
Abstract
A combination of ovarian tumors with the same histogenetic origin but different histologic subtype is relatively common, whereas a co-occurrence of tumors with different histogenetic origin is rare. We report a case of mixed ovarian tumor composed of Brenner tumor and adult-type granulosa cell tumor, a combination that to the best of our knowledge has not been reported in the literature until now.
Introduction
Most ovarian tumors show a pure histologic type. However, a combination of tumors with the same histogenetic origin but different histologic subtype is relatively common. Co-occurrence of tumors with different histogenetic origin is very rare.
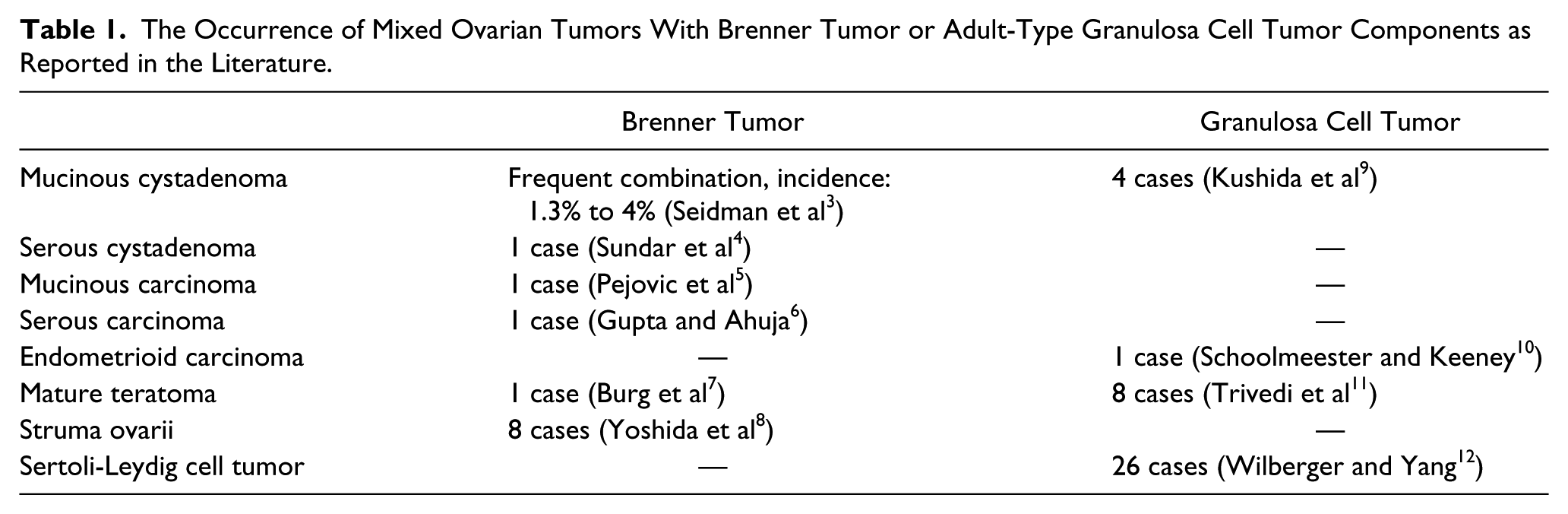
Brenner tumors composed of epithelial cells resembling urothelial cells represent 10% of epithelial ovarian tumors. 1 Nearly all of these tumors are benign. Borderline and malignant forms are uncommon. 1 One quarter of Brenner tumors are associated with other tumor types; among them, mucinous cystadenoma is the most common. 2 Adult-type granulosa cell tumors account for approximately 1% of all ovarian tumors. 2 Adult-type granulosa cell tumors occasionally occur in combination with other sex cord stromal tumors. A composition with non–sex cord stromal tumors is extremely rare. The histopathological diagnosis can be challenging, but testing for the presence of the FOXL2 402C→G mutation may improve diagnosis in problematic cases. Combinations of Brenner tumor and adult-type granulosa cell tumor with other tumor types reported in the literature so far are collated in Table 1.
The Occurrence of Mixed Ovarian Tumors With Brenner Tumor or Adult-Type Granulosa Cell Tumor Components as Reported in the Literature.
We report a case of mixed Brenner tumor and adult-type granulosa cell tumor. To the best of our knowledge, this has not been previously reported.
Materials and Methods
The patient’s clinical history was obtained from the MedWorks database. The diagnosis of ovarian tumor was based on the criteria of the World Health Organization (WHO) classification.
Surgical specimen was fixed in 8% formalin for 24 hours. Extensive tissue sampling was performed (1 block/cm diameter). Formalin-fixed paraffin-embedded sections of tissue were stained routinely with hematoxylin and eosin. BenchMark Ultra (Ventana Medical Systems, Inc, Tucson, AZ) slide staining system was applied for the immunohistochemical staining: cytokeratin (Biocare, Pacheco, CA; AE1/AE3 clone, 1:50 dilution), cytokeratin 7 (DAKO, Santa Clara, CA; OVTL clone, 1:200 dilution), calretinin (DAKO, Santa Clara, CA; DAK Calret 1 clone, 1:60 dilution), CD141 (Leica-Novocastra, Wetzlar, Germany; 15C8 clone, 1:100 dilution), inhibin (Biocare, Pacheco, CA; BC/R1 clone, 1:100 dilution), laminin (DAKO, Santa Clara, CA; 4C7 clone, 1:5 dilution), GATA3 (Biocare, Pacheco, CA; L50823 clone, 1:150 dilution), p63 (Zytomed, Berlin, Germany; 4A4 clone, 1:50 dilution), and PAX8 (Zytomed, Berlin, Germany; polyclonal, RTU [ready to use]). Detection was performed with UltraView Universal Alkaline Phosphatase Red Detection Kit (Ventana Medical Systems, Inc, Tucson, AZ) for cytokeratin, cytokeratin 7, inhibin, and with UltraView Universal DAB Detection Kit (Ventana Medical Systems, Inc, Tucson, AZ) for the other markers.
The presence of the FOXL2 (c.402C
Case Report
Clinical Data
A 66-year-old woman had a hysterectomy with ovarian conservation because of an endometrial polyp 22 years ago. Two years later, she was diagnosed with breast cancer and underwent mastectomy followed by radio-chemotherapy. In October 2013, during gynecologic routine check, pelvic ultrasonographic evaluation revealed a 43 × 26 mm right adnexal mass. Her preoperative tumor markers were as follows: CA-125 (49.30 U/mL; normal: 0.0-35.0 U/mL), HE4 (115.3 pmol/L; normal: 0.0-82.9 pmol/L), and CA-15-3 (50.9 U/mL; normal: 0.1-25 U/mL). The Risk of Ovarian Malignancy Algorithm index value was 42.40% (normal: 0.0% to 29.9% for postmenopausal women). This suggested malignancy. Magnetic resonance imaging showed a cystic right ovarian mass measuring 8 cm in largest diameter. No ascites or enlarged lymph nodes could be detected. Thereafter, exploratory laparotomy was performed, and a “fist-sized” ovarian tumor was removed with an intact capsule. Frozen section examination identified the tumor as a thecofibroma. However, the left ovary was macroscopically normal. Considering the patient’s postmenopausal status, a bilateral salpingo-oophorectomy was performed.
Histopathological Report
The tumor had a macroscopically smooth surface. It was 10 cm in largest diameter, and had a multicystic cut surface with a firm, yellowish, solid central region.
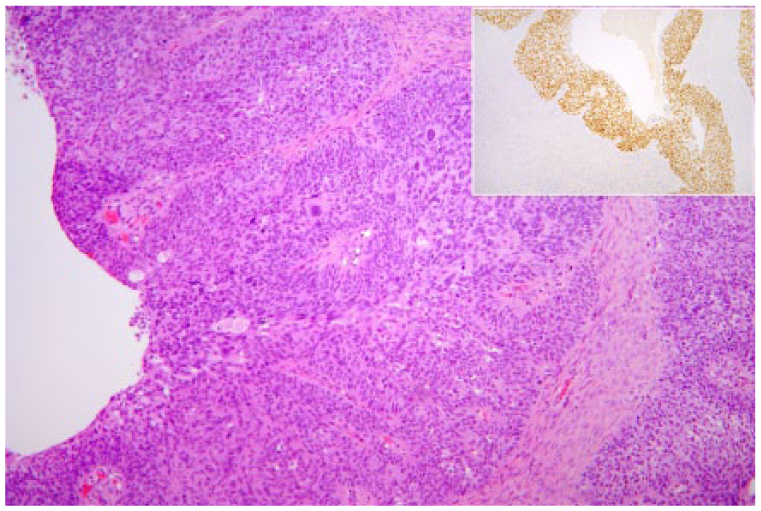
Microscopically, the tumor was composed of 2 distinct components with different histomorphology and immunophenotype. The 2 areas were predominantly separate but in parts were mixed (Figure 1). The larger of the 2 components, consisting of 70% tumor, had a mostly solid and partially trabecular pattern. The tumor cells had scant, eosinophilic cytoplasm and round to oval or angulated nuclei, some of which had grooves. The degree of nuclear atypia was mostly moderated, but focally tumor cells with 1 or 2 nucleoli showed severe nuclear atypia. The mitotic rate was 8/10 HPF (high-power field). Call-Exner bodies were identified (Figure 2). The stromal background composed of fibroblasts and theca cells intersected by fibrous bands and hyaline plaques. The tumor cells showed positive staining for inhibin and calretinin. CK7 staining was negative. Pancytokeratin immunohistochemical reaction showed dot-like positivity. Direct sequencing analysis showed that FOXL2 (C402G) missense mutation was present in this component of the tumor (Figure 3). The diagnosis of adult-type granulosa cell tumor was confirmed on the basis of morphological and immunohistochemical findings as well as molecular status.
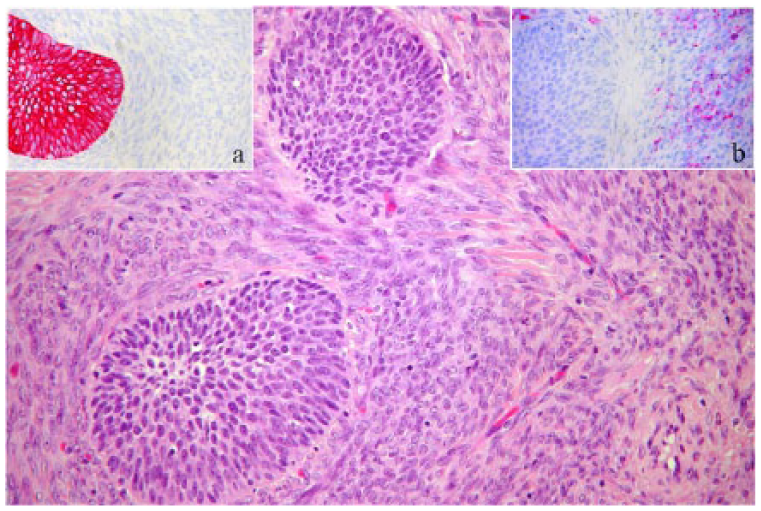
Solid cell nests of benign Brenner tumor admixed with granulosa cell tumor (hematoxylin and eosin, ×10); inset “a” showing positive staining for CK7 in Brenner tumor (CK7, ×20); inset “b” showing positive staining for inhibin in granulosa cell tumor (inhibin, ×20).
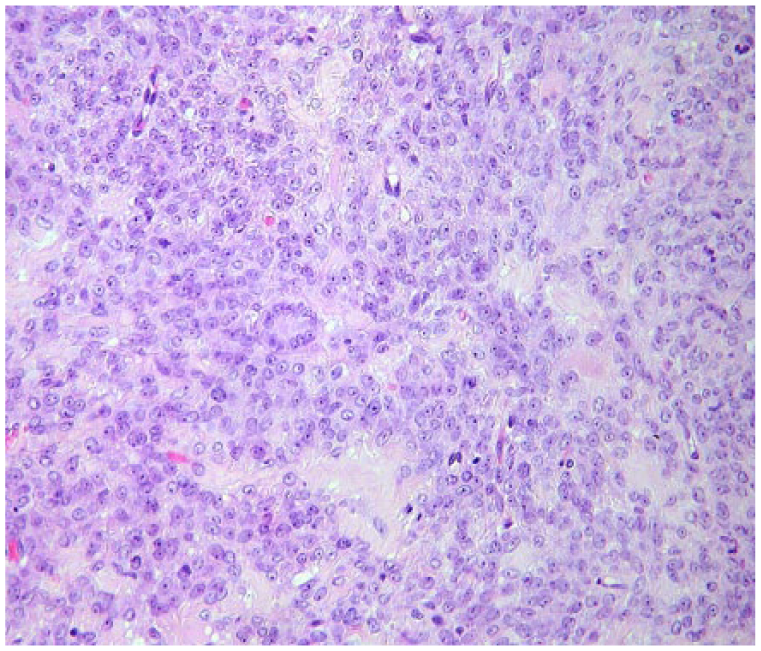
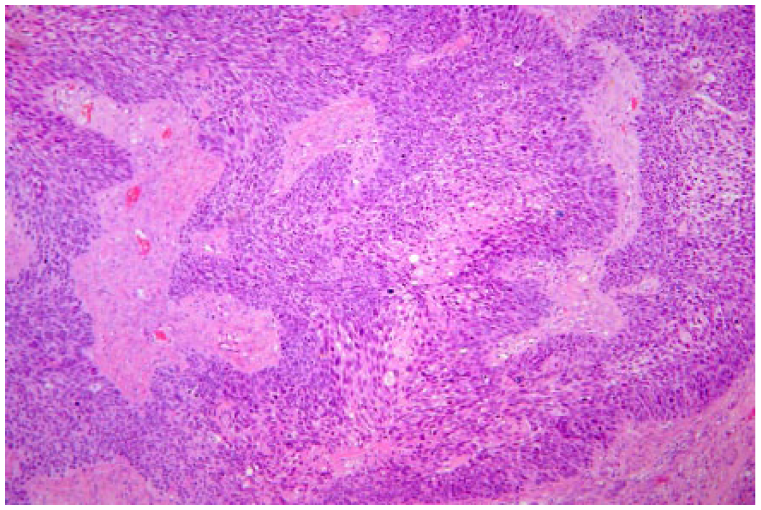
The degree of nuclear atypia is severe in this area of granulosa cell tumor. The tumor cells have scant, eosinophilic cytoplasm and oval or angulated nuclei with 1 or 2 prominent nucleoli. A Call-Exner body is identified (hematoxylin and eosin, ×40).
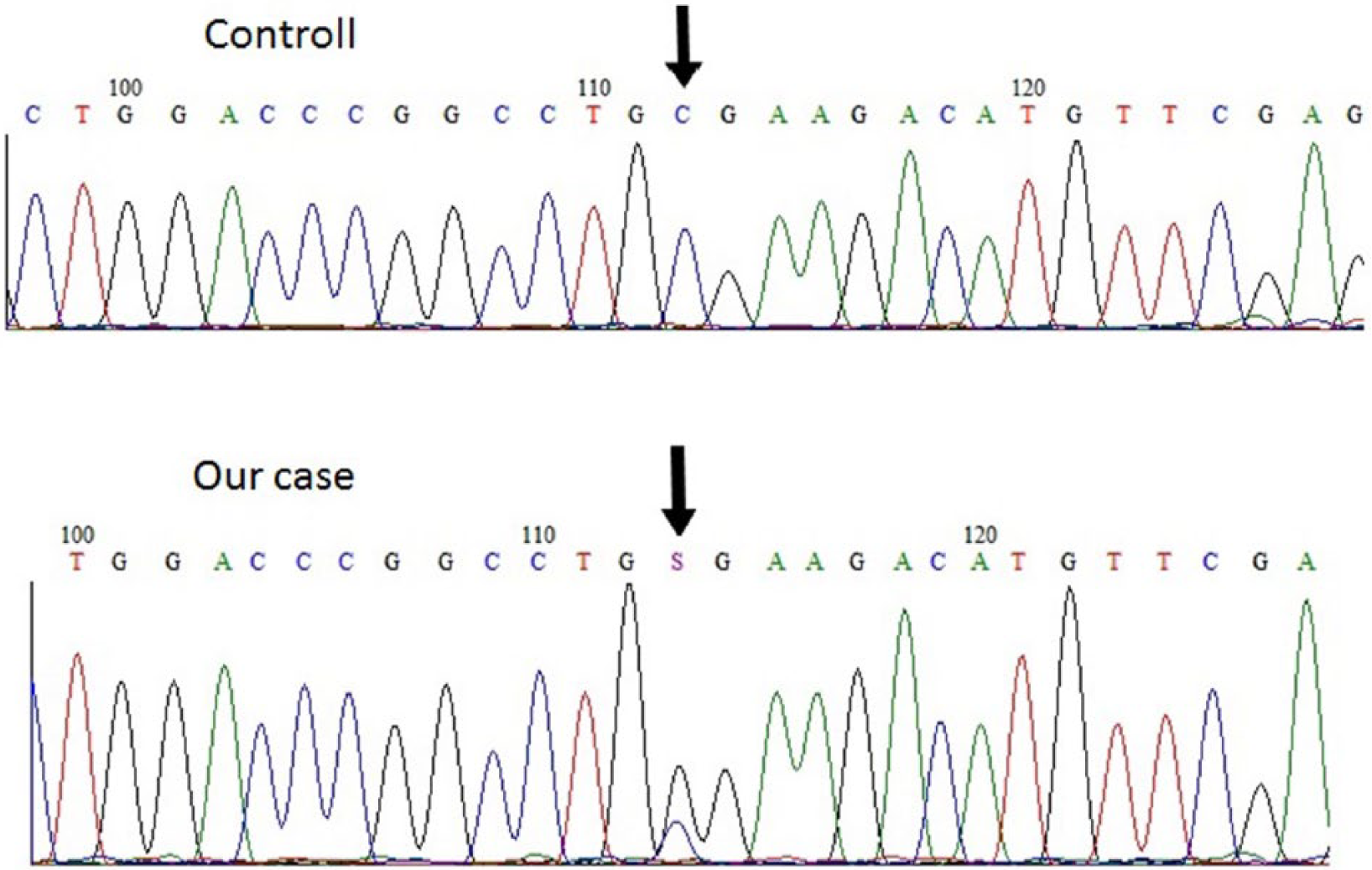
Direct sequencing analysis showed FOXL2 (C402G) mutation in the granulosa cell tumor.
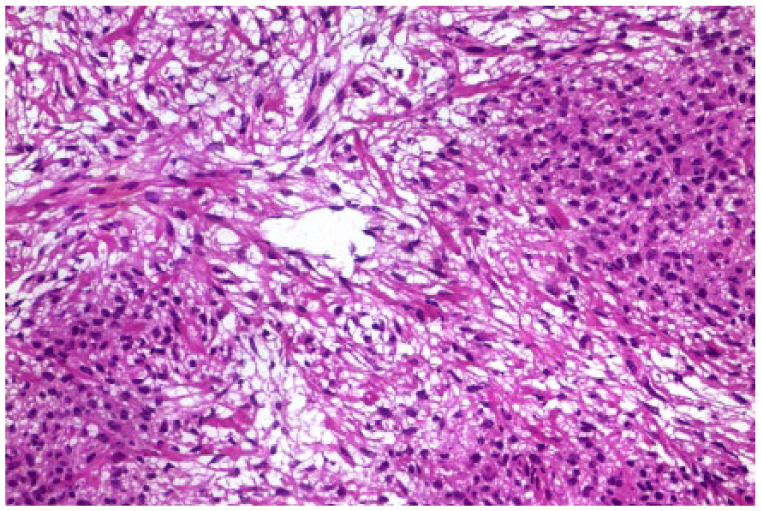
The remaining 30% of the tumor had a different histomorphology. The tumor had round, ovoid nests of epithelial cells resembling transitional epithelium scattered within a densely fibrotic stroma. Some nests were cystic and contained eosinophilic material. Thirty percent of this component had a benign morphology. In these areas the epithelial cells had sharply defined outlines, monomorphic oval nuclei with longitudinal grooves, small or inconspicuous nucleoli, and scant cytoplasm. Mitoses were seen only at the base of the epithelium. Borderline morphology was present in 60% of this tumor component. Epithelial thickening, loss of cell polarity, nuclear hyperchromasia with prominent nucleoli characterized these larger, mostly cystically dilated cell nests (Figure 4). Mitotic figures were seen at all levels of the epithelium. An infiltrative pattern with a diameter of 6 mm was detected. Immunohistochemical staining with laminin was negative around the cell nest (Figure 5). Immunohistochemical staining showed panCK, CK7, CD141, p63, and GATA3 positivity (inset, Figure 4), and PAX8 negativity. This component of the tumor was diagnosed as Brenner tumor (30% benign, 65% borderline) with a malignant area measuring 6 mm in diameter. The ovarian surface was intact. Vascular invasion was not seen. Serous cystadenoma was present in the left ovary.
Epithelial thickening, loss of cell polarity, and nuclear hyperchromasia characterize borderline Brenner tumor (hematoxylin and eosin, ×10); inset showing positive immunohistochemical staining for GATA3 (GATA3, ×4).
Infiltrative pattern of the malignant component of Brenner tumor (hematoxylin and eosin, ×10).
The solid region of tumor suggested malignancy. An intraoperative frozen section was therefore assessed. In the frozen section, only the stromal background was present (Figure 6). Neither adult-type granulosa cell tumor nor Brenner tumor could be seen in this sample. The tumor was therefore diagnosed as thecofibroma.
Within the frozen section, the stromal background of the tumor was present with fibroblasts and theca cells (hematoxylin and eosin, ×20).
We attempted to correlate the histomorphology of the tumor with the clinical behavior: the larger component was the adult-type granulosa cell tumor with solid and trabecular pattern, high nuclear grade, and high mitotic activity. The smaller component contained mostly benign and borderline Brenner tumor with only a small focus of invasion. In our opinion, the adult-type granulosa cell tumor affects the prognosis. Based on histomorphology, tumor recurrence can be expected.
The patient was assessed every 3 months for the first 2 years after surgery. Assessments included clinical assessment (history and physical), laboratory test for tumor markers, and computed tomography scanning. There was no tumor recurrence for 2 years, after which the patient disappeared and we have no further information about her.
Discussion
True mixed tumors of the ovary are uncommon. The definition of these tumors depends on the histogenetic origin of the tumor components. According to the WHO, the presence of 2 or more epithelial cell types in an ovarian epithelial neoplasm, where the minor component constitutes at least 10% of the tumor volume, warrants a designation of mixed epithelial tumor. 2 True mixed carcinomas of the ovary are relatively uncommon. They represent less than 4% of epithelial ovarian tumors. 13 Neuroendocrine tumors associated with an epithelial tumor and endometrioid tumors with squamous differentiation are not included in this definition. 13 The best known are Brenner tumor with a mucinous cystic component; endocervical-like atypical proliferative mucinous tumor exhibiting other epithelial cells of Müllerian derivation; and endometrioid carcinoma admixed with clear cell carcinoma and endometrioid carcinoma with a serous or undifferentiated carcinoma.1,13 In benign and borderline tumors, the mixture of different cell types is not prognostically relevant. 13 The prognosis of mixed malignant tumor depends on the therapeutic sensitivity of the tumor components, especially in advanced stage. Where there is a combination of components with different biological behavior, the treatment and the outcome are affected by the worst prognostic element regardless of the ratio. Mixed germ cell tumors are composed of more than one neoplastic germ cell element. The percentage of the components is irrelevant. 2 The group of mixed sex cord stromal tumors includes Sertoli-Leydig cell tumors and sex cord stromal tumors, NOS (not otherwise specified) according to the new WHO classification. 2 Gynandroblastoma represents a distinct entity, where there is a composition of adult-type granulosa cell tumor and Sertoli-Leydig cell tumor, with the minor component accounting for at least 10% of the tumor volume. 14 The presence of theca cells and fibroblasts in adult-type granulosa cell tumors and the presence of minor sex cord elements in thecoma/fibroma reflects a response of the ovarian stroma to the growth of tumor cells. As such, these are not considered mixed tumors. 14 The differential diagnosis of adult-type granulosa cell tumor from reactive ovarian stromal hyperplasia can be difficult. Molecular testing for the presence of FOXL2 402C→G mutation may improve diagnosis in problematic cases. Somatic mutation in FOXL2 gene has been described as a potential “driver” in the pathogenesis of adult-type granulosa cell tumors. Previous studies have shown that this mutation is specific for the adult-type granulosa cell tumors. It is present in up to 95% to 97% of these tumors.15-17
A combination of tumors with different histogenetic origins is uncommon. For an accurate histopathological report, all morphological subtypes within an ovarian tumor are recommended to be documented with percentages listed. 18 This helps make a more accurate prediction of the clinical behavior of mixed tumors.
Brenner tumor is commonly associated with other tumor types, especially other epithelial neoplasms. Adult-type granulosa cell tumor rarely presents as a component of composite tumors; it occasionally occurs in combination with other sex cord stromal tumors. We reported a case of an unusual mixed ovarian tumor that has not been reported in the literature until now to the best of our knowledge. It was composed of adult-type granulosa cell tumor and Brenner tumor. Seventy percent of the tumor was made up of adult-type granulosa cell tumor and 30% was Brenner tumor. Thirty percent of Brenner tumor was benign, 65% was borderline and an area 6 mm in diameter, which showed features of malignancy.
The histogenesis of mixed epithelial sex cord stromal tumors is uncertain. Three theories are known about the coexistence of mucinous and adult-type granulosa cell tumor. These include a collision tumor with accidentally combined tumor components; heterologous mucinous differentiation within an adult-type granulosa cell tumor; and a granulosa cell element that commenced as reactive stromal hyperplasia within the wall of a preexisting mucinous neoplasm, thereafter progressing to the point of producing a tumor-like mass or neoplastic changes.9,19 In our opinion the histogenesis of the presented mixed Brenner and adult-type granulosa cell tumor is most probably the result of an accidental combination of these tumor components.
From a diagnostic point of view in cases of ovarian neoplasm, it is important to consider the limitations of intraoperative frozen assessment. 20 Ovarian masses are usually of a large size, and sampling of the specimen during intraoperative evaluation is limited. Only 1 or 2 sections can be made and these may not represent all tumor components. As in our case, the frozen section contained only the stromal background of the tumor. Additionally, there are technical difficulties of getting good-quality sections, and furthermore, other supportive methods of evaluation, such as special stains or immunohistochemical stains, are not applied during frozen section examination. 20 The competence of the pathologists and the technician is also very important. Ovarian tumors require careful gross examination and extensive tissue sampling to identify all components of the tumor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.