
Abstract
Peritoneal metastasis in colorectal carcinoma is associated with a dismal prognosis; however, features that correlate with patterns of metastatic spread are not well characterized. We analyzed the clinicopathologic and molecular features of 166 patients with colorectal carcinomas stratified by metastases to the peritoneum or liver. Mucinous and signet ring cell differentiation were more frequently observed in colorectal carcinoma with peritoneal dissemination compared to colorectal carcinoma with liver metastasis (mucinous differentiation: 62% vs 23%, P < .001; signet ring cell differentiation: 21% vs 0%, P < .0001). The significant association of mucinous differentiation with peritoneal dissemination compared with liver metastasis was identified in patients with both synchronous and metachronous development of metastasis (P < .01). In contrast, colorectal carcinomas with liver metastasis were more frequently low-grade (90% vs 72%, P = .005) and associated with dirty necrosis (81% vs 56%, P = .001) compared with colorectal carcinomas with peritoneal dissemination. No significant differences were identified between colorectal carcinoma with peritoneal metastasis versus liver metastasis with respect to KRAS mutations, BRAF mutation, or high levels of microsatellite instability. Patients with tumors involving the peritoneum had a significantly worse overall survival in comparison to patients with liver metastasis lacking peritoneal involvement (P = .02). When including only those patients with peritoneal metastasis, the presence of any mucinous or signet ring cell differentiation was associated with a significantly worse overall survival (P = .006). Our findings indicate that mucinous and signet ring cell differentiation may be histologic features that are associated with an increased risk of peritoneal dissemination and poor overall survival in patients with peritoneal metastasis.
Introduction
Colorectal carcinoma is the third leading cause of cancer-related death in the United States. 1 Approximately 20% to 25% of patients present with distant metastasis, and patients who present with distant metastasis have an overall 5-year survival of 12.5%. 1 The most common site of distant metastasis is the liver, 2 but peritoneal metastasis affects 4% to 8% of patients with colorectal carcinoma at the time of diagnosis and subsequently develops in approximately 5% of patients during their disease course.3,4 Peritoneal metastasis in colorectal carcinoma has been traditionally considered to be a terminal condition with a median survival between 5 and 8 months,3,5,6 although improved survival has been reported with aggressive cytoreductive surgery and intraperitoneal chemotherapy in some centers.7-11 In contrast to peritoneal metastasis, improved patient survival is not uncommon in patients with liver metastasis, especially for those patients with resectable liver metastasis.12-15
Surprisingly little is known about the histologic differences between colorectal carcinomas that disseminate to the peritoneum and colorectal carcinomas that metastasize to the liver. A recent retrospective autopsy study identified mucinous and signet ring cell differentiation as being more frequently associated with peritoneal metastasis compared to liver metastasis, although systematic histopathologic analysis was not performed. 16 Certain subtypes of colorectal carcinoma, such as signet ring cell carcinoma, have been reported to have a high association with peritoneal dissemination17-21 compared to liver metastasis, but not all studies have confirmed this association. 22 In addition, the molecular differences such as mutations in KRAS and BRAF as well as differences in microsatellite instability between colorectal carcinoma with peritoneal versus liver metastasis have not been specifically studied. Given the poor prognostic significance of peritoneal metastasis in colorectal carcinoma, identification of histologic and molecular features associated with a high risk of peritoneal metastasis would be of potential benefit.
In this study, we analyzed the clinicopathologic features of 166 patients with colorectal carcinomas stratified by metastases to the peritoneum or liver in order to (1) compare tumor morphology within these 2 patient groups with different metastatic patterns, (2) correlate molecular alterations with tumor histology and metastatic pattern, and (3) evaluate the prognostic differences between peritoneal and liver metastasis and identify which histologic features, if any, affect patient survival. In so doing, we demonstrate that mucinous and signet ring cell differentiation is more commonly identified in colorectal carcinoma with peritoneal metastasis compared with liver metastasis and among patients with peritoneal metastasis mucinous or signet ring cell differentiation is associated with a worse prognosis.
Methods
Study Groups
The clinicopathologic records of 78 patients with resected primary colorectal carcinoma with synchronous (n = 60) or metachronous (n = 18) metastasis to the peritoneum were consecutively identified and reviewed at the Department of Pathology, University of Pittsburgh Medical Center, for the years 2005 through 2012. The clinicopathologic records of 88 patients with resected primary colorectal carcinoma with synchronous (n = 65) or metachronous (n = 23) metastasis to the liver were consecutively identified and reviewed at the Department of Pathology, University of Pittsburgh Medical Center, for the years 2009 through 2012. All cases had pathologic confirmation of the primary colorectal adenocarcinoma and metastasis. To be included in the metachronous metastasis group, a patient was required (1) to have no clinical evidence of metastatic disease at the time of presentation by either intraoperative assessment or radiologic imaging studies and (2) develop biopsy-confirmed metastatic disease at least 6 months following the initial surgical resection. The pathology reports and hospital charts were reviewed and the following information was obtained: type of surgical procedure, extent of disease at presentation, age, gender, administration of neoadjuvant therapy, tumor size, and tumor location. Demographic and intraoperative data were obtained from hospital and clinic charts under the guidelines of the University of Pittsburgh Institutional Review Board (IRB# PR012020335).
Pathologic Evaluation
All slides from the resected primary and metastatic tumor were reviewed by 2 pathologists (RKP and TRK). For tumors less than 3 cm in size, the entire tumor was submitted for histologic review. For tumors greater than 3 cm in size, at least 3 sections of tumor demonstrating deepest extent of invasion and 2 sections of tumor and adjacent mucosa were submitted. The following histologic features were recorded for each case: grade, extent of invasion using the American Joint Committee on Cancer classification system, 23 angiolymphatic invasion, perineural invasion, signet ring cell differentiation, mucinous differentiation, tumor budding, and dirty necrosis. The percentage of tumor with signet ring cell and mucinous differentiation was also separately recorded. For mucinous adenocarcinoma, 2-tiered grading system (low grade vs high grade) based on the percentage of gland formation in each tumor as advocated by the World Health Organization (WHO) for conventional colorectal carcinoma was used. 24 By definition, a carcinoma with signet ring cell differentiation was labeled high grade. Mucinous differentiation was defined as areas of extracellular mucin associated with tumor cells. Tumor budding was defined as isolated cells or groups of 5 or less detached tumor cells at the invasive front of the tumor. At least 5 different locations of the invasive front of each tumor were examined using 20× objective magnification. Cases with ≥10 tumor buds in a single 20× objective field (0.95 mm2) were considered to have high tumor budding. 25 Visceral peritoneal involvement was defined as presence of tumor on the serosal surface associated with adjacent tissue reaction in the form of inflammation and/or mesothelial hyperplasia. Dirty necrosis was defined as nuclear and cellular debris associated with the carcinoma. The presence of dirty necrosis was assessed at low-power (2× or 4× objective) magnification, and a tumor was labeled as demonstrating dirty necrosis if greater than 25% of the tumor was associated with dirty necrosis.
DNA Mismatch Repair Protein Immunohistochemical Analysis and Microsatellite Instability Analysis Polymerase Chain Reaction
Mismatch repair protein immunohistochemistry was performed using primary monoclonal antibodies against MLH1 (clone G168-728, Ventana, Tucson, AZ), MSH2 (clone G219-1129, Ventana), MSH6 (clone 44, BD Transduction, San Jose, CA), and PMS2 (A16-4, Cell Marque, Rocklin, CA). All antibodies were applied to 4-µm-thick formalin-fixed, paraffin-embedded sections. The sections were deparaffinized in xylene and rehydrated through graded alcohols to distilled water before undergoing antigen retrieval by heat treatment using either Ventana CC1 buffer solution (MSH2 and MSH6) or Ventana CC2 buffer solution (MLH1 and PMS2). Automated detection using the Ventana Benchmark Ultra staining system and Ventana UltraView detection was used. Normal expression was defined as nuclear staining within tumor cells, using infiltrating lymphocytes as positive internal control. Negative loss of protein expression was defined as complete absence of nuclear staining within tumor cells with concurrent positive labeling in internal nonneoplastic tissues.
For a subset of tumor, tumor targets were manually microdissected from 4-µm unstained histologic sections using corresponding hematoxylin and eosin–stained slides as guidance. DNA was extracted from paraffin sections, using the DNeasy tissue kit (Qiagen, Valencia, CA), according to the manufacturer’s instructions. Detection of microsatellite instability (MSI) was performed using a National Cancer Institute (NCI)–recommended panel of microsatellite markers (BAT25, BAT26, D2S123, D5S346, and D17S250) as well as one novel quasi-monomorphic mononucleotide marker CAT25. 26 Based on established criteria, if 0 of 6 (0%) markers show instability, the tumor is classified as microsatellite stable (MSS). If 2/6 (≥30%) or more markers show instability by polymerase chain reaction (PCR), the tumor is classified as high-level MSI (MSI-H).
Tumors with loss of expression of any MMR protein or with MSI-H by PCR analysis were labeled as MMR protein deficient. Tumors with preserved expression of all 4 MMR proteins and/or microsatellite stable by PCR analysis were labeled as MMR protein proficient.
BRAF Mutation Analysis
Tumor targets were manually microdissected from 4-µm unstained histologic sections. DNA was extracted from paraffin sections, using the DNeasy tissue kit (Qiagen, Valencia, CA), according to the manufacturer’s instructions. Detection of BRAF mutations was performed using real-time PCR and post-PCR fluorescence melting curve analysis (FMCA) on LightCycler (Roche Applied Science, Indianapolis, IN), as previously described. 27 This assay detects BRAF mutations in codons 599, 600, and 601.
KRAS Mutational Analysis
Tumor targets were manually microdissected from 4-µm unstained histologic sections using the original hematoxylin and eosin–stained slide as a guide. DNA was isolated from each target using the DNeasy kit (Qiagen, Valencia, CA), according to the manufacturer’s instructions. DNA was amplified with primers flanking exon 2 of the KRAS gene (forward primer 5′-GGT GAG TTT GTA TTA AAA GGT ACT GG-3′ and reverse primer 5′-TCC TGC ACC AGT AAT ATG CA-3′). PCR products were sequenced in both sense and antisense directions using the BigDye Terminator v3.1 cycle sequencing kit on an ABI 3130 (Applied Biosystems, Inc, Foster City, CA), according to the manufacturer’s instructions. The sequences were analyzed using Mutation Surveyor software (SoftGenetics, LLC, State College, PA). Each case was classified as positive or negative for KRAS mutation based on the sequencing results.
Statistical Analysis
Chi-square or Fisher exact tests were used to characterize the relationship between categorical variables, as appropriate. The endpoints selected for survival analysis were overall survival defined as the time (measured in months) from the date of initial diagnosis to the date of death and censored at the date of last clinical follow-up. For colorectal carcinoma with metachronous development of metastatic disease, time to metastasis (measured in months) was also selected and was defined as the time from the initial surgical resection of the primary carcinoma to the first documented evidence of the development of metastatic disease. Survival rates were determined by the Kaplan-Meier method, and differences between groups were evaluated by log-rank test. Hazard ratios were calculated from a Cox proportional hazard model to identify individual predictors of survival. Multivariate analysis of significant or borderline individual risk factors (P < .2) was performed using Cox proportional hazard regression to identify independent risk factors for survival. All statistics were assessed using 2-sided tests with P values <.05 considered statistically significant. Statistical analyses were performed using SPSS (for Windows 12.0, SPSS Inc, Chicago, IL).
Results
Clinical Features of Study Group Patients
A total of 166 cases with metastasis were analyzed including 78 colorectal carcinomas with peritoneal dissemination and 88 colorectal carcinomas with liver metastasis. Thirteen patients with colorectal carcinoma demonstrated both synchronous peritoneal and liver metastasis; all 13 cases had a predominant involvement of the peritoneum and were included in the group of patients with peritoneal metastasis in the analysis. None of the patients included in the colorectal carcinoma with liver metastasis group had concurrent peritoneal dissemination at presentation. Most patients with synchronous peritoneal metastasis (36/60, 60%) were treated with cytoreductive surgery with hyperthermic intraperitoneal chemoperfusion, as previously described, 10 with the remainder (24/60, 40%) treated with systemic chemotherapy alone. Most patients with synchronous liver metastasis (37/65, 57%) underwent surgical resection of their liver metastases. All 18 patients with metachronous development of peritoneal metastasis lacked concurrent liver metastasis and were treated with cytoreductive surgery with hyperthermic intraperitoneal chemoperfusion. Seventeen of 23 (74%) patients with metachronous development of liver metastasis were treated with resection of the liver metastasis with the remainder undergoing biopsy only.
The clinicopathologic features of the study group colorectal carcinomas stratified by metastasis pattern are further detailed in Table 1. Colorectal carcinoma with peritoneal dissemination was more common in women compared with colorectal carcinoma with liver metastasis (55% vs 39%, P = .04) and had a trend to preferentially occur in younger patients (mean age 57 vs 62 years, P = .07). Colorectal carcinoma with peritoneal dissemination was more frequently primary to the right colon compared with colorectal carcinoma with liver metastasis (49% vs 34%, P = .01).
Clinicopathologic Features of Colorectal Carcinomas Stratified by Metastasis Pattern.
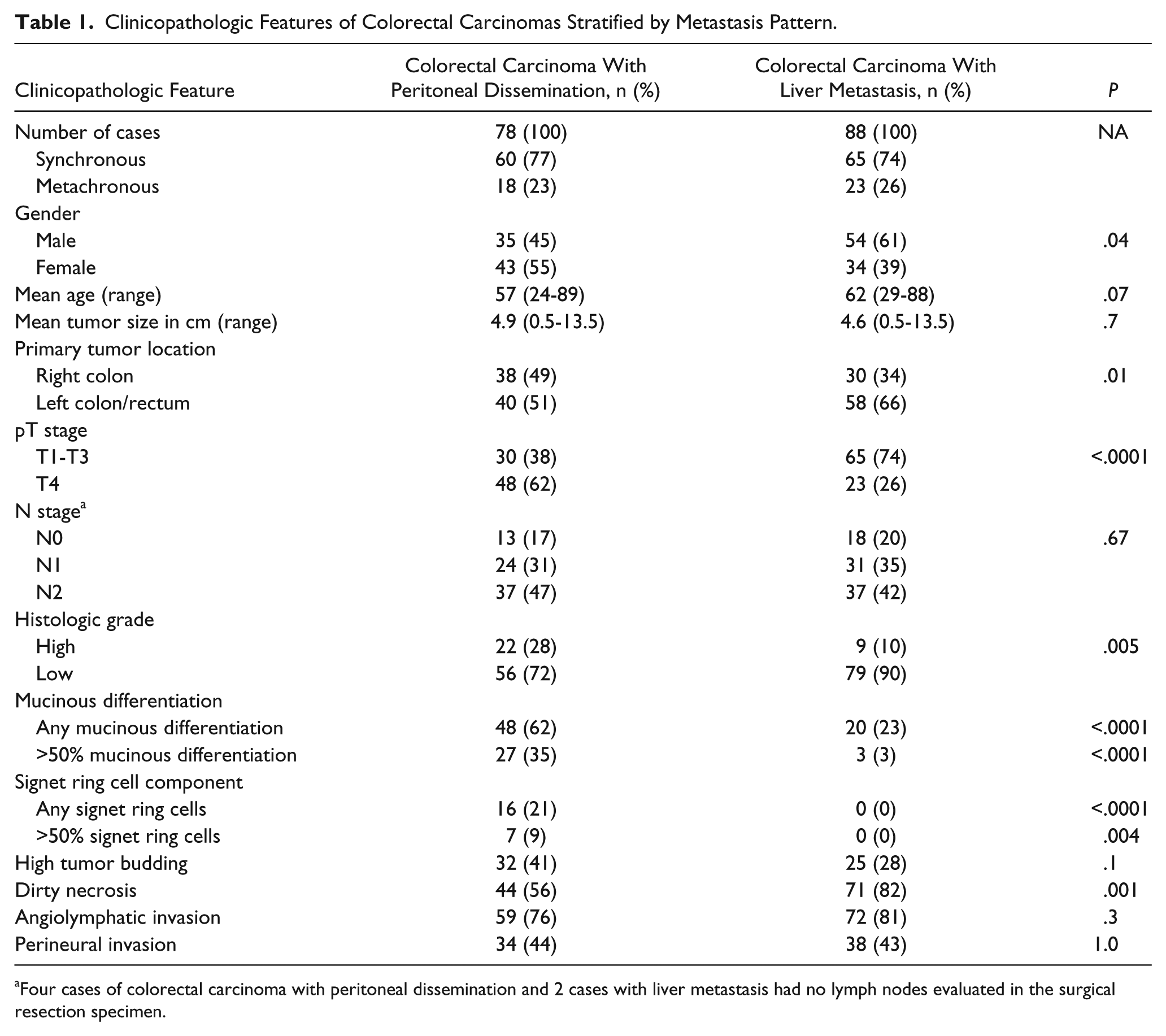
Four cases of colorectal carcinoma with peritoneal dissemination and 2 cases with liver metastasis had no lymph nodes evaluated in the surgical resection specimen.
Pathologic Features of Colorectal Carcinomas Stratified by Metastatic Pattern: Mucinous and Signet Ring Cell Differentiation Are Associated With Peritoneal Dissemination
Colorectal carcinomas with peritoneal dissemination demonstrated different morphologic features compared to colorectal carcinomas with liver metastasis (Table 1). Any degree of mucinous differentiation was more frequently observed in colorectal carcinoma with peritoneal dissemination compared to colorectal carcinoma with liver metastasis (62% vs 23%, P < .0001). Colorectal carcinoma with peritoneal dissemination was also more frequently composed of abundant extracellular mucin comprising >50% of the tumor volume satisfying WHO criteria for mucinous adenocarcinoma compared with colorectal carcinoma with liver metastasis (35% vs 3%, P < .0001). The significant association of mucinous differentiation with peritoneal dissemination compared with liver metastasis was identified in both the synchronous and metachronous metastasis subgroups (both with P < .01). Patients with colorectal carcinoma with synchronous peritoneal dissemination received neoadjuvant chemotherapy therapy less frequently compared with patients with colorectal carcinoma with synchronous liver metastasis (25% vs 51%, P = .005). Therefore, therapy-induced changes cannot explain the difference in mucinous differentiation observed among these 2 groups.
Signet ring cell differentiation was identified in 21% of colorectal carcinoma with peritoneal dissemination, with 9% of cases being composed of >50% signet ring cells satisfying WHO criteria for signet ring cell carcinoma (Figure 1). None of the 88 colorectal carcinomas with liver metastasis displayed any signet ring cell features (P < .0001). A significant association of signet ring cell differentiation with peritoneal dissemination compared with liver metastasis was identified in the subgroup of patients with synchronous metastasis (23% vs 0%, P < .001). Within the metachronous subgroup, 2 of 18 (11%) colorectal carcinomas with metachronous development of peritoneal dissemination demonstrated signet ring cell differentiation compared with none of the colorectal carcinoma with metachronous liver metastasis (0/23, 0%). However, this difference did not reach statistical significance given the low numbers of cases in each subgroup (P = .2).
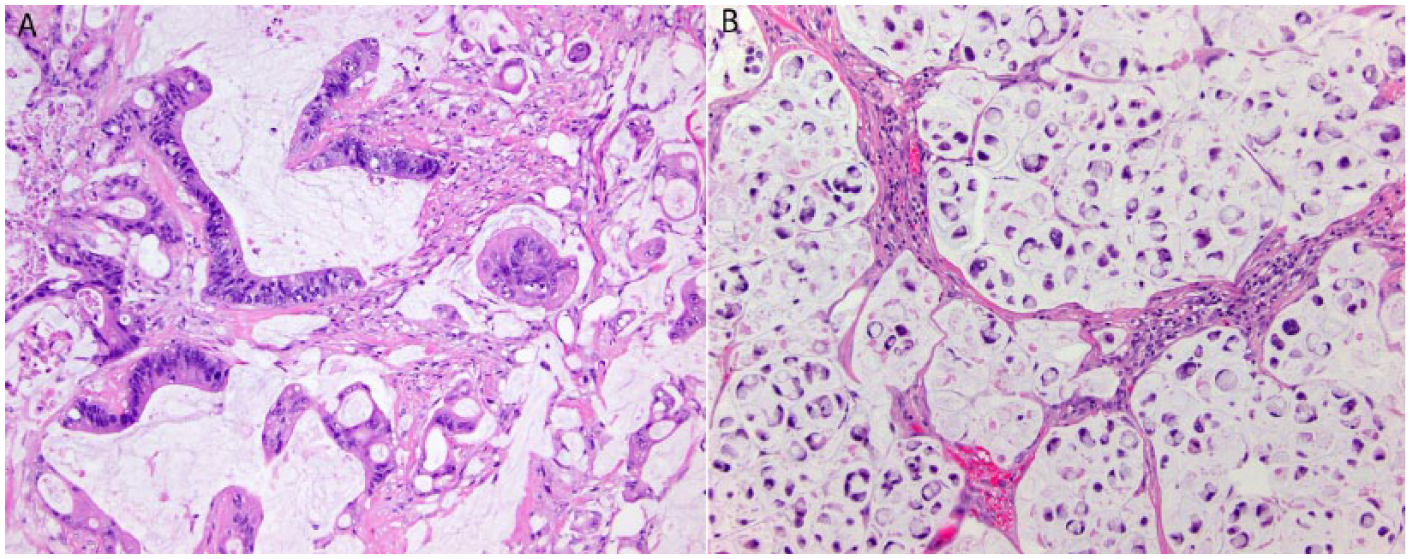
(A) Primary mucinous adenocarcinoma of the colon (100×) that demonstrated peritoneal metastasis. (B) Primary signet ring cell adenocarcinoma of the colon (200×) that demonstrated peritoneal metastasis.
Colorectal carcinomas with liver metastasis were more frequently low grade and associated with dirty necrosis compared with colorectal carcinomas with peritoneal dissemination (low grade: 90% vs 72%, P = .005; dirty necrosis: 81% vs 56%, P = .001). As expected, colorectal carcinoma with peritoneal dissemination more frequently demonstrated visceral peritoneal penetration corresponding to a pT4 designation compared with colorectal carcinoma with synchronous liver metastasis (62% vs 26%, P < .0001). There was no significant difference between colorectal carcinomas with peritoneal dissemination and colorectal carcinomas with liver metastasis with respect to tumor budding, angiolymphatic invasion, perineural invasion, and venous invasion (all with P > .05).
Molecular Features: Similar KRAS and BRAF Mutation Rates and Microsatellite Instability Status in Patients With Peritoneal and Liver Metastasis
Of the 134 cases tested, KRAS exon 2 and 3 mutations were identified in 54 tumors (40%; Table 2). No significant difference in KRAS mutations were identified between colorectal carcinomas with peritoneal dissemination and colorectal carcinomas with liver metastasis (33% vs 45%, P = .21). Similarly, within the synchronous and metachronous subgroups, no differences in KRAS mutation status was identified between those tumors with peritoneal dissemination and those tumors with liver metastasis (P > .05). There was no association with KRAS mutation status and any of the histologic features assessed.
Molecular Features of Colorectal Carcinomas Stratified by Metastasis Pattern.

Abbreviations: MMR, mismatch repair; PCR, polymerase chain reaction.
Tumors with loss of expression of any MMR protein or with MSI-H by PCR analysis were labeled as MMR protein deficient. Tumors with preserved expression of all 4 MMR proteins and/or microsatellite stable by PCR analysis were labeled as MMR protein proficient.
Of the 114 cases tested, BRAF V600E mutations were identified in 12 tumors (11%; Table 2). No BRAF codon 599 or 601 mutations were identified. No significant difference in BRAF V600E mutation was identified between colorectal carcinomas with peritoneal dissemination and colorectal carcinomas with liver metastasis (15% vs 7%, P = .2). Similarly, within the synchronous and metachronous subgroups, no differences in BRAF mutation status was identified between those tumors with peritoneal dissemination and those tumors with liver metastasis (P > .05). There was no association with BRAF mutation status and any of the histologic features assessed.
Finally, of the 137 cases evaluated for DNA mismatch repair protein abnormalities by either MSI PCR or DNA mismatch repair protein immunohistochemistry, mismatch repair protein deficiency was identified in 11 tumors (8%) with no significant difference identified between colorectal carcinoma with peritoneal dissemination and colorectal carcinoma with liver metastasis (7% vs 9%, P = .8; Table 2). Of the 11 patients with mismatch repair protein deficient tumors, 3 patients were subsequently diagnosed as having Lynch syndrome and the remaining 8 patients were diagnosed as having sporadic mismatch repair protein deficient tumors given the presence of concurrent BRAF V600E mutations in their tumors. There was no association with mismatch repair protein status and any of the histologic features assessed.
Analysis of Clinical Outcome: Peritoneal Metastasis With Mucinous or Signet Ring Cell Differentiation Is a Predictor of Worse Overall Survival
A total of 164 patients (98%) had clinical follow-up with a median follow-up interval of 21 months (range = 1-129 months). Among the study patients, there were 63 deaths occurring between 1 month and 68 months from the time of initial diagnosis.
Using Kaplan-Meier survival functions, patients with tumors involving the peritoneum had a significantly worse overall survival in comparison to patients with liver metastasis lacking peritoneal involvement (log-rank P = .02; Figure 2). When including only those patients with peritoneal metastasis, the presence of any mucinous or signet ring cell differentiation was associated with a significantly worse overall survival (log-rank P = .006; Figure 2). There was no difference in overall survival between those patients with metachronous versus synchronous metastasis for the patient group with peritoneal metastasis (P > .05). However, patients with synchronous liver metastasis had a significantly worse overall survival compared to patients with metachronous development of liver metastasis (P = .03). Finally, there was no significant difference in the time to development of metachronous metastatic disease between the patients in the peritoneal and liver metastasis groups (P > .05).

(A) Kaplan-Meier survival curves comparing overall survival of patients with colorectal carcinoma with peritoneal versus liver metastasis. Patients with peritoneal metastasis had a statistically worse overall survival compared with patients with liver metastasis (log-rank P = .02). (B) Kaplan-Meier survival curves comparing overall survival of patients with peritoneal metastasis stratified by tumor histology. Patients with tumor harboring either mucinous or signet ring cell differentiation had a statistically worse overall survival compared with patients with non–mucinous/non–signet ring cell histology (P = .006).
Factors associated with poor overall survival using Cox proportional hazards univariate analysis included peritoneal tumor dissemination (P = .02), high tumor grade (P = .001), perineural invasion (P = .03), and female gender (P = .001; Table 3). Mucinous histology, signet ring cell histology, angiolymphatic invasion, and lymph node involvement had borderline associations with poor overall survival. In the multivariable analysis that included variables with at least borderline association with survival (P < .2) from the univariate analysis, the only factors associated with poor survival were patient age (P = .03) and high tumor grade (P = .01). Peritoneal tumor metastasis had a borderline association with poor survival in the multivariable analysis, but this did not reach statistical significance (P = .1).
Univariate and Multivariate Analysis of Overall Survival of All Study Patients According to Clinical, Histologic, and Molecular Features.
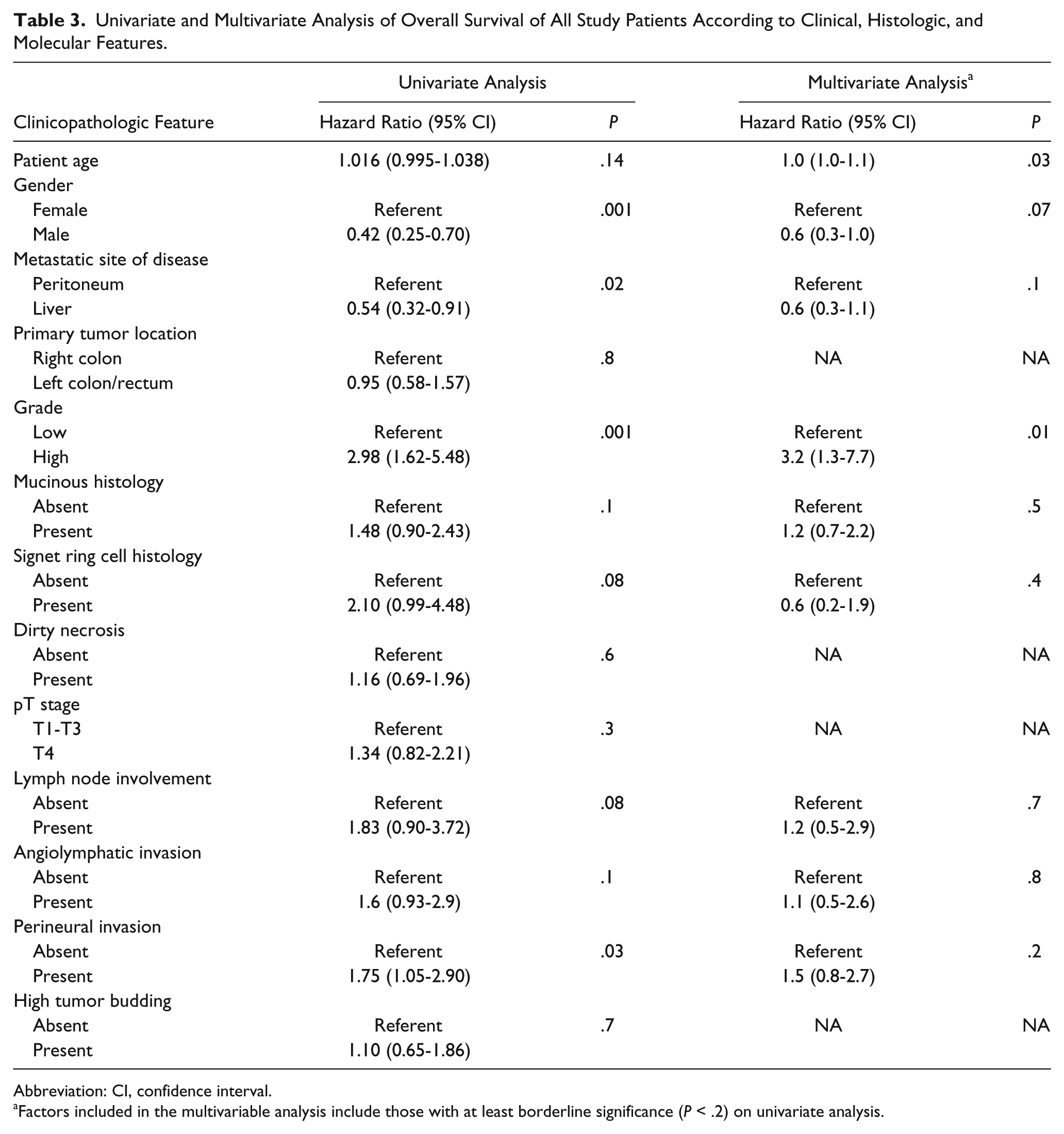
Abbreviation: CI, confidence interval.
Factors included in the multivariable analysis include those with at least borderline significance (P < .2) on univariate analysis.
As not all tumors in our study group were analyzed for molecular abnormalities, we separately evaluated the association of molecular factors with overall survival. Neither KRAS mutation status nor MSI status were significantly associated with overall survival (both with P > .05), although positive BRAF mutation had a borderline association with poor overall survival (P = .06).
Discussion
The primary motivation for this study was to identify the morphologic features in colorectal carcinoma that correlate with patterns of distant metastatic spread. We demonstrate that pathologic features are significantly associated with patterns of metastatic spread in colorectal carcinoma in both the synchronous and metachronous settings. Colorectal carcinoma that develops peritoneal metastasis frequently displays mucinous and signet ring cell differentiation and high-grade differentiation and more frequently originates in the right colon. In contrast, colorectal carcinoma that develops liver metastasis is frequently low grade, lacks mucinous and/or signet ring cell differentiation, displays characteristic “dirty” necrosis, and more often is primary to the left colon/rectum. These findings suggest that mucinous and signet ring cell differentiation may be histologic features in colorectal carcinoma, which are associated with an increased risk of development of peritoneal dissemination. Our analysis also confirms previous literature data that have found that patients with peritoneal dissemination of colorectal carcinoma have a worse overall survival compared with patients with liver metastasis. We expand on these previous literature reports and demonstrate that patients with colorectal carcinoma with peritoneal metastasis that harbor carcinomas with either mucinous or signet ring cell morphology have worse survival compared to those patients with nonmucinous, non–signet ring cell histology.
Mucinous adenocarcinomas of the colon and rectum are relatively common and account for between 4% and 19% of colorectal adenocarcinomas, although incidence rates appear to differ worldwide.28-33 Most studies have found no association between mucinous adenocarcinoma and patient survival,29,34-36 although some studies have found mucinous differentiation to be an indicator of poor prognosis.36,37 Our results indicate that patients with peritoneal dissemination of colorectal carcinoma more often have adenocarcinomas with mucinous differentiation with 35% meeting WHO criteria for a diagnosis of mucinous adenocarcinoma. In a large population-based study, Lemmens and colleagues analyzed colorectal carcinomas with synchronous peritoneal metastasis found that 27% were mucinous adenocarcinomas. 32 Of particular interest, in our analysis of patients who developed metachronous peritoneal metastasis after initial curative resection of their colorectal carcinoma, mucinous differentiation was identified in large proportion (67%) of primary tumors that subsequently developed peritoneal metastasis. Similarly, van Gestel et al patients with a primary mucinous adenocarcinoma were at increased risk of developing metachronous peritoneal metastasis. 38 Finally, among those patients with peritoneal metastasis, patients with mucinous tumor histology had a significantly worse survival compared with patients with nonmucinous, non–signet ring cell tumor histology. Our findings indicate that mucinous histology in the metastatic setting is associated with worse survival.
Signet ring cell carcinoma of the colon and rectum is relatively rare and accounts for between 0.1% and 1.1% of colorectal adenocarcinomas. 19 Signet ring cell differentiation is a well-established factor associated with poor patient survival.19,21,22,39,40 Most but not all studies have identified a high frequency of peritoneal metastasis for patients with signet ring cell carcinoma. Tung and colleagues found a high rate of peritoneal seeding (35.7%) and a low rate of liver metastasis (14.3%) for signet ring cell carcinoma compared to conventional colorectal adenocarcinoma. 21 Similarly, Psathakis and colleagues 17 found higher incidence of peritoneal tumor spread (64.3%) and a lower incidence of hepatic metastasis (14.3%) when compared to non–signet ring cell colorectal carcinoma. In contrast, Nissan et al found a similar proportion of patients with signet ring cell carcinoma that presented with peritoneal metastasis compared with liver metastasis. 22 Our results confirm the conclusions of most previous studies and demonstrate that signet ring cell differentiation is more often associated with peritoneal metastasis compared with liver metastasis. Many of these previous analyses did not perform detailed histologic review of the cases included in their analysis. Our data indicate that colorectal carcinoma with peritoneal metastasis frequently display a signet ring cell component that may not meet the WHO diagnostic threshold for signet ring cell carcinoma and that the presence of any signet ring cell differentiation within a colorectal carcinoma with peritoneal dissemination is associated with worse overall survival.
Correlation of patterns of metastasis in colorectal carcinoma with molecular alterations has not been previously studied to our knowledge. Mismatch repair protein deficiency is well known to be associated with mucinous and signet ring cell differentiation, and one would expect an increase in the incidence of mismatch repair protein deficiency in cases of peritoneal dissemination as they are enriched for carcinomas with mucinous and signet ring cell components. However, our results show similar frequency of mismatch repair protein deficiency for carcinomas regardless of pattern of spread. In addition, there was no difference in frequency of mismatch repair protein deficiency between those tumors with mucinous and/or signet ring cell differentiation and those tumors with nonmucinous/non–signet ring cell histology in our study. We have previously shown that BRAF-mutated colorectal adenocarcinoma is an aggressive adenocarcinoma with frequent mucinous differentiation and metastasis at presentation 41 ; however, we did not identify any significant association between BRAF mutation and pattern of metastasis or tumor histology in our current analysis. Similarly, KRAS mutation status did not correlate with tumor histology or pattern of metastatic spread. Further study is necessary to determine which molecular factors, if any, are associated with peritoneal dissemination compared with liver metastasis of colorectal carcinoma. In addition, the reasons why colorectal carcinoma with mucinous and/or signet ring cell differentiation has a propensity to metastasize to the peritoneum remain to be discovered.
Our study has limitations, including the retrospective design, the size of the study cohort, and the inherent issue of lack of rigorously standardized treatment and follow-up in retrospective analyses. Most but not all patients with peritoneal metastasis received cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion. Similarly, most patients with liver metastasis underwent surgical resection of their liver metastasis but some were treated with systemic chemotherapy alone. We were also not able to control for postoperative chemotherapy treatment. Although not a large study by some standards, our analysis is one of the largest studies to date requiring rigorous re-review of tumor histology and correlation of patterns of metastasis in colorectal carcinoma with morphologic and molecular factors.
In conclusion, colorectal carcinoma with peritoneal metastasis demonstrates distinctly different tumor morphology with frequent mucinous and signet ring cell differentiation and high tumor grade compared to colorectal carcinoma with liver metastasis. The association of mucinous and signet ring cell differentiation and peritoneal metastasis suggests that mucinous and signet ring cell histology may represent a high-risk histologic feature for the development of peritoneal dissemination. Indeed, mucinous and signet ring cell differentiation were often identified in the primary adenocarcinomas in patients who developed metachronous peritoneal metastasis after initial curative resection of their colorectal carcinoma. We confirm that patients with peritoneal dissemination of colorectal carcinoma have a worse overall survival compared with patients with liver metastasis and identify mucinous or signet ring cell morphology as poor prognostic factors in patients with peritoneal metastasis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.