
Abstract
Vaginal carcinosarcomas (VCSs) are rare and clinically aggressive neoplasms. Primary vaginal malignancies are among the rarest malignant tumors, so clear management guidelines and optimal therapy, especially in the presence of significant pelvic organ prolapse, has not been determined. Here, we present a case of primary VCS closely associated with differentiated squamous intraepithelial neoplasia (DSIN), from which it appeared to have arisen in a postmenopausal patient with complete uterine prolapse. The unusual presentation of our case with DSIN in the adjacent vaginal epithelium with possible diagnostic pitfalls emphasizes the need for systemic presentation of these cases to help pathologists and clinicians know that such lesions can initially present in a patient with complete uterine prolapse. To our knowledge, this is the first case of vaginal DSIN described in the literature to date.
Keywords
Introduction
Carcinosarcomas (CSs) of the female genital tract are rare, very heterogeneous, and clinically highly aggressive neoplasms. Although they can arise in any female genital organ, they are exceptionally rare in the vagina with only 13 documented cases in the literature.1-10 These tumors are composed of 2 distinct epithelial and mesenchymal components, both of which are histologically malignant. The histogenesis of carcinosarcomas is now well established, and they are considered epithelial neoplasms that have undergone sarcomatous transformation. Accordingly, the epithelial component is the main driving force of these tumors.11-14
Differentiated squamous intraepithelial neoplasia (DSIN) has been described as a premalignant lesion with a distinct, human papillomavirus (HPV)-independent pathway in the development of squamous cell carcinoma (SCC) at several anatomical sites, including the vulva, 15 anus 16 and upper aerodigestive tract. 17 The characteristic morphological features of DSIN are thickened epithelium with elongation and anastomosis of rete ridges, keratin pearl formation, and enlarged keratinocytes with large vesicular nuclei and abundant eosinophilic cytoplasm with prominent intercellular bridges. Cytological atypia is characteristically limited to basal and parabasal layers of epithelium. 15 Despite their subtle histological features, DSIN are considered high-grade lesions with greater risk for malignant transformation and shorter time interval for progression to SCC than usual intraepithelial neoplasias driven by persistent high-risk HPV infection.
To the best of our knowledge, vaginal DSIN has not been documented so far. Only 3 cases of primary vaginal carcinosarcomas (VCSs) associated with usual high-grade vaginal intraepithelial neoplasia (VaIN3) have been documented in the literature.4,6,7 Here, we report a case of primary VCS closely associated with DSIN of the adjacent vaginal epithelium, from which it appeared to have arisen in an 86-year-old woman with complete uterine prolapse.
Case Report
An 86-year-old G2P2 woman presented with a third-degree uterine prolapse and a history of sporadic postmenopausal vaginal bleeding for the past 12 months but that had intensified in the past 2 months. The patient had been previously well considering her age, but was known to have complete uterine prolapse for more than 10 years, and her medical history included only hypertension. There was no history of previous gynecological malignancies, and our patient had not received any radiotherapy in the past. Any family history of gynecological or other malignancies was denied.
The uterus was manually repositioned and on vaginal examination, an exophytic mass with contact bleeding involving the right anterolateral wall in the middle third of the vagina was found. The cervix was clinically normal. On bimanual examination, the uterus was normal in size, mobile, painless, and without bleeding. Both adnexa were unremarkable. Transvaginal ultrasound examination revealed a proper-sized anteverted uterus with normal texture and thin, atrophic endometrium, unremarkable adnexa, and no free fluid in the peritoneal cavity. Cervical cytological smear, smear and small biopsy of the vaginal tumor mass were also taken. Cytologists identified only hyperkeratosis in the otherwise normal cervical Pap smear. Smear of the vaginal tumor mass was covered with blood, but necrotic tumor diathesis in the background and rare degeneratively changed atypical squamous cells with signs of keratinization were also detected. A small biopsy of the vaginal tumor mass showed leiomyosarcoma. The patient was admitted to the gynecological oncology department, and after complete workup, she underwent surgery. The abdomen was opened through an infraumbilical midline vertical incision with the extension of the cut 5 cm above the navel. Intraoperatively, organs of the abdominal cavity, uterus, and both adnexa were all macroscopically unremarkable. There was no free fluid in the abdominal cavity, and peritoneal washing was negative. Selective pelvic lymphadenectomy was completed first, followed by Piver-Rutledge-Smith type IV radical hysterectomy, bilateral salpingo-oophorectomy, and omentectomy. Therefore, removal of three-fourths of the upper vagina with full resection of the paracervical tissue up to the wall of the pelvic bone, with no residual tumor mass, was performed.
Pathology
Gross examination of the specimen revealed an exophytic vaginal tumor mass measuring 5 cm in greatest dimension with focal surface ulceration (Figure 1). Cut surface was fleshy, grayish to brown, with areas of necrosis and hemorrhage. Vaginal mucosa adjacent to the tumor seemed to be irregular, slightly raised, and whitish in color.

Vagina, uterus, and adnexa: an exophytic tumor mass with focal surface ulceration involving the right anterolateral wall in the middle third of the vagina.
Microscopic examination showed that the tumor had biphasic morphology with distinctive and separate, but intimately associated, malignant epithelial and mesenchymal components (Figure 2). The epithelial component was a moderately differentiated SCC composed of nests of cells with abundant eosinophilic cytoplasm and intercellular bridges with focal keratin pearl formation (Figures 2D, 2E, and 3D). The mesenchymal component surrounded the epithelial structures and consisted of a dense proliferation of spindle cells with cytological atypia and frequent mitoses, up to 26 mitotic figures per 10 high-power fields (Figures 2D and 2F). No heterologous elements were seen. The tumor deeply infiltrated the muscle layer of the vaginal wall but did not extend beyond it to tunica adventitia. Adjacent vaginal epithelium was thickened with elongation and anastomosis of rete ridges, enlarged keratinocytes with abundant eosinophilic cytoplasm, and prominent intercellular bridges. Furthermore, keratinocytes of the basal/parabasal layers showed cytological atypia with an increased number of mitotic figures (Figure 2C). The tumor was closely associated with previously described changed vaginal epithelium from which it appeared to be arising (Figures 2A-2C and 3A). A panel of immunohistochemical markers was performed. The epithelial component was diffusely and strongly positive for CK5/6 (Figure 3E), EMA, and p63, whereas the sarcomatous component was negative for these markers. On the other hand, the sarcomatous component was diffusely and strongly positive for vimentin (Figure 3F) and SMA, but the epithelial component was negative. Both components were negative for caldesmon, desmin, and p16INK4A. Therefore, the diagnosis of CS of the vagina composed of moderately differentiated SCC and high-grade leiomyosarcoma was made. In addition, p53 and Ki67 showed strong nuclear positivity in the basal and parabasal layers of the closely associated vaginal epithelium, with both CS components also being diffusely positive for p53, so the diagnosis of DSIN was also made (Figures 3B and 3C).
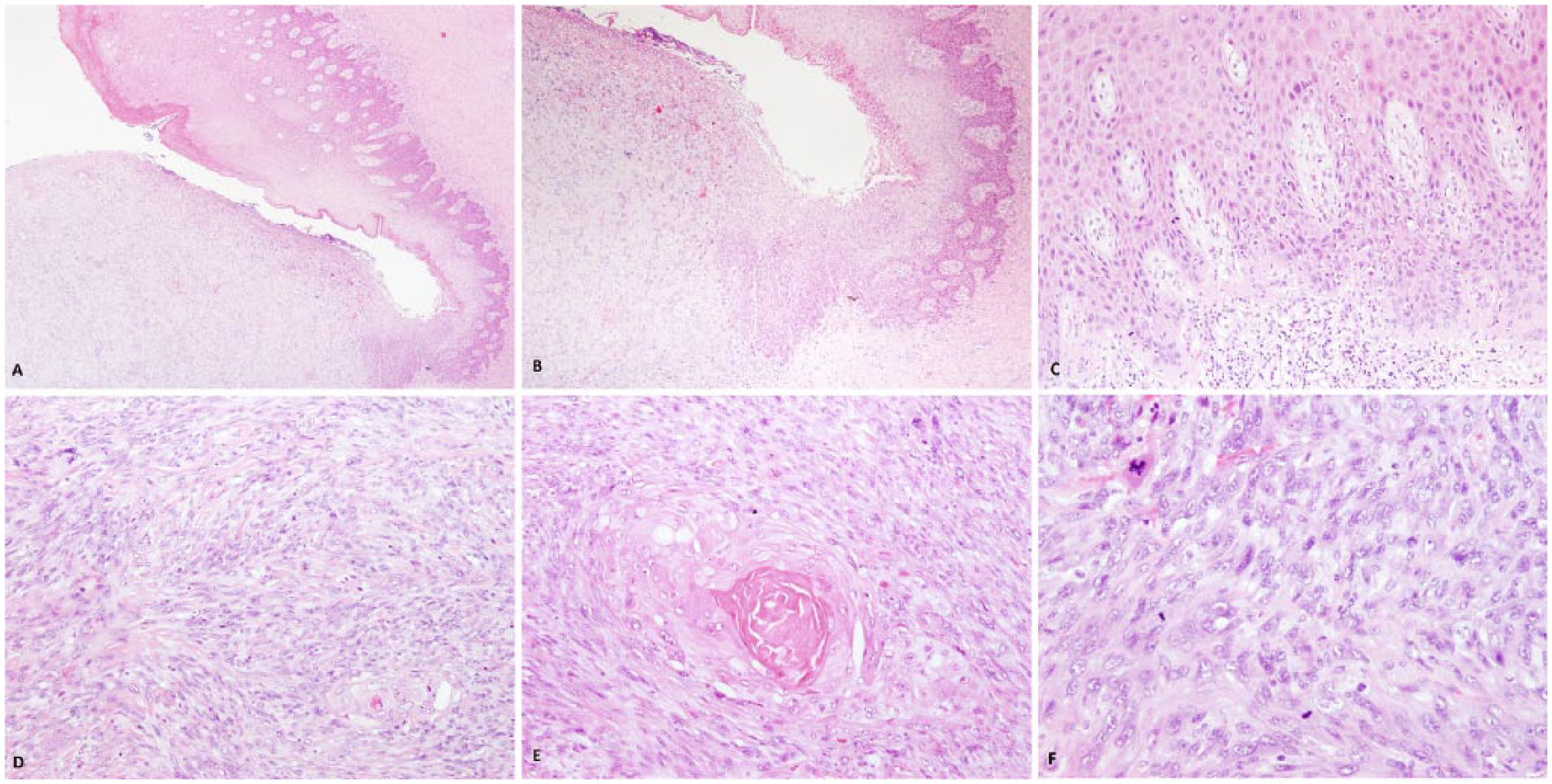
Microscopic features of the resected tumor and adjacent vaginal epithelium. The tumor was closely associated with vaginal epithelium that was thickened with elongation and anastomosis of rete ridges, from which it appeared to be arising; hematoxylin and eosin (HE), 20× (A) and 40× (B). Keratinocytes of the basal/parabasal layers showed cytological atypia with increased number of mitotic figures, suprabasal enlarged keratinocytes with abundant eosinophilic cytoplasm and with prominent intercellular bridges; HE, 200× (C). Biphasic morphology of the resected tumor with distinctive malignant epithelial and mesenchymal component; HE, 100× (D). The epithelial component was moderately differentiated squamous cell carcinoma composed of nests of cells with focal keratin pearl formation; HE, 200× (E). The mesenchymal component consisted of dense proliferation of spindle cells with cytological atypia and frequent mitoses; HE, 400× (F).
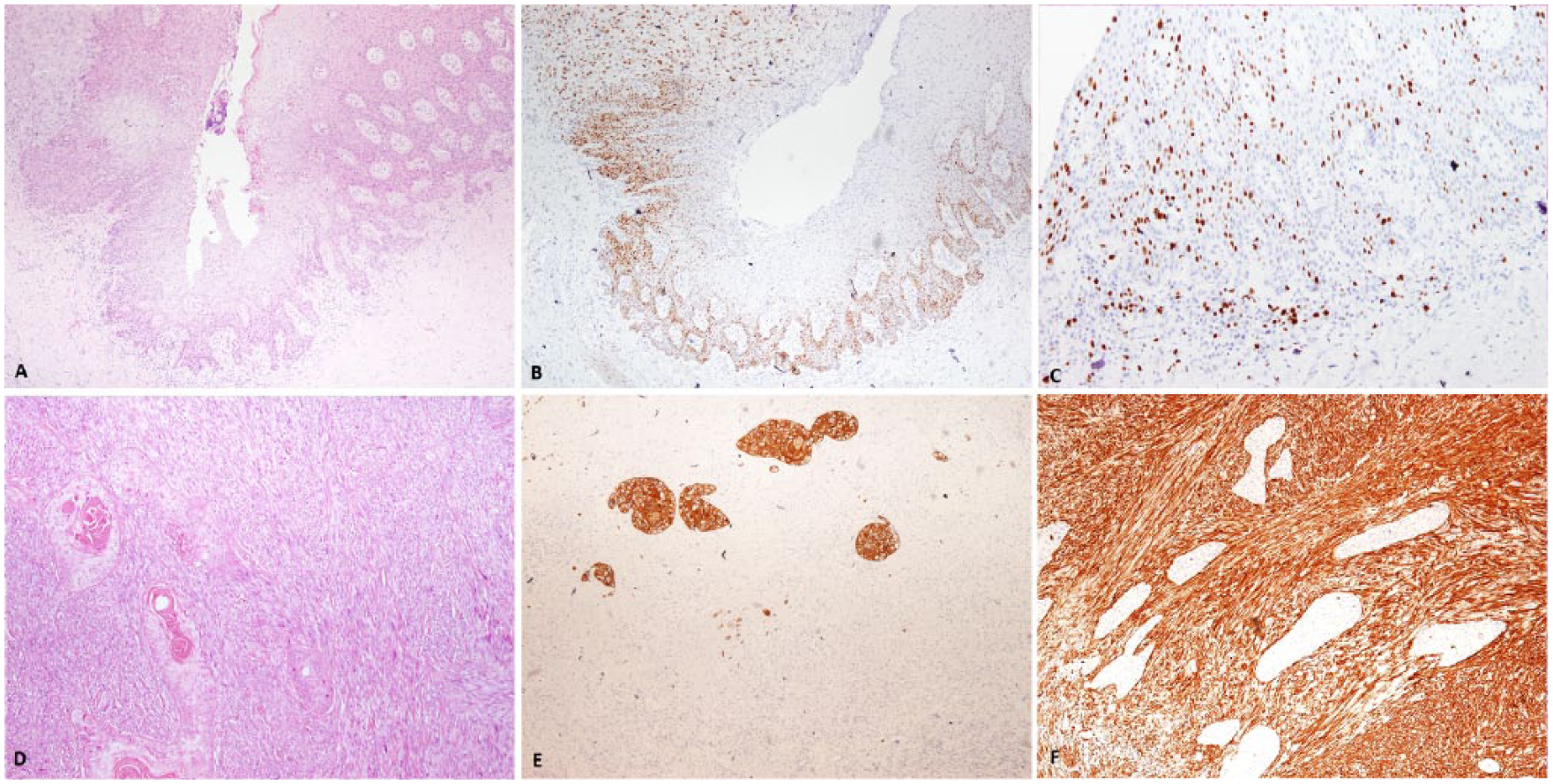
Histological and immunohistochemical characteristics of the resected tumor and associated vaginal DSIN. Vaginal DSIN in close association with the biphasic tumor from which the tumor seems to be arising; hematoxylin and eosin (HE), 100× (A). Immunohistochemical staining for p53 protein showed positive cells extending above the basal layer into higher levels of the DSIN lesion and also diffuse nuclear p53 expression in both tumor components; 100× (B). Immunohistochemical staining for Ki67 showed strong nuclear positivity in the basal and parabasal layers of the vaginal DSIN lesion; 200× (C). Biphasic morphology of the resected tumor with moderately differentiated squamous cell carcinoma composed of nests of cells with abundant eosinophilic cytoplasm and intercellular bridges with focal keratin pearl formation surrounded with dense proliferation of spindle cells with cytological atypia and frequent mitoses; HE, 40× (D). Immunohistochemical staining for CK5/6 showed diffuse and strong positivity in the epithelial component of tumor; 100× (E). Immunohistochemical staining for vimentin showed diffuse and strong positivity in the sarcomatous component, whereas epithelial nests of cells were negative; 100× (F).
The uterus, adnexa, omentum and pelvic lymph nodes were all negative for the disease, as well as resection margins. Based on these findings, the disease was staged according to the International Federation of Gynecology and Obstetrics system as stage I.
Follow-up
The postoperative course was uneventful. In agreement with the patient, considering her age and excellent performance status, the patient was advised against adjuvant chemotherapy or radiotherapy. She was further advised to have regular follow-up examinations every 3 months during the first year after surgery, and then every 6 months at the gynecological oncology outpatient department (OPD). The patient presented for the first 2 follow-ups at the OPD and was feeling well without evidence of the disease; then, she decided to continue regular check-ups at her general practitioner. At 14 months after the surgery, the patient is alive with no evidence of the disease.
Discussion
The morphological, clinical, and treatment details of previously reported primary VCSs are shown in Table 1. Several studies have reported that vaginal cancers are most often located in the posterior wall in the upper third of the vagina. In addition, tumor localization is a prognostic parameter, with better outcomes for those with lesions in the upper third of the vagina.8,18,19 Contrary to these data, primary VCSs were located in the lower two-thirds of the vagina in 6 out of 9 reported cases: that is, 3 tumors were in the lower third, 3 tumors were in the middle third, and 3 other tumors were occupying the entire length of the vagina, with predilection for the anterior vaginal wall (5 vs 1; Table 1).
Morphological, Clinical, and Treatment Details of the Reported Cases of Primary CS of the Vagina.
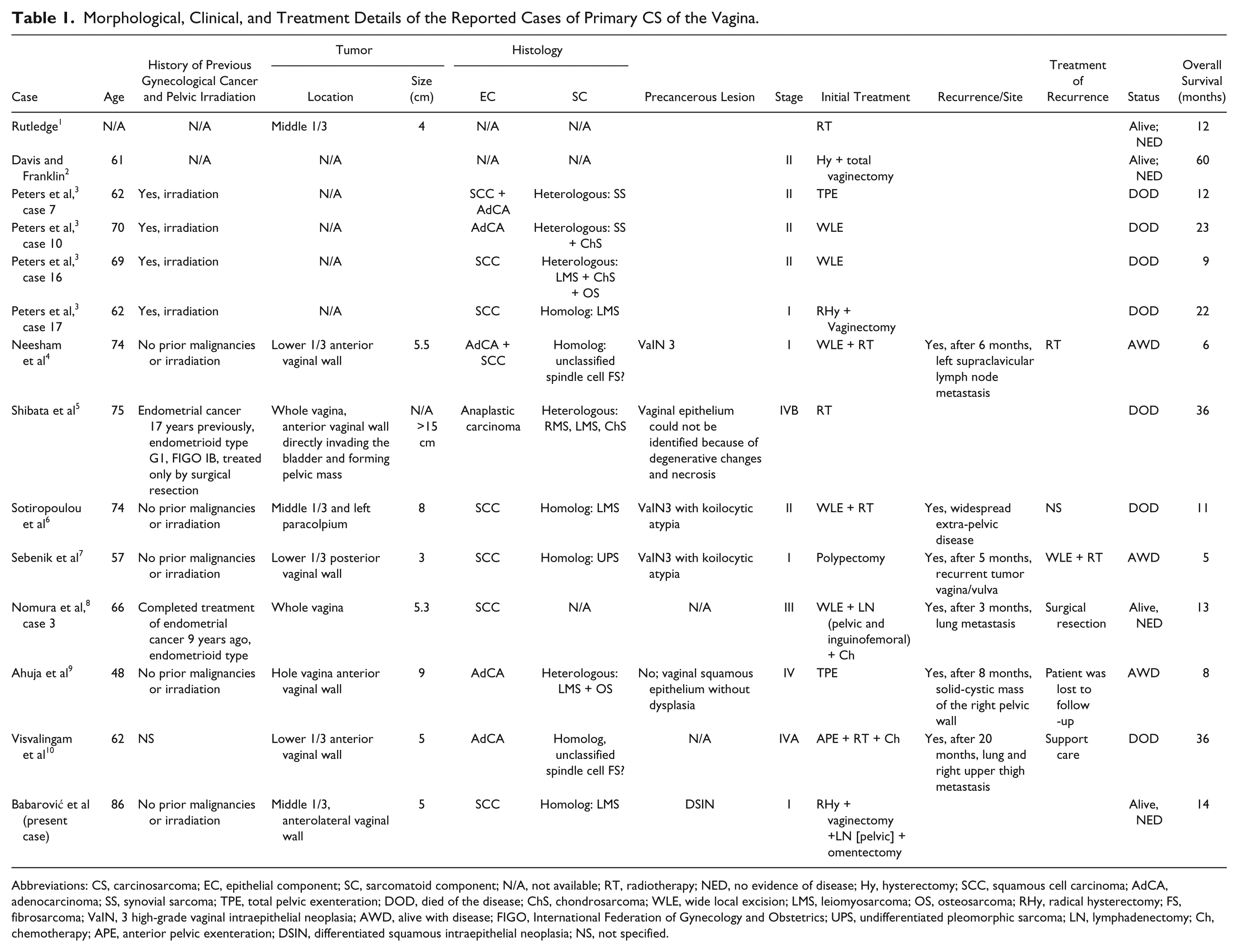
Abbreviations: CS, carcinosarcoma; EC, epithelial component; SC, sarcomatoid component; N/A, not available; RT, radiotherapy; NED, no evidence of disease; Hy, hysterectomy; SCC, squamous cell carcinoma; AdCA, adenocarcinoma; SS, synovial sarcoma; TPE, total pelvic exenteration; DOD, died of the disease; ChS, chondrosarcoma; WLE, wide local excision; LMS, leiomyosarcoma; OS, osteosarcoma; RHy, radical hysterectomy; FS, fibrosarcoma; VaIN, 3 high-grade vaginal intraepithelial neoplasia; AWD, alive with disease; FIGO, International Federation of Gynecology and Obstetrics; UPS, undifferentiated pleomorphic sarcoma; LN, lymphadenectomy; Ch, chemotherapy; APE, anterior pelvic exenteration; DSIN, differentiated squamous intraepithelial neoplasia; NS, not specified.
Although previously considered as subtypes of sarcoma, the histogenesis of CSs has been the subject of discussion, and there is now substantial evidence for its epithelial origin.7,11-14 In their case study of 8 cervical CSs, Grayson et al 14 found in situ SCC in 7 cases and also detected HPV type 16 in both epithelial and sarcomatous tumor components. Likewise, Sebenik et al 7 detected localization of the integrated high-risk HPV DNA in both tumor components of the vaginal counterpart and also found VaIN3 with koilocytic atypia adjacent to the tumor. Two additional reports have also described high-grade VaIN3 lesion in the adjacent mucosa of the primary VCS,4,6 and our case was associated with vaginal DSIN from which it appeared to have arisen. Additionally, immunohistochemical staining for the tumor suppressor p53 protein showed positive cells extending above the basal layer into the higher levels of the DSIN lesion, and both components of our patient’s tumor also showed diffuse nuclear p53 expression. All these findings support the so-called metaplastic theory of origin with epithelial component as a driving force of CSs.
We also performed immunohistochemical staining with p16INK4A, and the tumor along with adjacent vaginal mucosa was completely negative. Positive p16INK4A immunostaining is an indirect marker of high-risk HPV infection because the expression of the HPV E7 oncogene leads to inactivation of pRb and consequent overexpression of p16INK4A. According to the study by Alonso et al, 20 patients with HPV-negative vaginal carcinomas had poorer prognosis than HPV-positive patients. Moreover, Hellman et al 21 demonstrated in their study that immunohistochemistry by p16INK4A could be a marker for diagnosis of HPV-positive primary vaginal carcinomas as well as a prognostic marker. Despite our increased knowledge of the biological potential and even different pathogenic pathways of some other intraepithelial neoplasias such as vulvar intraepithelial neoplasia (VIN), the natural course, true malignant potential, and optimal therapeutic approach with recommended surveillance of VaIN remain unknown. However, the lack of knowledge is certainly associated with rarity of this intraepithelial neoplasia, which accounts for less than 1% of all intraepithelial neoplasias of the female genital tract. The question arises as to what is the premalignant lesion of the HPV-negative vaginal carcinomas? Modeled on vulvar cancer, our hypothesis is that there are 2 different pathways leading to vaginal cancer, with different premalignant lesions. The HPV-related pathway is preceded by classic VaIN, whereas the HPV-independent pathway could be preceded by DSIN, which is probably primarily driven by TP53 mutations. Chronic inflammatory injuries and local chronic irritation of the vaginal wall by prolonged uterine prolapse, pessary use, and urine leakage might be the main etiological factors for these HPV-independent vaginal cancers. Additional studies are needed to confirm this possible association and also to establish the strength of this link.
Although a causal association remains to be proven, we feel that clinicians should be mindful of the possibility of vaginal DSIN when managing patients with a long history of uterine prolapse. Histologically, recognition of DSIN is hindered by a high degree of cellular differentiation combined with the absence of widespread architectural disarray, nuclear pleomorphism, and diffuse nuclear atypia. Additionally, it should be noted that in DSIN, atypia is strictly confined to the basal and parabasal layers of the epithelium. Therefore, cytological diagnosis on smear is very difficult or virtually impossible, so biopsy of the lesion is highly required. The optimal biopsy should include the interface between the lesion and normal mucosa, if possible.
Primary vaginal malignancies are among the rarest malignant tumors. As a result, the natural course of the disease, clear management guidelines, and optimal therapy, especially in the presence of significant pelvic organ prolapse, have not been determined. Because of the anatomy of the region and close proximity of the vagina to critical pelvic structures such as the bladder, urethra, and rectum, surgery has a limited role in the management of vaginal carcinoma. 22 Radiation therapy, including brachytherapy and external beam radiation, is the standard modality of treatment.23,24 Nevertheless, some authors have advocated radical surgery with or without associated radiotherapy as a therapeutic option in properly selected patients.25-28 The role of adjuvant radiotherapy and chemotherapy is still unclear.
In our case, therapeutic approach and treatment planning were complicated because of total uterine prolapse. Brachytherapy was not technically feasible, and we were also concerned that the bladder, colon, and rectum might receive higher exposure to the radiation field in our patient. Our patient was medically fit and in the early stage of the disease, so our therapeutic approach was radical surgery. Equally, the initial treatment of previously reported cases of primary VCS was surgical in 11 cases; surgery alone was performed in 7 cases, surgery in combination with radiotherapy in 2 cases, surgery with radiotherapy and chemotherapy in 1 case, and surgery in combination with chemotherapy in 1 case (Table 1). VCSs are aggressive neoplasms. Of the previously reported 13 cases, 7 died from the disease, whereas 3 patients were alive but with recurrent disease at 6, 5, and 8 months of follow-up, respectively. One of these patients had supraclavicular lymph node metastasis, which was treated by radiotherapy; 1 patient had a recurrent vulvo/vaginal mass treated by wide local resection followed by radiotherapy; and 1 patient was lost to follow-up with a large pelvic tumor mass. In addition, there was 1 patient who developed lung metastasis 3 months after initial treatment. Solitary lung metastasis was treated by surgical resection, and this patient was alive without evidence of the disease after 13 months. 8 Our patient is alive without evidence of the disease after 14 months, and there are only 2 more patients who are alive and well after 12 and 60 months.
Conclusions
The rarity of primary VCSs and the unusual presentation of our case with DSIN of the adjacent vaginal epithelium, with possible diagnostic pitfalls, points to the need of systemic presentation of these cases to help pathologists and clinicians know that such a lesion can initially be present in a patient with complete uterine prolapse. The aggressive nature of this disease demands careful follow-up of these patients, and because of the rarity of the condition, appropriate strategies of treatment remain to be determined. Surgery followed by radiotherapy is the currently favored management modality, although the prognosis is very poor even after treatment.
Footnotes
Acknowledgements
We would like to express our gratitude to Professor Nives Jonjić for her valuable and helpful comments on manuscript. We thank Renata Grabar and Ozren Štanfel for their excellent technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has not been supported by private or public sources, grants, or funds.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Trial Registration
Not applicable, because this article does not contain any clinical trials.