
Abstract
This report describes the management of an unusual case of oral pemphigus vulgaris (PV). The patient was referred for a painful single bullous lesion together with a small proliferative area localized in the soft palate. Histology and direct immunofluorescence data were consistent for PV but disclosed unusual signs of high-grade dysplasia in the proliferative area. At surgical removal of the dysplastic area 1 week after the start of cortisone therapy there was no evidence of dysplasia. Histological signs of high-grade dysplasia in oral mucosa are often associated with concurrent or subsequent carcinoma. However, severe inflammation may induce reactive epithelial cell changes and hence mimic histologic dysplasia. Pathologic evaluation of dysplasia in an inflammatory disease like PV may be a diagnostic challenge and a careful pathological evaluation is advisable before choosing between surgical and medical approach.
Introduction
Pemphigus vulgaris (PV) is an immune-mediated disorder in which immunoglobulin G (IgG) antibodies target desmosomal proteins to produce intraepithelial, mucocutaneous blistering. 1 Oral lesions are the first manifestation of the disease in 50% to 90% of cases and the blisters may later spread to the skin.2-4 Diagnosis of PV is based on 3 major criteria: clinical features, histology, and immunological detection of autoantibodies.5,6 A skin or mucosal biopsy should be taken for histology and direct immunofluorescence (DIF), the latter requiring perilesional intact or clinically uninvolved skin. Suprabasal acantholysis and blister formation is highly suggestive of PV but the diagnosis should be confirmed by the characteristic deposition of IgG in the intercellular spaces of the epidermis. 7
The accidental detection of cytological atypia in histology is unusual in an incisional biopsy performed for suspected blistering disease and it may be a key issue in defining the appropriate treatment. The finding of dysplasia in oral epithelium may herald an oral squamous cell carcinoma (OSCC) or a high-risk oral potential malignant lesion (OPML) and PV has been associated with malignancies of different histogenesis.2,8-12 Conversely, severe inflammation may induce reactive epithelial cell changes that mimic dysplasia.
The present report describes the management of a patient with PV presenting unusual histological signs of high-grade dysplasia.
Case Report
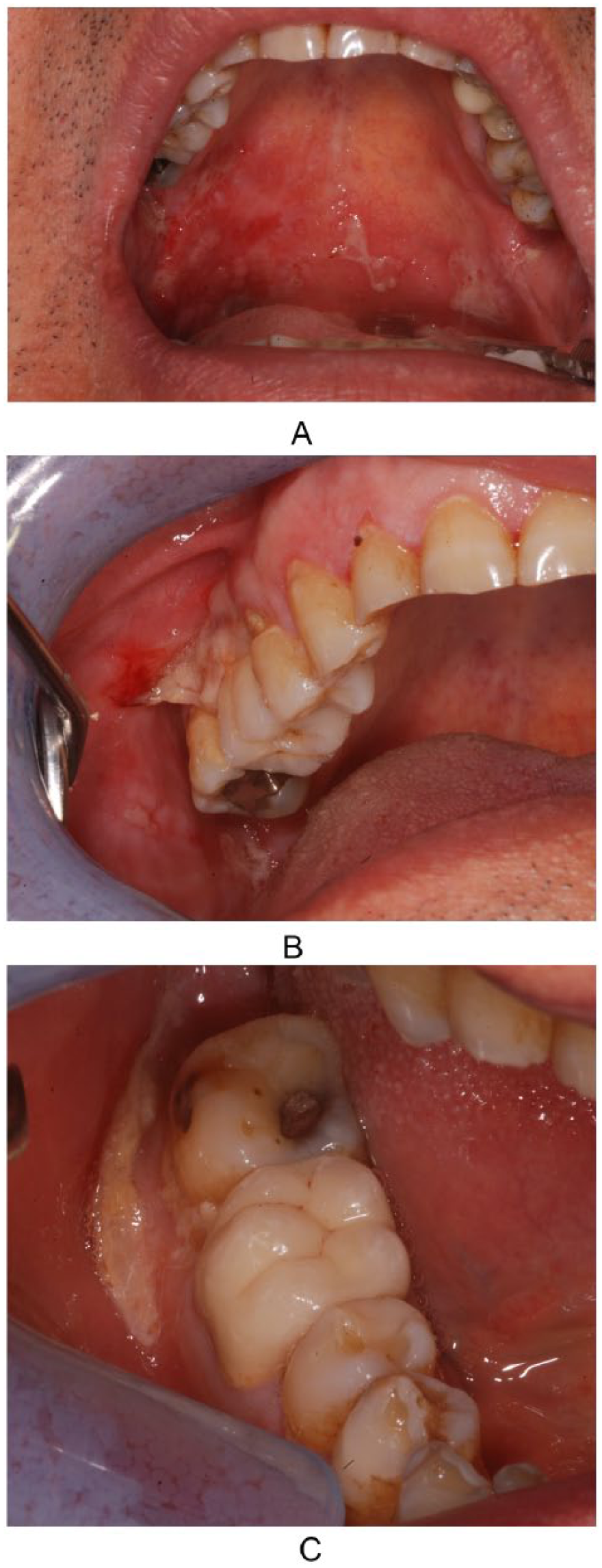
In May 2014, A 67-year-old man was referred to the Department of Biomedical and Neuromotor Sciences, Division of Oral Medicine, University of Bologna for a painful lesion in the soft palate. Intraoral examination revealed a bullous lesion and a small proliferative area localized in the soft palate (Figure 1). Nikoslky signs were negative and nothing noteworthy emerged from the patient’s medical and dental history. Two incisional biopsies were performed for histology and DIF, and pharmacological therapy with topical betamethasone (1 mg tablets 3 times a day) and prednisone 50 mg/d was initiated to alleviate symptoms. The diagnostic sample included the peripheral area of the bullous lesion and a portion of the proliferative area. In addition, a sample of healthy mucosa next to ulcerated lesion was taken for DIF. Histological examination of the proliferative area showed intraepithelial areas of acantholysis associated with high-grade dysplasia (Figure 2A and B). Immunoistochemical analysis revealed an increased expression of Ki67 in dysplastic area with respect to nondysplastic area (Figure 3). DIF revealed intercellular deposits of IgG and C3 (Figure 4). Histopathology and DIF were consistent for PV with histological signs of dysplasia. An OSCC or high-risk OPML could not be completely ruled out, so the dysplastic area in the soft palate was surgically resected 1 week after the start of cortisone therapy. Histological analysis of the excisional biopsy confirmed intraepithelial acantholysis but showed no sign of dysplasia. After surgery, the lesions worsened becoming larger and more painful (Figure 5A-C). Systemic pharmacological therapy was adjusted with prednisone (75 mg) and azathioprine (50 mg, 3 times a day) and regular follow-ups were scheduled. The patient’s clinical condition significantly improved with complete remission of the disease (Figure 6). At 23 months’ follow-up, prednisone was tapered to 6 mg/d still associated with azathioprine 50 mg, 3 times a day and the patient remains free from malignancies.

Oral bullous lesion with an adjacent small proliferative area localized in the right soft palate.
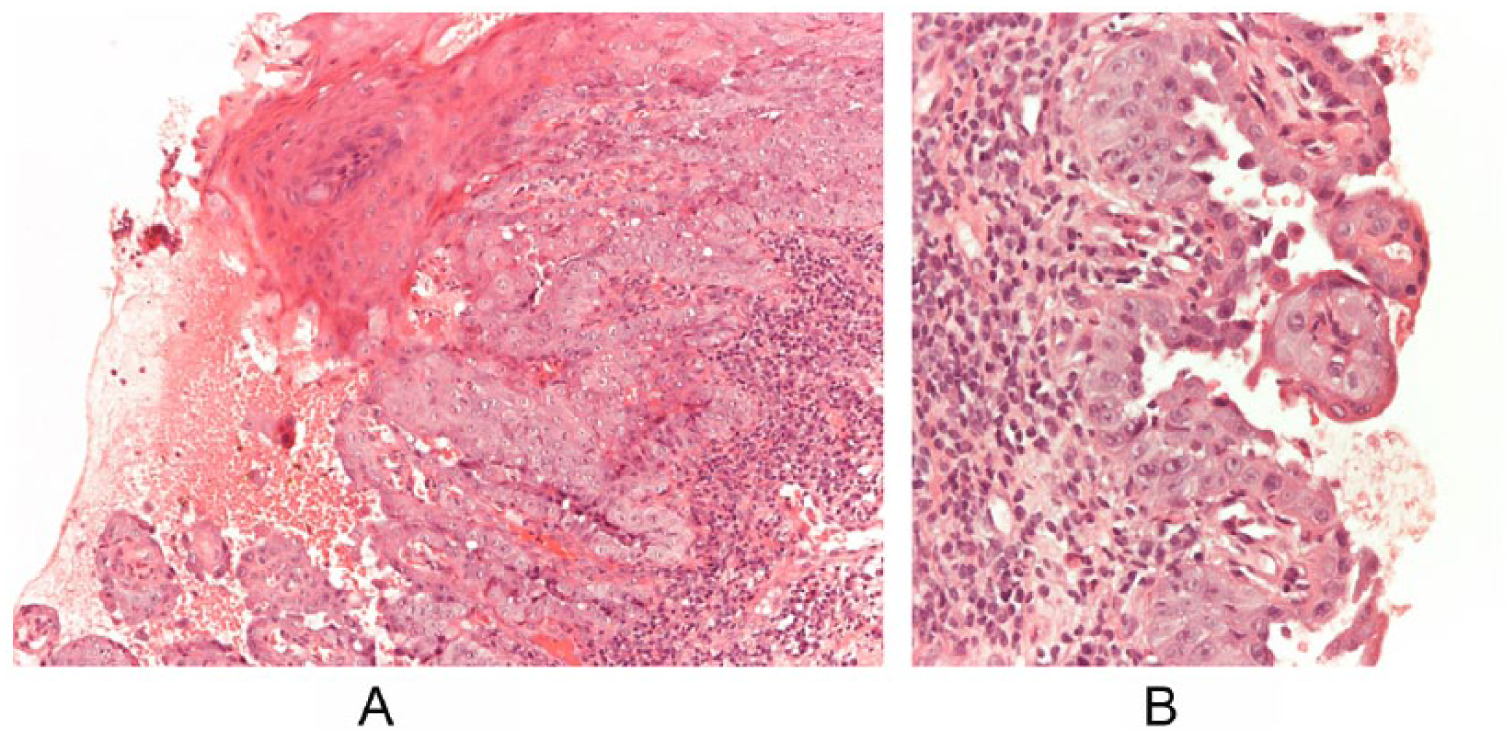
Histopathological analysis of the incisional biopsy shows acantholysis (A) and high-grade dysplasia (B).

Dysplastic epithelium presents increased expression of Ki-67 in basal, parabasal, and suprabasal layers compared with the adjacent nondysplastic mucosa (right).
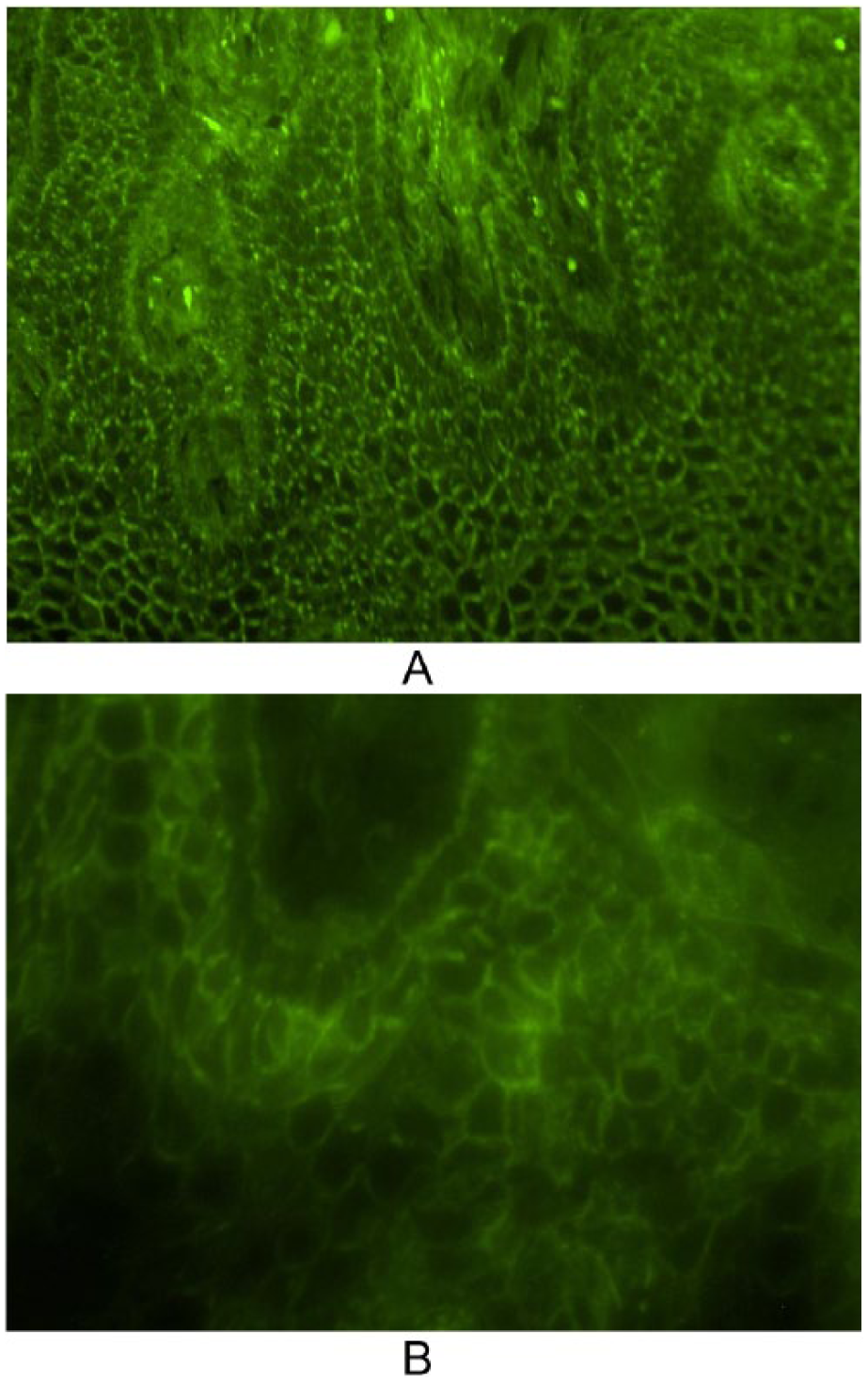
Direct immunofluorescence microscopy shows intercellular deposition of IgG (A) and C3 (B) in mucosa.
(A-C) Painful bullous lesions appeared in other sites of the oral cavity after surgery.

Clinical improvement after systemic therapy and 15 months of follow-up.
Discussion
Architectural and cytological changes in the oral cavity, generally referred to as epithelial dysplasia, are currently considered the strongest predictors of the future transformation of an oral potentially malignant lesion (OPML).
The 2005 World Health Organization classification of head and neck tumors divided the spectrum of dysplasia into 3 groups, mild, moderate, and high-grade dysplasia, depending on the number, type, and extension of architectural and cytological changes. 13 More recently, 6 internationally recognized experts and 3 pathologists from Ljubljana proposed a new dichotomic classification dividing lesions presenting epithelial dysplasia into low-grade (LG SIL) and high-grade (HG SIL) intraepithelial lesions. 14 Generally speaking, the more prominent and more numerous the architectural changes and cytological atypia are, the more severe the dysplasia. High-grade dysplasia or HG SIL is an important indicator of the risk status of an OPML.
Epithelial dysplasia in the oral cavity is usually identified in white/red lesions defined as OPMLs: leukoplakia and erythroplakia, whereas it is an uncommon histological finding in oral PV. PV is not classified as an OPML in the oral cavity but is considered a benign chronic autoimmune mucocutaneous disease. However, the correlation between malignancies and PV is a controversial literature topic. Some studies have reported an association between PV and malignancies of different histogenesis (lymphoma, thymoma, and leukemia).2,8-12 whereas a few reports have described OSCC arising in acantholytic bullous disease.15-17
PV is histologically characterized by rounded acantholytic cells with intensely eosinophilic cytoplasm, pyknotic nuclei, and perinuclear halos.1,3 A remarkable histological feature in the present case was the small neoproliferative area located near to the blistering disease. Incisional biopsy of this area disclosed high-grade dysplasia associated with a marker inflammatory infiltrate. However, the disappearance of neoproliferation after initial corticosteroid therapy and the histological findings of a second biopsy showing no signs of dysplasia and the follow-up period free from malignancies were all in favor of reactive rather than “truly” dysplastic cytological and architectural atypia. Several studies have emphasized that even inflammatory or reactive lesions may demonstrate features that are considered dysplastic, 18 one finding that 25% of benign lesions presented microscopic dysplastic features. 19 The distinction between “true dysplasia” and reactive mucosa in chronic inflammatory illnesses like bowel disease or Crohn’s disease, and gastroesophageal disease is currently considered a diagnostic problem in clinical practice.20,21 This is particularly true for features of low-grade dysplasia, where cellular hyperproliferation due to an inflammatory insult can be erroneously interpreted as cytological abnormalities. However, the present case showed severe architectural and cytological changes, and it is uncommon for aspects of high-grade dysplasia to be caused by a simple reactive process.
To the best of our knowledge, only one similar case has been reported in literature. Caltabiano et al 22 described a patient presenting whitish keratotic skin lesions suggestive of actinic keratosis who exhibited histological signs of moderate-to-severe dysplasia as well as classical PV histomorphology. The lesions completely regressed after steroid therapy, even if no histological evidence of the “disappearance” of epithelial dysplasia was reported. 22
In conclusion, a diagnosis of dysplasia or carcinoma in situ in patients with PV is a potential diagnostic challenge. Similar cases would benefit more from medical therapy instead of surgery and careful evaluation is necessary to institute the most appropriate treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.