
Abstract
We report the case of a sclerosing perineurioma with conspicious collagen rosette formation in a 20-year-old male presenting with a firm, painless nodule on the palmar side of his right ring finger. The main differential diagnosis is a low-grade fibromyxoid sarcoma. The distinction between these entities is important because low-grade fibromyxoid sarcoma has a metastatic potential, while, as a rule, perineuriomas are benign. The presence of collagen rosettes in this current case makes this distinction even more difficult given that approximately 30% of low-grade fibromyxoid sarcoma cases show the focal presence of collagen rosettes. The demonstration of the characteristic t(7;16), t(11;16) or t(11;22) translocations (resulting in the FUS-CREB3L2, FUS-CREB3L1 or EWSR1-CREB3L1 fusion genes, respectively) or immunoreactivity for MUC4, a recently described sensitive and specific marker for low-grade fibromyxoid sarcoma, remain the gold standard in the diagnosis of low-grade fibromyxoid sarcoma, differentiating it from perineurioma. This case is, to our knowledge, the first report on collagen rosettes in sclerosing perineurioma, extremely well mimicking low-grade fibromyxoid sarcoma, and further expanding the morphological spectrum of this rare subtype of perineurioma.
A 20-year-old male presented with a firm, painless nodule on the palmar side of his right ring finger that was present for several months. Histopathological evaluation showed a fairly well-circumscribed nodular spindle cell proliferation embedded in a dense, homogenized collagenous stroma. Areas with myxoid changes were seen. Focally, prominent nodular condensation of the stroma with formation of collagenous rosettes was observed (Figure 1A and B). The slender spindle cells were arranged in a fascicular (lamellar) to whorled pattern having tapering nuclei, indistinct nucleoli, and distinct bipolar cytoplasmic endings (Figure 1C). No significant cytological atypia, pleomorphism, or necrosis was seen. Mitotic figures were inconspicuous. Immunohistochemical studies revealed diffuse reactivity for epithelial membrane antigen (EMA), glucose transporter 1 (Glut-1), and CD34, accentuating the elongated cytoplasmic processes (Figure 2A and B). The cells were uniformly negative for S-100, SOX10, glial fibrillary acidic protein, smooth muscle actin, desmin, and mucin 4 (MUC4). Fluorescence in situ hybridization was performed using break-apart probes for FUS and EWSR1 (Vysis LSI FUS and EWSR1 Break Apart Probe Kits; Abbott Molecular, Des Plaines, IL) and did not show rearrangement of FUS or EWSR1. Based on the characteristic histological features, and the supportive immunohistochemical and molecular findings, a diagnosis of a sclerosing perineurioma was rendered.
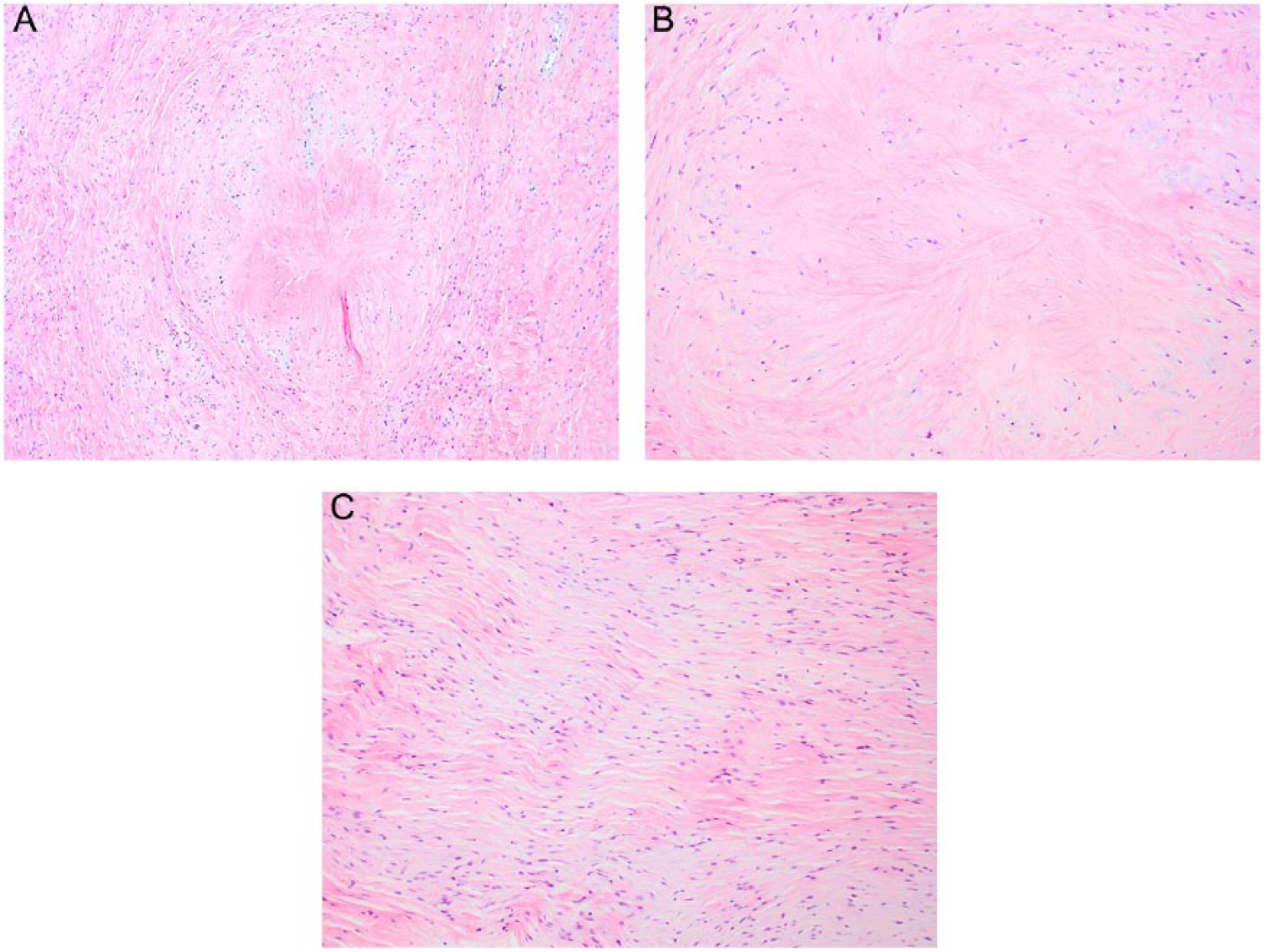
(A, B) Microscopy shows a spindle cell proliferation embedded in a dense, homogenized, sclerotic, and collagenous stroma within the center formation of a collagen rosette (hematoxylin and eosin, original magnification 40× and 400×). (C) In the most cellular areas, the slender spindle cells are arranged in a fascicular (lamellar) pattern and have tapering nuclei, indistinct nucleoli, and delicate bipolar cytoplasmic processes (hematoxylin and eosin, original magnification 400×).
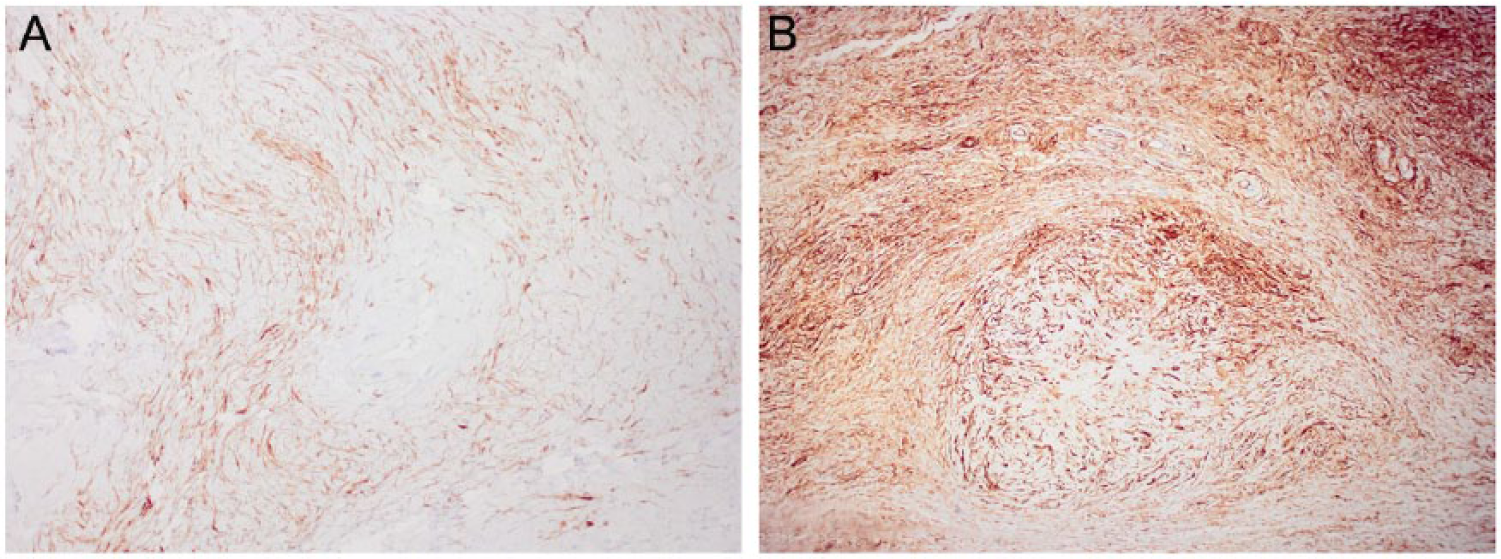
(A) The spindle cells show diffuse reactivity for EMA, accentuating the elongated cytoplasmic processes (original magnification 200×). (B) Strong and diffuse CD34 expression is seen, nicely illustrating the collagen rosette (original magnification 100×).
Perineurioma is an uncommon benign peripheral nerve sheath neoplasm derived from neoplastic perineurial cells. 1 Sclerosing perineurioma, first described by Fetsch and Miettinen 2 in 1997, is a rare soft tissue perineurioma subtype characterized by a strong predilection for the fingers and palms of young (male) adults (in contrast with ordinary perineurioma, which is found on the trunk and extremities). On histology, it forms a well-circumscribed fibrous collagenous nodule with a storiform, lamellar, and/or whorled arrangement of elongated spindle cells with slender nuclei and long bipolar cytoplasmic processes.3-5 The main differential diagnosis for the current case is a low-grade fibromyxoid sarcoma (LGFMS). The distinction between these entities is important because LGFMS has a low (but definite) metastatic potential, while, as a rule, perineuriomas are benign. The differential diagnosis may be difficult because sclerosing perineurioma can mimic LGFMS extremely well, as it displays bland cellular morphology, often grows in a whorled pattern, and may show myxoid changes. The presence of collagen rosettes in this current case makes this distinction even more difficult given that approximately 30% of LGFMS cases show the focal presence of collagen rosettes. In a subset of LGFMS in which these collagen rosettes are particularly prominent and well-formed, the term “hyalinizing spindle cell tumor with giant rosettes” was formerly applied. 6 Moreover, sclerosing perineuriomas, like soft tissue perineuriomas, show nearly always immunohistochemical expression of EMA and Glut-1, which are also expressed in a high percentage of LGFMS cases.1,3,7,8 Therefore, positivity for the “perineurial markers” EMA and Glut-1 should be interpreted together with clinical findings, morphology, immunoprofile, and genetic investigations where possible. The strong CD34 expression in current case is more in favor of the diagnosis of a perineurioma, as LGFMS is usually CD34 negative. 1 The demonstration of the characteristic t(7;16), t(11;16), or t(11;22) translocations (resulting in the FUS-CREB3L2, FUS-CREB3L1, or EWSR1-CREB3L1 fusion genes, respectively) or immunoreactivity for MUC4, a recently described sensitive and specific marker for LGFMS remain the gold standard in the diagnosis of LGFMS, differentiating it from perineurioma.7,9 This case is, to our knowledge, the first report on collagen rosettes in sclerosing perineurioma, extremely well mimicking LGFMS, and further expanding the morphological spectrum of this rare subtype of perineurioma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained in accordance with the Code of Conduct of the Medical Ethical Committee of the Ghent University Hospital.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not any clinical trials.