
Abstract
Subareolar sclerosing duct hyperplasia (SSDH) remains to be fully characterized nearly 20 years after initial description. Thirty-five SSDH cases diagnosed over a 16-year period (January 2000 to December 2015) were reviewed. All patients were female (mean age = 59 years, range = 18-80) who had presented with a unilateral solitary lesion (left 22, right 13) with a mean size of 1.3 cm (range = 0.4-3.0 cm), and showed florid and papillary epithelial hyperplasia with dense sclerosis without involvement of nipple or areolar epidermis. Significant lesions concurrent within SSDH included low-grade adenosquamous carcinoma (n = 1), ductal carcinoma in situ (DCIS; n = 1), lobular carcinoma in situ (LCIS; n = 1), and atypical ductal hyperplasia (ADH; n = 13). No case of SSDH recurred in a mean follow-up of 44 months (range = 6-189). Subsequent significant lesions occurred in 6 patients: DCIS (n = 3; ipsilateral 2, contralateral 1), ipsilateral ADH (n = 2), and ipsilateral atypical lobular hyperplasia (n = 1). Long-term follow-up for patients with SSDH is indicated as DCIS can occur subsequently in either breast.
Introduction
Complex sclerosing papillary hyperplastic lesions (CSPHL) are relatively common in the breast. Most such lesions show florid epithelial hyperplasia with a dominant papillary architectural growth pattern amid a densely sclerotic stroma. Some types of CSPHL are histologically distinctive and have been well characterized—for example, radial scar and florid papillomatosis of nipple. Some such lesions display lesser degree of sclerosis (eg, juvenile papillomatosis). Several diagnostic terms have been invoked for related lesions, some of which may be rather generic, such as “sclerosing papilloma,” “complex sclerosing papilloma,” and “ductal papillomatosis.” Other purportedly characteristic lesions that could be considered in the differential diagnosis of CSPHL include “infiltrating epitheliosis,” 1 “indurative mastopathy,” 2 “nonencapsulated sclerosing lesion,” 3 and “sclerosing papillary proliferation.” 4
A distinct type of CSPHL located in the subareolar region of the breast, with neither nipple nor areolar involvement, had been described by Rosen in 1987 as “subareolar sclerosing duct hyperplasia” (SSDH). 5 The lesion has also been referred to as “subareolar papillomatosis.” 6 Since then, only one published case series of SSDH (in the Spanish literature) has been published. 7 As stated in its original description, 5 SSDH differs sufficiently from other sclerosing papillary hyperplastic lesions to warrant a specific diagnosis.
Herein, we describe 35 additional cases of SSDH. Our study was intended to further characterize this distinctive clinicopathological entity—which remains not only underrecognized but is also commonly confused with the spatially and morphologically related lesion of florid papillomatosis of nipple and other CSPHL.
Materials and Methods
The electronic records of the Department of Pathology at New York Presbyterian Hospital-Weill Cornell Medical Center were examined for cases of SSDH. The search encompassed a 16-year period (January 2000 to December 2015) and included cases received for consultative opinion as well as those diagnosed on in-house material. Twenty-seven of the 35 cases had been diagnosed by Dr Paul Peter Rosen (author of the original paper on SSDH). All available clinical and pathological material for each case diagnosed with SSDH were retrieved and reviewed. The reviewed histopathological material comprised routinely processed and prepared hematoxylin-eosin–stained slides, as well as routinely prepared immunohistochemical preparations in some cases. The diagnosis of SSDH was confirmed for each case. Follow-up information was obtained, wherever possible, from treating physicians. This study was conducted under an institutional review board–approved protocol.
Results
Thirty-five cases of SSDH were included in the study. Thirty of the 35 cases had been received in consultative second opinion. All patients were female (age range = 18-80 years, mean = 59) with a unilateral solitary lesion (left = 22, right = 13; Figure 1). Thirty-one of 35 (88%) patients presented with a palpable mass, 3 (8%) with a mammographic abnormality, and 1 (3%) with nipple discharge. No patient had a bilateral lesion. The clinical impression, at the time of excision (as stated in the specimen requisition), was either “papillary lesion” or “papilloma” in 34 cases. Although Paget disease was stated as the clinical diagnosis in one case, no carcinoma was identified either in the corresponding SSDH lesion or in the overlying nipple or areola on excision.
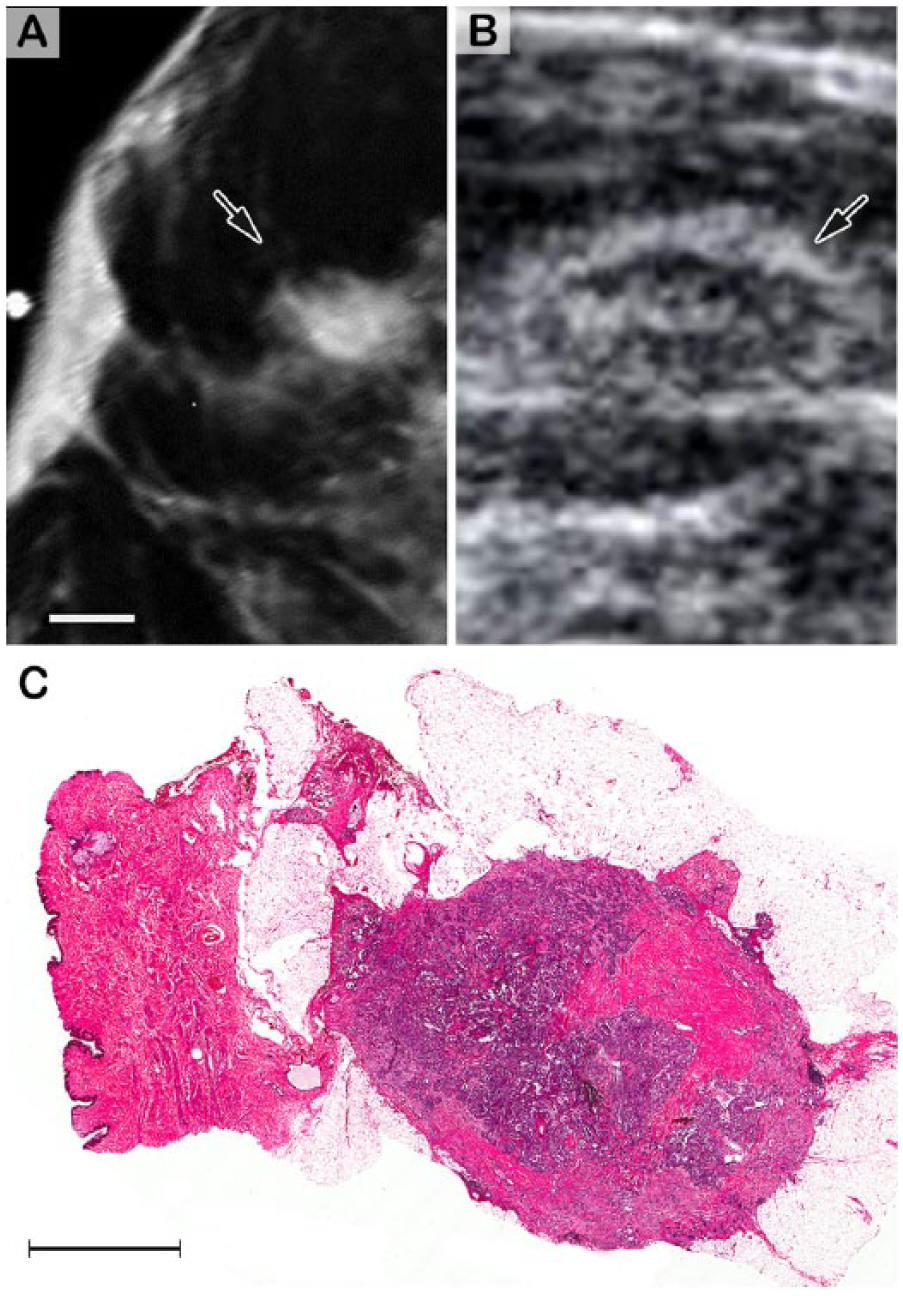
Subareolar sclerosing ductal hyperplasia, typical appearance on mammogram and ultrasound, and on whole-mount microscopy. (A) Mammography of a typical lesion (arrow) shows relative circumscription of the mass with focally ill-defined edges. Bar = 0.4 cm. (B) Ultrasonography of the corresponding mass (arrow) shows relatively regular outer contour, a somewhat heterogeneous internal echo level with indistinct margins. (C) Whole-mount image shows the nodular mass to be circumscribed, albeit focally irregular, with proliferating hyperplastic glands embedded in densely fibrotic tissue. In this particular case, a portion of overlying areolar skin was excised since the areola (not the nipple) “seemed retracted”. Bar = 0.4 cm.
A preoperative needle core biopsy had been performed in 5 cases (Figure 2). All needle core biopsies had been interpreted as benign papillary lesion (n = 3) or sclerosing papilloma (n = 2).
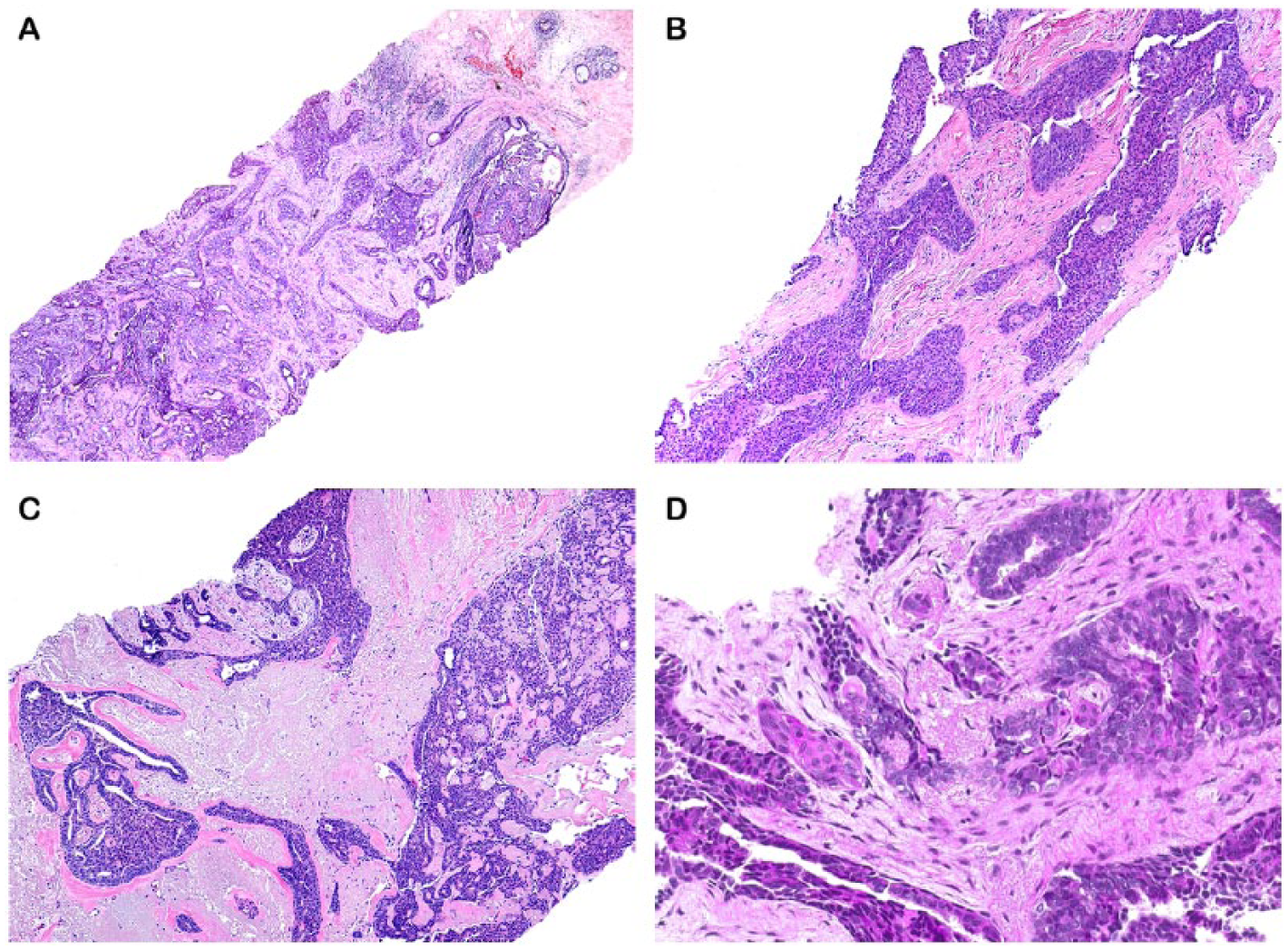
Subareolar sclerosing ductal hyperplasia, needle core biopsies. (A-D) Needle core biopsies of 4 cases of SSDH are shown. In each case, the tumor shows epithelial hyperplasia amid a densely sclerotic background. Note “infiltrative” lesional glands (A), florid epithelial hyperplasia (B), central elastosis (C), and minute foci of squamous metaplasia (D).
On macroscopic examination, SSDH appeared as a round or oval, tan or brown, mass with indistinct margins, and spanned a mean size of 1.3 cm (range = 0.4-3.0 cm). On microscopic evaluation, all cases showed a sclerosing papillary lesion associated with foci of moderate epithelial hyperplasia. There was intra- as well as perilesional desmoplasia with entrapment of glandular elements (Figure 3). The latter process imparted an “infiltrative” appearance, at least focally, to each lesion. The sclerosing process was as evident in the center as it was at the perimeter of the lesion. Focal keloid-like stroma was evident. The proliferative epithelium formed complex patterns. The epithelial cells lining the fibrovascular cores showed foci of columnar cell change and apocrine metaplasia. Rare foci of minimal luminal secretions admixed with cellular debris were evident. A few glands within the SSDH lesion in 13 cases displayed atypical ductal hyperplasia (ADH), that is, a modest degree of architectural irregularity, associated with cytological atypia.
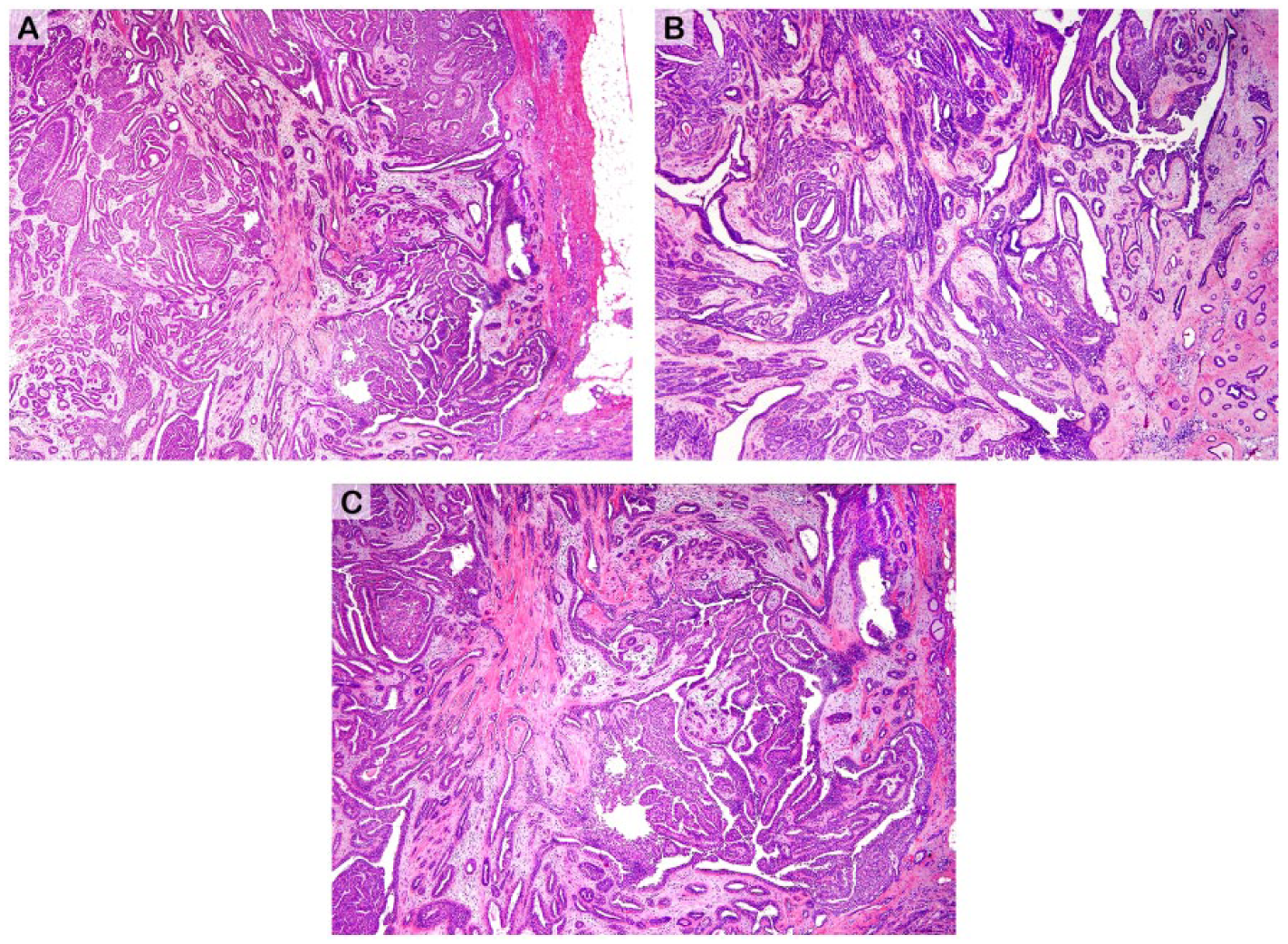
Subareolar sclerosing ductal hyperplasia, excisional biopsies. (A-C) Three different cases of SSDH are shown. In each case, the tumor exhibits a dominant papillary pattern and is associated with varying degrees of epithelial hyperplasia. Note sclerotic entrapment of lesional glands—centrally and at the perimeter.
High-molecular-weight cytokeratin (eg, CK5/6), performed in 7 cases, showed mosaic-like reactivity in the lesional hyperplastic epithelia (Figure 4A). A relatively higher proportion of CK5/6-positive cells were present at the periphery of each lesion. In 7 cases, estrogen receptor (ER) immunostaining showed a heterogeneous pattern of reactivity with approximately 75% of the lesional cells showing moderate to strong reactivity (Figure 4B). Myoepithelial immunostains, including smooth muscle myosin (Figure 4C) and p63 (Figure 4D), performed in 3 cases, showed preservation of myoepithelial cells around almost all “infiltrative” proliferative glands—although immunostaining for myoepithelial cells was focally absent around the perimeter of some lesional glands in rare sclerotic, centrally and peripherally located, foci (Figure 4E).
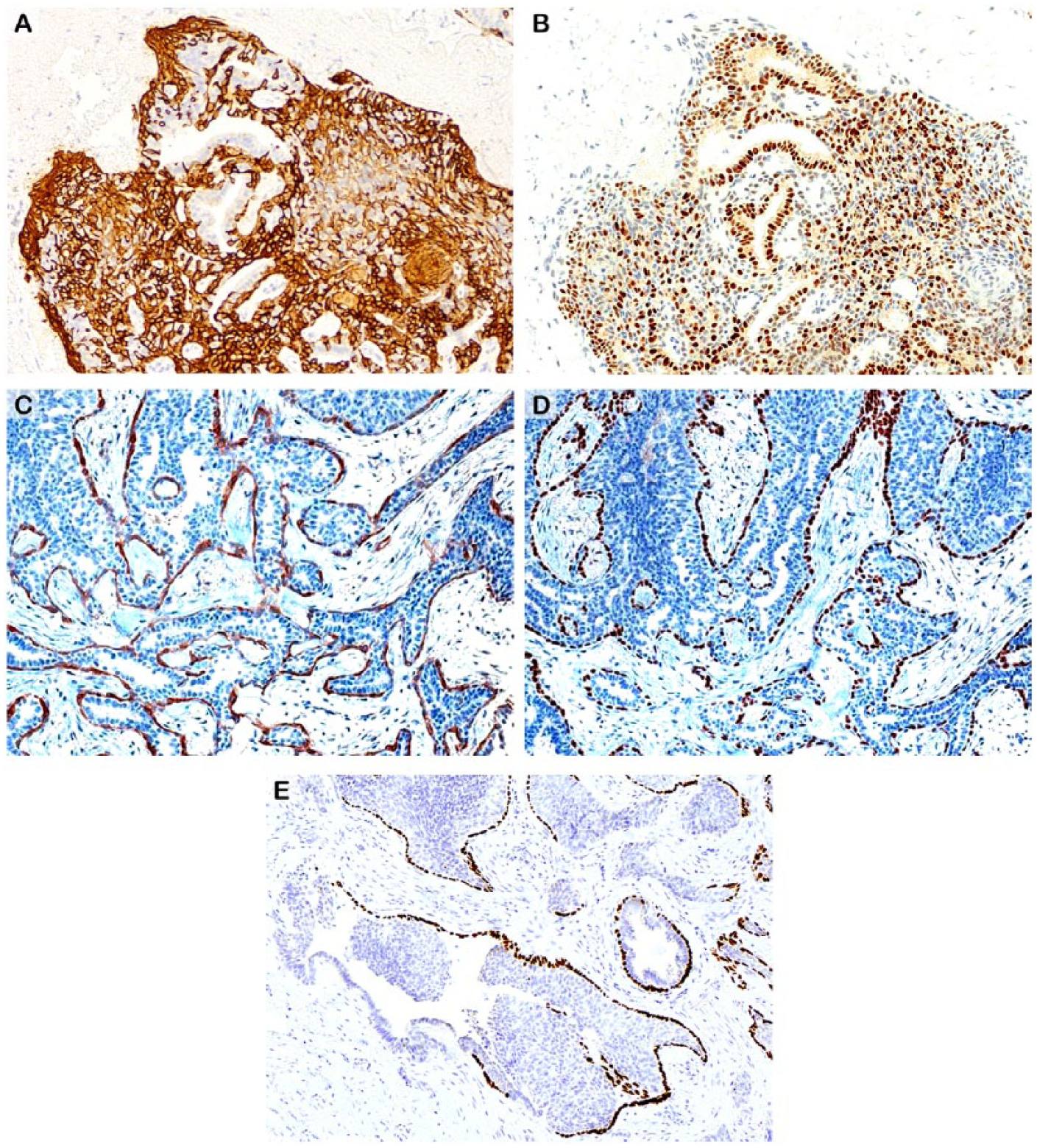
Subareolar sclerosing ductal hyperplasia, typical immunohistochemical findings. (A) Cytokeratin 5/6 immunostain shows “mosaic-like” reactivity in the lesional hyperplastic glands. (B) Estrogen receptor (ER) immunostaining shows strong immunoreactivity in the bulk (approximately 90%) of lesional cells. Smooth muscle myosin (C) and p63 (D) immunostains show preservation of myoepithelial cells around the “infiltrative” proliferative glands. (E) Some proliferating glands show partial absence of p63 immunoreactivity for myoepithelial cells along the perimeter.
Significant lesions that coexisted within SSDH were low-grade adenosquamous carcinoma (LGASC; n = 1), ductal carcinoma in situ (DCIS; n = 1), lobular carcinoma in situ (LCIS) of the classic type (n = 1, focal), and ADH (n = 13). LGASC in a 47-year-old woman was characterized by elongated clusters of neoplastic glandular and squamous cells infiltrating a densely sclerotic stroma (Figure 5). The LGASC spanned 1.0 cm, and was located at the periphery of the dominant, otherwise typical, SSDH lesion. No DCIS was identified in this case. The patient underwent ipsilateral mastectomy and has no evidence of breast disease 12 years later. DCIS was present at the perimeter of another otherwise classic example of SSDH in a 51-year-old woman. This DCIS spanned 0.3 cm and was characterized by marked epithelial atypia and luminal necrosis admixed with karyorrhectic debris (Figure 6). The patient was treated conservatively—undergoing excisional biopsy followed by radiation. This patient had no evidence of breast disease 6 years later. All cases of ADH, and the solitary case of LCIS, were located within the SSDH lesion.
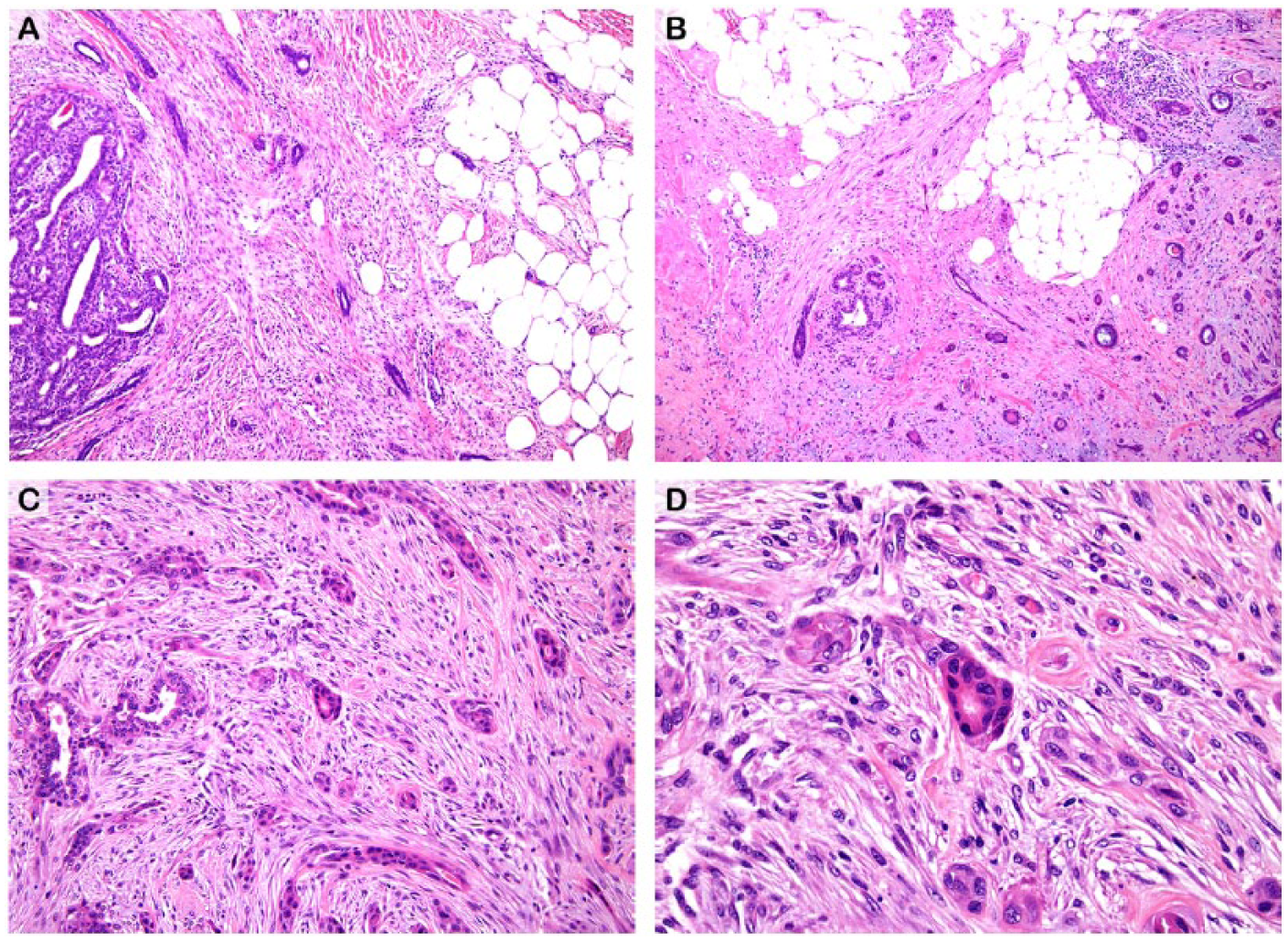
Low-grade adenosquamous carcinoma concurrently associated with subareolar sclerosing ductal hyperplasia. (A) Note neoplastic glands invading spindle cell stroma and adipose tissue. The periphery of subareolar sclerosing ductal hyperplastic process is seen (at left). (B) The haphazard infiltrative appearance of the invasive carcinoma is evident. (C, D) The invasive carcinoma is represented by epithelial (“tadpole-like”) strands amid a hypercellular spindle cell stroma. Squamoid differentiation is focally evident. All figures of LGASC are of the only such case associated with SSDH in this case.
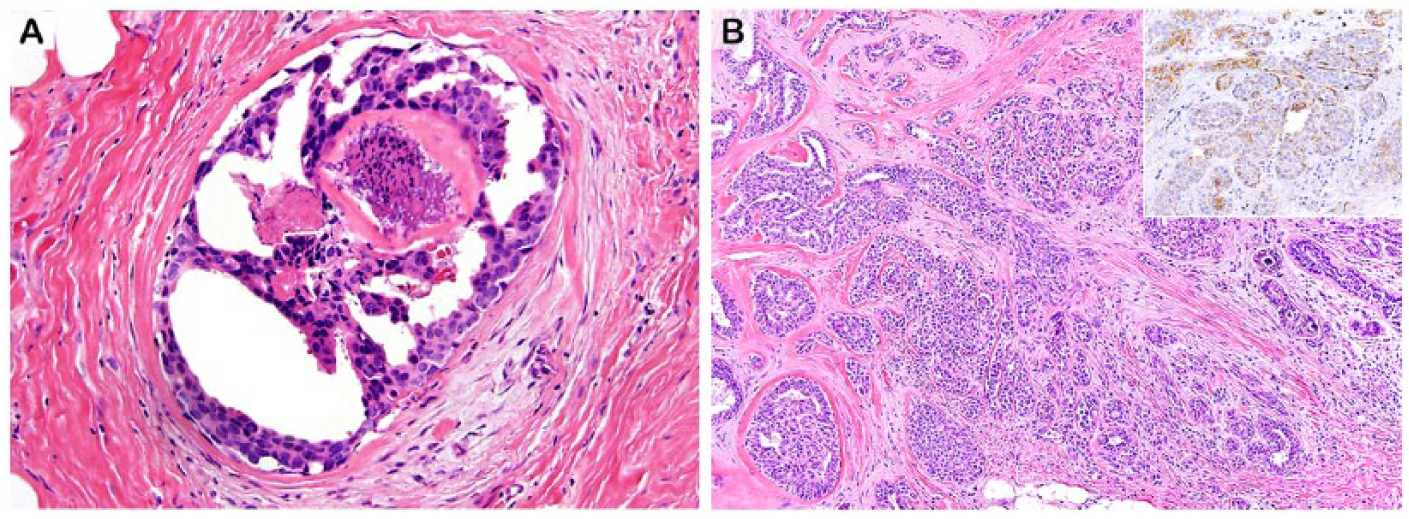
In situ carcinoma concurrently associated with SSDH. (A) Ductal carcinoma in situ (DCIS) of the micropapillary type. Note micropapillary structures lined by neoplastic cells bearing high-grade nuclei, and dense periductal sclerosis. Presence of intraluminal necrosis admixed with karyorrhectic debris in the lesional gland is supportive of the diagnosis of DCIS. (B) Lobular carcinoma in situ (LCIS) of the classic type concurrent with SSDH. Note dense stromal fibrosis. Inset shows the lesional cells to be negative for Ecadherin (supporting the diagnosis of LCIS). Residual native ductal epithelium and myoepithelial cells show weak immunoreactivity for E-cadherin.
The only mastectomy performed in our set of 35 SSDH cases was for LGASC. The ipsilateral mastectomy showed no significant abnormality. One patient underwent excision of the overlying nipple for clinical suspicion of Paget disease vide supra; however, no carcinoma was histologically evident in this case. A portion of the histologically unremarkable areolar skin overlying SSDH was excised in one case for technical reasons (Figure 1C).
There was no recurrence of SSDH on follow-up of 26 (74%) cases in a mean follow-up of 44 months (range = 6-189). Follow-up data were unavailable in 9 cases. The 2 patients with DCIS and LCIS were treated conservatively (with radiation only in the DCIS case, and with selective estrogen receptor modulator in the LCIS case). Neither case showed evidence of recurrence of either malignancy in a follow-up of 67 and 89 months, respectively. Follow-up in 6 patients showed mammographically detected calcifications (that developed 12-50 months after the diagnosis of SSDH). Excisional biopsies performed in these 6 cases revealed DCIS (n = 3, ipsilateral 2, contralateral 1), ADH (n = 2, both ipsilateral), and atypical lobular hyperplasia (n = 1, ipsilateral). None of the 3 cases of DCIS diagnosed during the follow-up period were located centrally (ie, in the subareolar region). Five additional patients presented with a palpable mass in either breast (n = 5, ipsilateral 3, contralateral 2). Excisional biopsies performed in these 5 cases revealed various types of proliferative (“fibrocystic”) changes including florid ductal hyperplasia, radial scar, and sclerosing adenosis (all without atypia).
Discussion
In 1987, Rosen described 12 cases of a “distinct” proliferative entity that formed a discrete subareolar mass with a complex papillary and sclerosing configuration, and bestowed the descriptive designation of “subareolar sclerosing duct hyperplasia” (SSDH) to the lesion. 5 In the only other published series of SSDH by Tresserra et al, 8 cases of the entity were described. 7
In Rosen’s series, one case was concurrent with carcinoma (DCIS “arising in SSDH”) at the time of diagnosis. 5 Follow-up, albeit brief (mean = 31 months), showed neither carcinoma nor recurrence of SSDH (although SSDH persisted in 2 cases, presumably following incomplete excision). 5 In Tresserra’s case series, no malignancy was concurrently or subsequently diagnosed. 7 In our series of 35 SSDH cases, the largest reported thus far, significant lesions that were concurrent at the time of initial diagnosis included one case each of low-grade adenosquamous carcinoma, DCIS, and LCIS. No case of SSDH recurred in a follow-up of 26 (74%) cases in a mean follow-up of 44 months; however, 2 cases of DCIS were subsequently diagnosed in the ipsilateral breast and one in the contralateral breast. Table 1 summarizes the key findings in the 3 case series of SSDH reported to date.6,7
Subareolar Sclerosing Ductal Hyperplasia: Summary of Case Series.
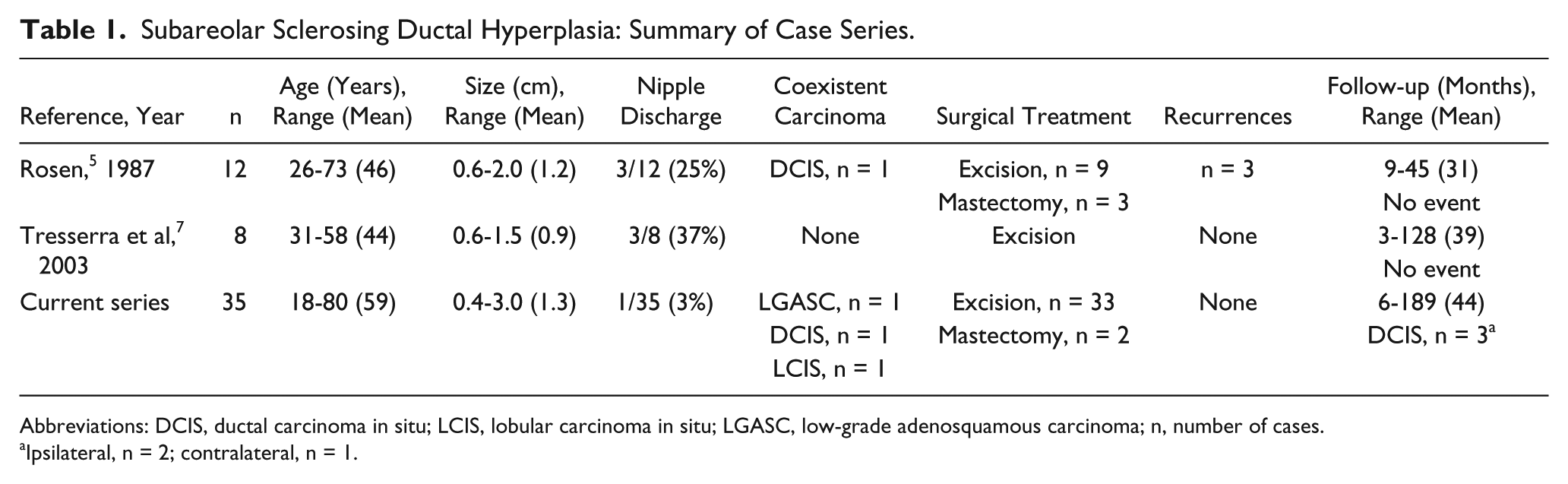
Abbreviations: DCIS, ductal carcinoma in situ; LCIS, lobular carcinoma in situ; LGASC, low-grade adenosquamous carcinoma; n, number of cases.
Ipsilateral, n = 2; contralateral, n = 1.
Thirty of the 35 cases that were included in our series had been submitted for consultative opinion and had a “working pathological diagnosis” of “sclerosing papilloma,” “florid papillomatosis,” or “complex sclerosing lesion/radial scar.” Classical examples of all 3 aforementioned lesions are sufficiently distinctive and should not be mistaken for SSDH. Sclerosing papillomata when located in close proximity to the nipple-areolar complex present with bloody nipple discharge, whereas most cases of SSDH do not. Furthermore, in contradistinction to SSDH, the major duct harboring the papilloma can be readily discerned in its vicinity. Although SSDH shares several histopathological features with the prototypical florid papillomatosis of nipple including exuberant epithelial hyperplasia and underlying papillary architecture, the fundamental difference between the two is that while the latter invariably involves the nipple the former is (as the name implies) subareolar.8-10 Complete excision of SSDH can usually be performed without removal of the nipple. Nonetheless, it is possible that in some cases of SSDH clinically apparent “nipple retraction,” “tethering of skin,” or other “technical problems” may require excision of the nipple (or of the overlying areolar skin; Figure 1C). Complete excision of florid papillomatosis inevitably requires removal of nipple. According to the World Health Organization’s latest Classification of Tumours of the Breast, a complex sclerosing lesion refers to a radial scar that is “larger” or has “more complex features.” 11 Using this broad definition, it would not be inaccurate to call SSDH as a complex sclerosing lesion; nevertheless, it would not be accurate either! Be that as it may, a classic radial scar has a stellate configuration (radiographically, grossly, and on low-power microscopy) whereas SSDH is typically nodular. Stromal fibrosis and elastosis are present in both, but fibroelastosis is located in the center of the radial scar and is more diffusely present in SSDH. In this regard, it is notable that Fechner and Mills preferred the term subareolar papillomatosis to SSDH “because not all examples have a prominent sclerotic component.” 6
The relative paucity of published case series or even case reports of SSDH leads us to believe that most SSDH lesions are being diagnosed using any one of the several diagnostic terms that are included in the rubric of CSPHL. The latter group of lesions are characterized by “streaming” of proliferating cells, formation of irregular spaces, papillary architecture, and dense scleroelastosis. Some authors have described particular features in some entities; for example, Eusebi and Millis have described frequent squamoid appearance in infiltrating epitheliosis; however, squamous metaplasia can be encountered in any CSPHL. 1 Indeed, LGASC and other metaplastic carcinomas have been associated with CSPHL.12,13
In general, all CSPHL show either diffuse uniform or (more often) mosaic-like immunoreactivity for CK5/6 in the hyperplastic epithelial cells. 14 Likewise, SSDH cases generally show diffuse reactivity with CK5/6—in the manner of usual ductal hyperplasia. Myoepithelial cells can be demonstrated via immunostains to line most of the perimeter and the intralesional fibrovascular cores of SSDH lesions and CSPHL—although there can be focal absence of myoepithelial cell immunoreactivity in markedly sclerotic foci thereof (as commonly encountered at the center of radial scars). 15
CSPHL (including radial scar) comprise less than 8% of all breast lesions and are concurrent with carcinoma in 3.6% to 32% of cases.16-21 Whether or not CSPHL, in general, and SSDH, in particular, truly represent an independent risk factor or a nonobligate precursor of breast carcinoma remains uncertain at this time.
Molecular studies may elucidate the biological potential of CSPHL and SSDH, although the genetic characteristics of the prototypical mammary papillary lesion appear to be rather heterogeneous. Loss of heterozygosity of 16q23 and at the TP53 locus has been found in malignant papillary lesions, and loss of heterozygosity at 16p13 and 16q21 loci has been detected in benign and malignant papillary lesions. 22 Another study has shown lower frequency of activating point mutations of PIK3CA, AKT1, and NRAS genes in papillary carcinomas when compared with benign papillomata. 23
In summary, we have added 35 cases of SSDH to the existing list of reported cases and have confirmed the clinical and pathological findings that were described in the 2 case series published earlier. Based on cumulative data, SSDH tends to occur in older women as a central, solitary, and unilateral lesion with distinctive histopathology and a clinical course that is generally, but not always, benign. In our set of SSDH cases, reported herein, one case each of LGASC, micropapillary DCIS, and classic LCIS was concurrently present at initial diagnosis; no SSDH lesion recurred; and DCIS was subsequently diagnosed in 3 cases (including 2 cases in the ipsilateral breast, although not in the central location). Complete excision and long-term clinical and radiological follow-up is recommended for all cases of SSDH. In contradistinction to florid papillomatosis of nipple, neither nipple nor areola need to be excised for SSDH—unless there is a confounding clinical (or technical) reason.
Footnotes
Acknowledgements
Ms Patricia Kuharic assisted with the preparation of the photographic material. Multiple physicians and their office staff provided follow-up information on patients included in this study.
Authors’ Note
This study was presented, in part, at the annual meeting of the United States and Canadian Academy of Pathology Meeting in Seattle, WA, in March 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.