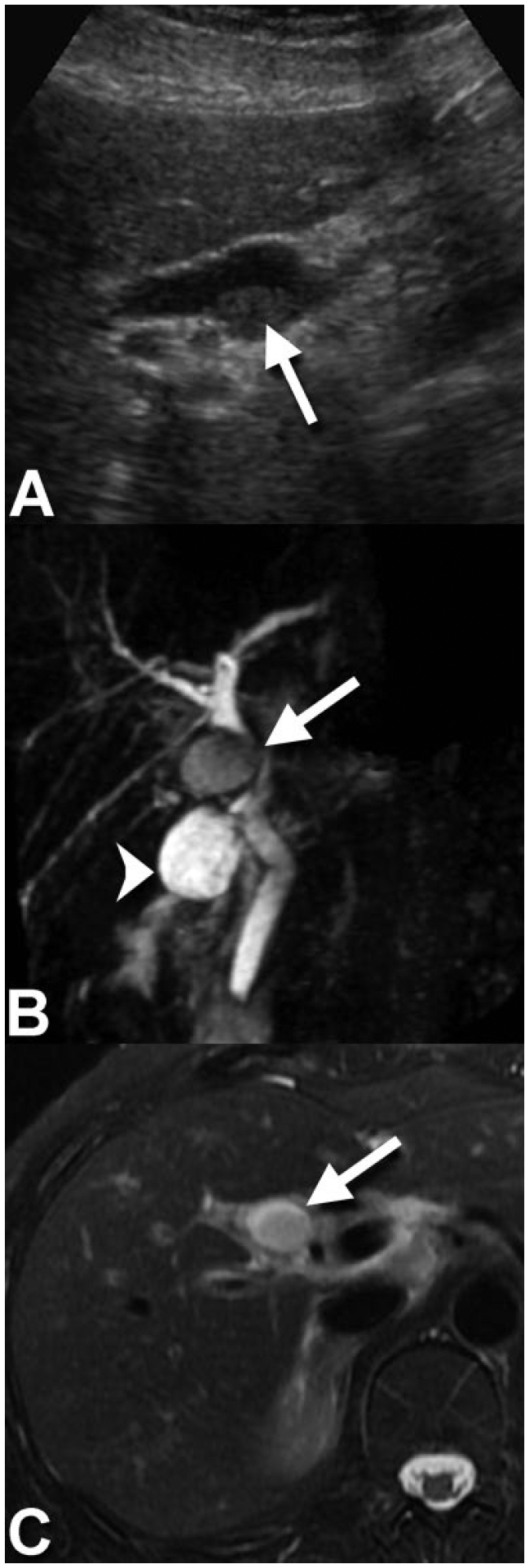
(A) Grayscale ultrasound image oriented sagittal to the common hepatic duct demonstrates a periductal cystic lesion (arrow) with layering echogenic debris. This image suggests that the cyst might communicate with the common hepatic duct, as expected for a type II choledochal cyst. (B) Full-volume maximum intensity projection (MIP) magnetic resonance cholangiopancreatography (MRCP) and axial fat-saturated T2-weighted (C) magnetic resonance (MR) images confirm a cystic lesion (arrows) arising adjacent to the common hepatic duct. As on the ultrasound, both MR images show intraluminal debris of intermediate T2 signal intensity. In particular, the heavily T2-weighted MRCP image (B) clearly depicts the cystic lesion to be of different signal intensity than that of the gallbladder (arrowhead) and biliary ducts. MRCP also shows compression of the common duct with no definite communication with its lumen. There is no upstream biliary duct dilation.
The patient underwent an elective cholecystectomy with resection of a segment of common hepatic duct including the cyst. Intraoperatively, the cyst was confirmed to be attached to the common hepatic duct in close proximity to the cystic duct and gallbladder. An anatomically high division of the common hepatic duct was noted at surgery. Following resection of the cyst and bile duct segment, a Roux-en-Y hepaticojejunostomy was performed
Grossly, the unilocular cyst measured 1.7 × 1.5 × 1.2 cm. It was thin-walled (<0.2 cm in thickness) and contained yellow-gray liquid, which was distinctly different in color from the green bile within the gallbladder. The cyst contained no stones. The cyst wall was attached to the wall of the common hepatic duct. However, the lumen of the cyst did not communicate with the lumen of the bile duct.
Microscopy revealed that the cyst had a ciliated, pseudostratified columnar epithelial lining, typical of respiratory type mucosa (Figure 2). The cyst wall was collagenous with no smooth muscle. The epithelial lining demonstrated strong expression of thyroid transcription factor 1 (TTF1), cytokeratin 7, and cytokeratin 19 by immunochemistry. Scattered synaptophysin positive endocrine cells were identified in the epithelial lining. The cyst lining did not express cytokeratin 20, estrogen receptor, or progesterone receptor by immunohistochemistry.
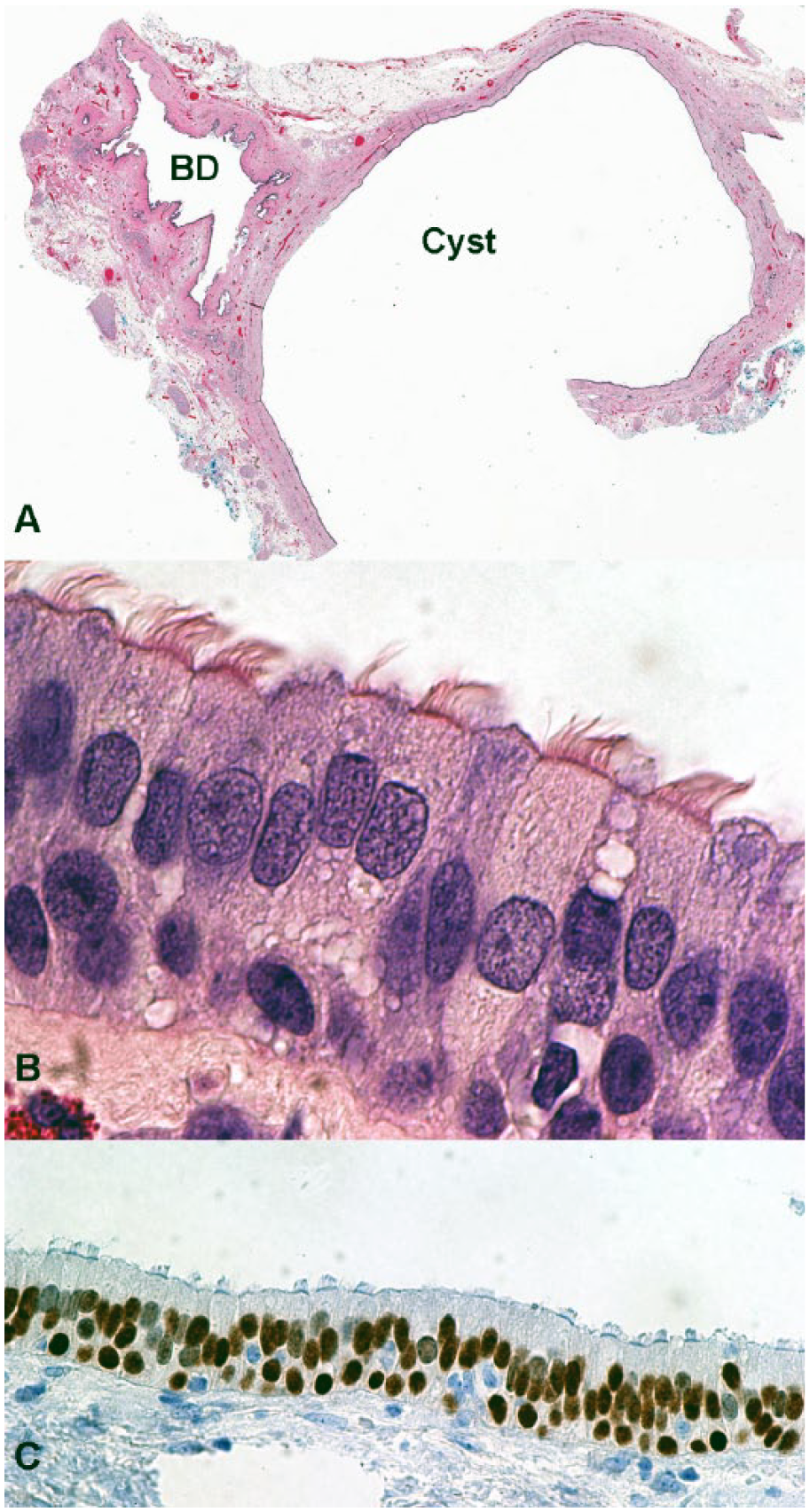
(A) Cross section of the common hepatic bile duct (BD) with a cross section of the adjacent simple cyst. (B) High magnification (1000×) shows the ciliated respiratory-type epithelial lining of the cyst. (C) Immunohistochemistry shows expression of thyroid transcription factor 1 (TTF1) in the epithelial lining of the cyst.
At the time of discharge from hospital 1 week after surgery, the patient was feeling well and tolerating a full diet with minimal abdominal tenderness related to the surgery. Biochemically, her bilirubin, AST, ALT, and alkaline phosphatase had normalized by discharge. At follow-up 1 year after the surgery, the patient has not developed any recurrent episodes of biliary obstruction.
Discussion
This case represents a unique anatomical location for a ciliated foregut duplication cyst, which resulted in an unusual clinical presentation. The patient’s intermittent episodes of jaundice were presumably related to compression of the common hepatic duct by the cyst. The morphology and anatomical location of this particular cyst on imaging and gross examination are strikingly similar to that of a type II choledochal cyst, which is a diverticulum of the common duct (Figure 3). However, gross pathologic examination showed no communication of the cyst contents with the common hepatic duct lumen, which is uncharacteristic of a type II choledochal cyst. 6 Histology provided the definitive diagnosis of a ciliated foregut cyst based on the characteristic respiratory epithelial lining. The expression of TTF1 in the ciliated cells and the presence of scattered neuroendocrine cells (highlighted with synaptophysin) is the characteristic immunophenotype of respiratory type mucosa. This pattern of immunohistochemistry has previously been reported to be expressed in the epithelial lining of ciliated foregut cysts.7,8 In contrast, the biliary epithelial lining of a choledochal cyst would not express TTF1.
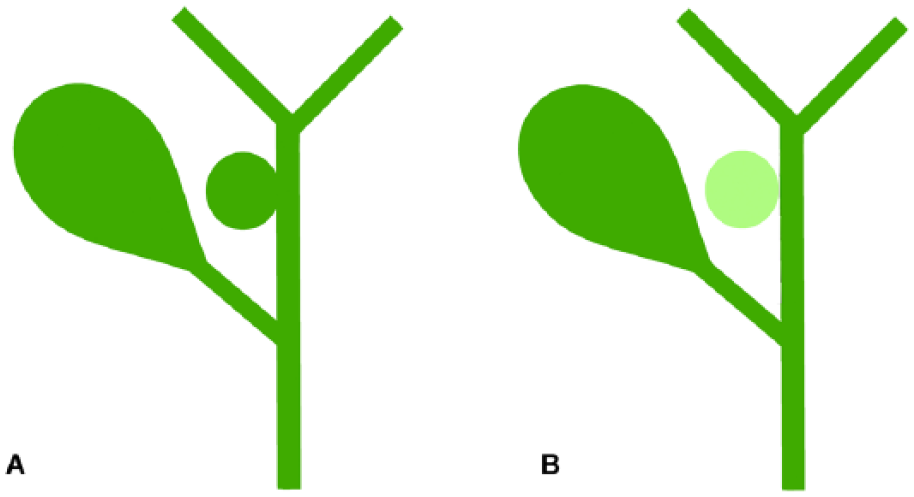
(A) A type II choledochal cyst of the common hepatic duct is a diverticulum of the bile duct wall which is in communication with the biliary tree and contains bile, illustrated in dark green. (B) In contrast, the ciliated foregut cyst in this case had a similar anatomical location to a type II choledocal cyst, but it did not communicate with the biliary tree and it contained no bile.
In this case, a ciliated foregut cyst was distinguished from a type II choledochal cyst based on histologic examination after surgical resection. However, communication with the biliary tree is characteristic of a type II choledochal cyst, and the absence of this communication on imaging might suggest the diagnosis preoperatively. In particular, MRI with gadoxetic acid (Bayer Healthcare Pharmaceuticals, Wayne, NJ; marketed as Eovist in the United States and Primovist in Canada, Europe, and Asia), a contrast agent, which is 50% excreted via the biliary and renal pathways, can demonstrate with certainty whether a lesion communicates with the biliary tree or not.
The distinction between a choledochal cyst and ciliated foregut cyst is important because the two entities are associated with a markedly different risk of neoplastic transformation. Dysplasia, or biliary intraepithelial neoplasia (BilIN), was present in 28.5% of choledochal cysts in one North American series. 9 The frequency of associated malignancy in surgically resected choledochal cysts was 7.0%, 14.3%, and 26.0% in 3 studies evaluating the risk of malignant tranformation.9-11 The risk of malignant transformation has also been observed to increase with patient age.9,10 In contrast, ciliated foregut cysts are generally considered benign, although rare cases of squamous cell carcinoma have been reported in association with intrahepatic ciliated foregut cysts.12-15 Establishing whether a cyst in the biliary tree is a choledochal or ciliated foregut cyst prior to surgery may therefore alter patient management and prognosis. Because the cyst in our case caused intermittent biliary obstruction, surgical intervention was required to relieve the patient’s symptoms irrespective of the histological diagnosis.
Footnotes
Authors’ Note
According to institutional policy, the patient provided informed, written consent for publication of a de-identified case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jonathan Cottreau’s summer research work on this case report was sponsored by the Dalhousie University Medical School Research in Medicine summer studentship program.