
Abstract
Granular cell tumor (GCT) rarely involves the central nervous system, and fewer than 100 cases have been reported in English literatures. We herein report a case of a 36-year-old Chinese man with GCT of the neurohypophysis. Magnetic resonance imaging showed one mass located in the hypophysis with heterogeneous contrast enhancement. Pathological examination showed a neoplasm comprising densely packed polygonal cells of ample cytoplasm with abundant eosinophilic granules inside. The nuclei were small with inconspicuous nucleoli and yet without any mitoses. The tumor was positive for S-100, CD68, CD163, lysosome, and vimentin. Translocation factor E-3 (TFE-3) was diffusely nuclear positive although ASPSCR1-TFE-3 fusion was not detected by fluorescence in situ hybridization. GCT of the neurohypophysis is supposed to be considered under differential diagnosis with neoplasms or lesions of histiocytic origin and others such as pituitocytoma and spindle cell oncocytoma. A group of markers such as GFAP, EMA, CD68, S-100, and PAS staining are useful in complementary diagnosis and TFE-3 may be an alternative marker.
Keywords
Introduction
Granular cell tumor (GCT), which is characterized by abundant eosinophilic granules in the cytoplasm, always involves various anatomic sites throughout the body, including the tongue, digestive system, skin, and soft tissue. Involvement of the central nervous system is rare, and fewer than 100 cases have been reported in the English literature since GCT located in the saddle area was described in 1893 first. We experienced 1 case of GCT of the neurohypophysis (GCTN). Herein, we present the case and discuss with review of literature.
Case Presentation
A 36-year-old Chinese man presented with 10-day history of intermittent dull headache, especially in the bilateral temporal region, without vomiting, seizures, polyuria, visual field deficit, and so on. Physical examination revealed no significant differences. Serum cortisol was 73.0 nmol/L (normal 185-624 nmol/L) and the other pituitary hormones were normal. Brain magnetic resonance imaging (MRI) showed one mass located in the hypophysis with heterogeneous contrast enhancement (Figure 1). Diagnosis of pituitary adenoma was recommended. Surgery was performed and the white tumor with a diameter of 0.8 cm was resected.
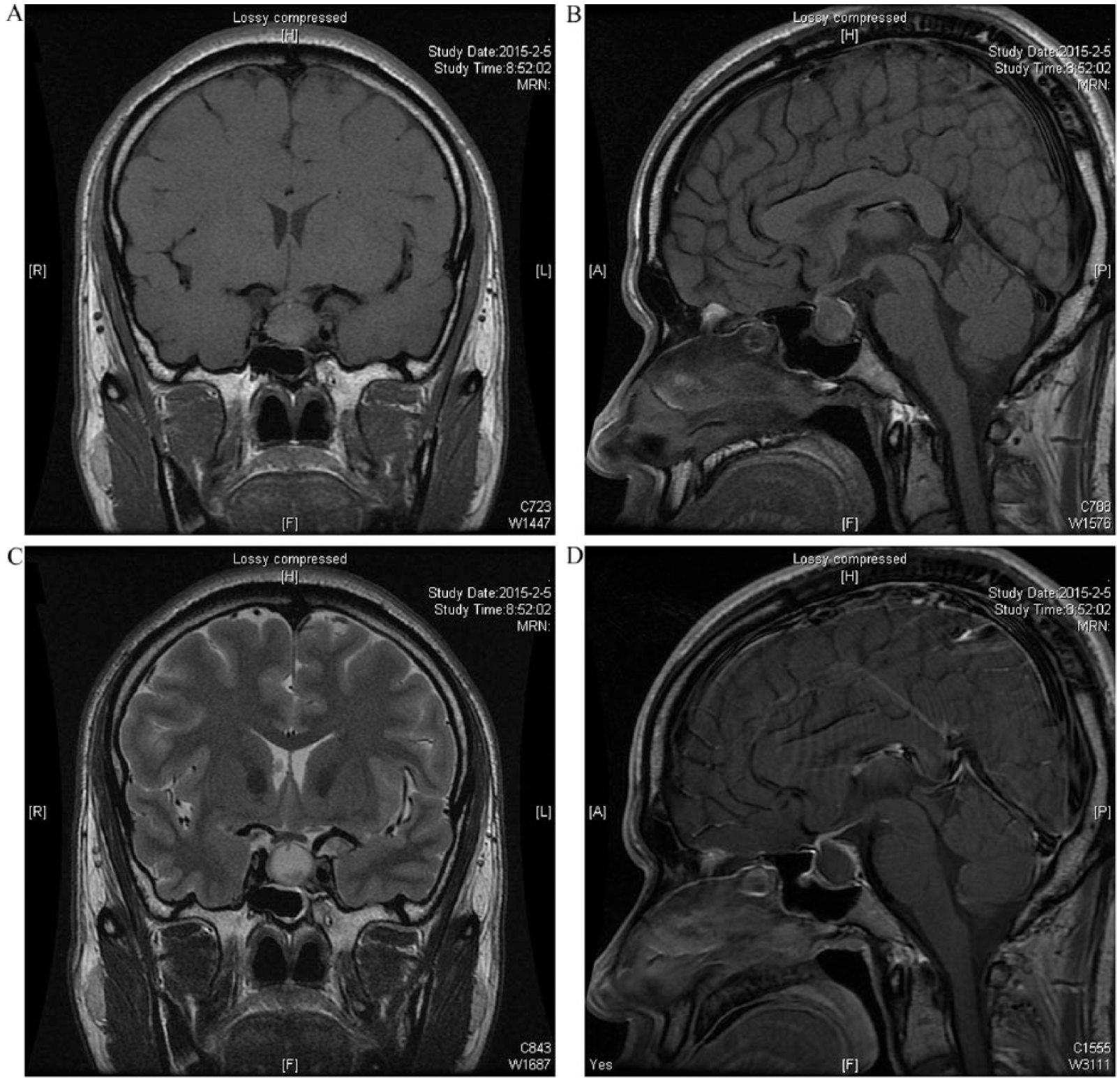
Magnetic resonance images of a 36-year-old man with one mass located in the hypophysis. Coronary (A), sagittal (B) T1-weighted images and coronary (C) T2-weighted images showed pituitary solid mass. Sagittal (D) enhanced T1-weighted images showed heterogeneous enhancement.
Histologically, the tumor consisted of densely packed polygonal cells. The neoplastic cells possessed ample cytoplasm with abundant eosinophilic granules inside. The nuclei were small with inconspicuous nucleoli and mitoses were absent.
Immunohistochemically, the tumor was positive for S-100 protein, CD68, CD163, lysozyme, translocation factor E-3 (TFE-3), and vimentin. CD1a, glial fibrillary acidic protein (GFAP), neuron-specific enolase (NSE), synaptophysin (Syn), chromogranin A (CgA), thyroid transcription factor-1 (TTF-1) and pituitary hormone markers were negative. Ki-67 labeling index was about 3%. Periodic acid–Schiff (PAS) and diastase-digested PAS staining showed positive granules in the cytoplasm. ASPSCR1-TFE3 fusion was not detected by fluorescence in situ hybridization (FISH; Figure 2).
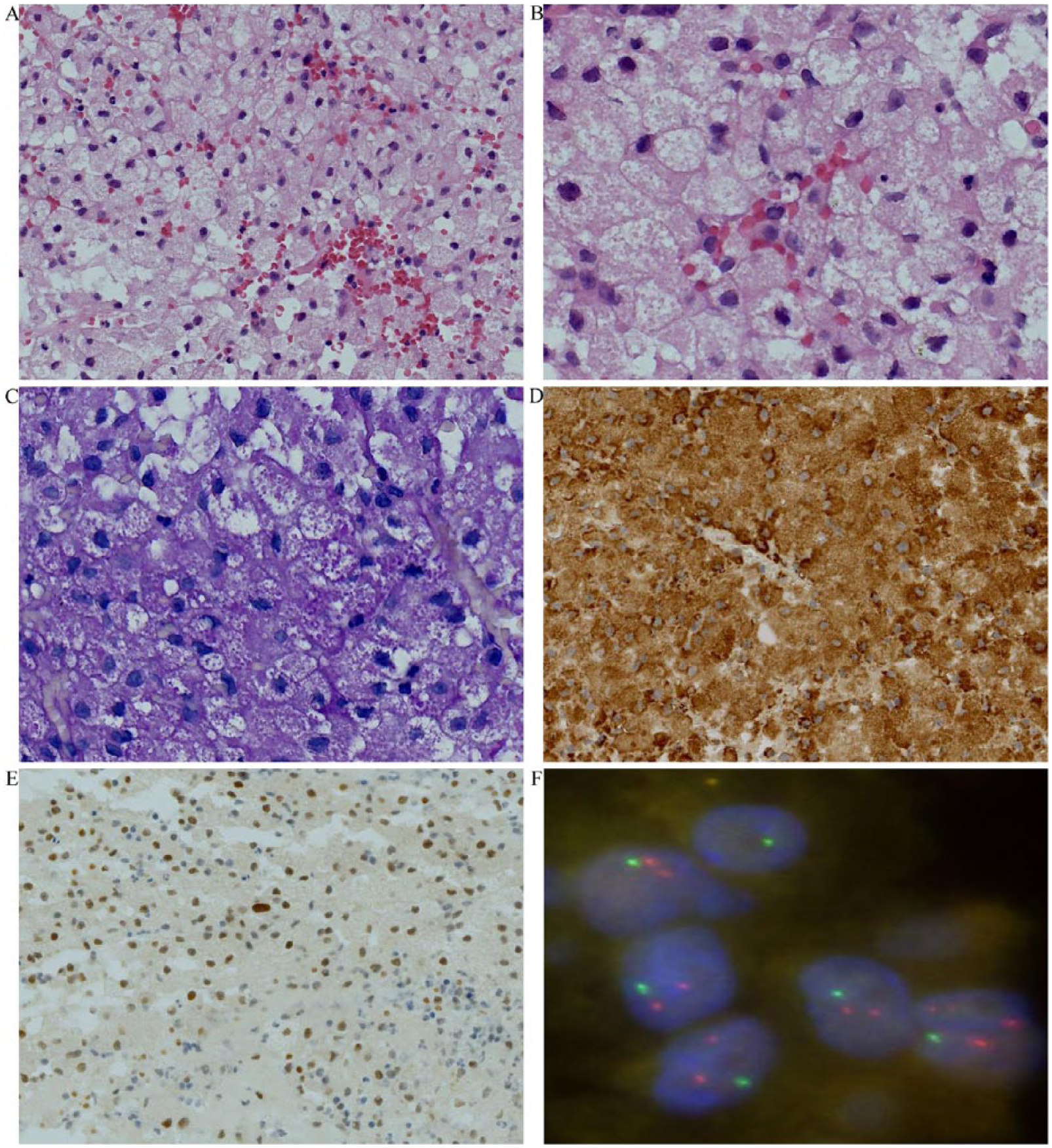
Pathological features of granular cell tumor of the neurohypophysis (GCTN). (A) The tumor consisted of densely packed polygonal cells (magnification, 200×). (B) The neoplastic cells had ample cytoplasm within abundant eosinophilic granules (magnification, 400×). (C) Diastase-digested periodic acid–Schiff (PAS) staining showed positive granules in cytoplasm (magnification, 400×). (D) The tumor cells were positive for CD68 (magnification, 200×). (E) The tumor cells were nuclear positive for TFE-3 (magnification, 200×). (F) ASPSCR1-TFE-3 fusion gene detection was negative by fluorescence in situ hybridization (FISH). Red signal represents ASPSCR1 gene and green represents TFE-3 gene.
The patient received no adjuvant therapies and remained free of recurrence after 1 year of follow-up.
Discussion
Like GCTs in other locations, GCTNs always affect adults at peak age in the fifth and sixth decade in females and males, respectively. GCTNs are more prevalent in females with a female-to-male ratio of more than 2:1. 1 Although symptomatic cases of GCTN are rare, asymptomatic tumorlets are more common and have been documented with an incidence up to 17% in pituitary autopsy. 2
The presenting symptoms and complaints of GCTNs include visual field deficit, panhypopituitarism, galactorrhea, amenorrhea, diabetes insipidus, headache, and so on. 3 There are no reliably diagnostic signs since most are secondary to mass effects. Symptoms usually develop gradually, which is corresponding to the clinic-biological characteristics of slow growth of GCTNs.
MRI typically shows a well-circumscribed suprasellar mass with homogeneous or heterogeneous enhancement. 3 Lack of calcification and a dural attachment help to distinguish GCTN from craniopharyngioma or meningoma. Only in a few cases was the tumor separated from the pituitary by the inferior end of the pituitary stalk, which was a relatively specific suggestion of GCTN. 4 The rarity of GCTN makes accurate diagnosis difficult prior to pathological investigation.
The microscopic architecture of GCTN is always nodular, and occasionally in sheets or fascicular patterns. The neoplastic cells are round or polygonal with diagnostically abundant eosinophilic granules in the cytoplasm. The nuclei are small with inconspicuous nucleoli and mitoses are absent. A few neoplasms characterized by nuclear pleomorphism, prominent nucleoli and increased mitotic activity (up to 5 mitoses per 10 high-power field or Ki-67 index of 7%) are favored as atypical GCTN, whereas the clinical outcomes are still uncertain.5,6
In immunohistochemistry, GCTNs are variably positive for S-100, CD68, vimentin, antitrypsin, antichymotrypsin, and NSE, and negative for cytokeratin, Syn, CgA, desmin, and the pituitary hormones. Only a few cases are positive for GFAP. The immunophenotype of the reported case was similar to the documented examples.
It is notable that our case showed diffuse nuclear expression of TFE-3, whereas ASPSCR1-TFE3 fusion was not detectable by FISH, which was quite consistent with the recent studies.7,8 TFE-3 is a ubiquitous transcription factor whose overexpression is crucial to screen neoplasms of the TFE-3 family which underlies Xp11.2 translocation. It is believed that strong expression of nuclear TFE-3 is sensitive and specific for TFE-3 gene fusion, yet GCT may be an exception. 8 Ultrastructural investigation confirmed that the cytoplasm of the GCTN is filled with intermediate filaments, desmosomes and lysosomes, which are positive granules in PAS staining correspondingly. 9 It is supposed that aberrant nuclear TFE-3 accumulation may induce the characteristic cytoplasmic accumulation of phagolysosomes in GCT since TFE-3 is instrumental in feedback regulation of lysosome/phagosome synthesis and the Golgi stress response. 10
The exact diagnosis of GCTN depends on pathological examination. Neoplasms or lesions of histiocytic origin are supposed to be in the differential diagnosis because the typical histopathological manifestations of GCTN are large pleomorphic cells with abundant eosinophilic granules in the cytoplasm and immunohistochemical constant expressions of histiocytic markers. However, the cytoplasms of histiocytes are vacuolated or bubbly, rather than full of eosinophilic granules. In addition, PAS staining or immunohistochemical staining such as S-100 protein may facilitate accurate diagnosis.
GCT is a descriptive term of a histogenetically heterogeneous group of neoplasms according to morphological features and mostly of Schwann cell origin, whereas GCTN is likely to originate from pituicytes. Diffuse TTF-1 expression was detected in nontumorous pituicytes, pituicytomas, spindle cell oncocytomas and GCTNs, in combination with ultrastructural studies, displayed a common pituicyte lineage. 11 However, TTF-1 expression was not confirmed in our case. According to the latest World Health Organization classification, pituitocytoma and spindle cell oncocytoma are supposed to be differentiated from GCTN, and a combination of markers such as GFAP, EMA, CD68, and PAS staining is useful.
Most GCTNs pursue a benign clinical course with slow progress and surgery is the preferred treatment. Postoperative radiation seems unnecessary for cases without complete resection, and so far no studies have confirmed that radiation improved the survival. 9 For a few cases of so-called atypical GCTN, further data may be accumulated for the clinical course and treatments.
Conclusion
Here, we present a rare case of 36-year-old male with GCTN. MRI displayed one mass located in the hypophysis with heterogeneous contrast enhancement. Pathological examination showed a neoplasm comprising densely packed polygonal cells of ample cytoplasm with abundant eosinophilic granules inside. The nuclei were small with inconspicuous nucleoli and mitoses were absent. The tumor was positive for S-100, CD68, CD163, lysosome, and vimentin immunohistochemically. PAS and diastase-digested PAS staining showed positive granules in the cytoplasm. It is notable that our case showed diffuse nuclear expression of TFE-3, whereas ASPSCR1-TFE-3 fusion was not detected by FISH. GCTN is one rare neoplasm in the saddle area with benign clinical biological behavior, which is supposed to be considered in the differential diagnosis with neoplasms or lesions of histiocytic origin and others such as pituitocytoma and spindle cell oncocytoma. GCTN may always show diffuse nuclear expression of TFE-3 without ASPSCR1-TFE-3 fusion just like GCTs in other locations. A group of markers such as GFAP, EMA, CD68, S-100, and PAS staining are useful in complementary diagnosis and TFE-3 may be an alternative marker.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.