
Abstract
Simultaneous presence of pancreatic serous cystic neoplasms and neuroendocrine neoplasms is rare. We present a case with the incidental finding of a duodenal neuroendocrine tumor (NET) with 2 lymph node metastases in a Whipple resection specimen performed to remove a pancreatic cystic neoplasm that postoperatively turned out to represent a serous cystic neoplasm (SCN). The patient was a 75-year-old female. She presented with loss of appetite and weight. Preoperative contrast-enhanced computed tomography scan of the abdomen showed a multicystic lesion in the head of pancreas. On histologic examination of the resection specimen, a pancreatic SCN was found, and in addition in 2 peripancreatic lymph nodes, metastases from a NET. Further examination of the resected specimen revealed a duodenal NET. Review of the literature revealed only one prior study with 4 cases of pancreatic SCN associated with a duodenal NET. In 1 of the 4 cases, the patient had von Hippel-Lindau disease. Our report emphasizes the importance of careful examination of pancreatic resection specimens including the peripancreatic lymph nodes also when dealing with SCNs, as coexisting and more malignant tumors may otherwise be missed.
Introduction
Serous cystic neoplasms (SCNs) of the pancreas account for between 10% and 16% of cystic pancreatic tumors and are considered benign neoplasms with very rare malignant potential.1-5 Most SCNs represent serous cystadenomas. The reported frequency of serous cystadenocarcinoma ranges from 0.1% to 3%.6,7 However, when causing symptoms, surgical resection is recommended also for serous cystadenomas.2,6-8 Neuroendocrine neoplasms (NENs) of the duodenum are relatively rare, representing only 2.5% of all gastroenteropancreatic (GEP) NENs in a recent study from Norway. 9
We report a case of SCN associated with a duodenal neuroendocrine tumor (NET) that already had metastasized to 2 peripancreatic lymph nodes in a patient without any signs of von Hippel-Lindau (VHL) disease. Moreover, we reviewed the literature on previously reported cases of SCN associated with NEN of the pancreas, duodenum, or ampulla of Vater. SCNs have rarely been described in association with other pancreatic neoplasms such as pancreatic adenocarcinomas and NENs.10-12 However, we were able to identify only one previous publication reporting SCN associated with a duodenal NEN. This was a retrospective analysis of 193 SCNs, 4 of whom were associated with a duodenal NEN. 13 Of these 4 cases, one patient had VHL disease. 13 Hence, this is only the second publication on the association of SCN and duodenal NEN. Interestingly, this is the first report of SCN associated with metastasizing duodenal NEN. Our report emphasizes the importance of careful examination of pancreatic resection specimens including the peripancreatic lymph nodes also when dealing with SCNs, as coexisting and more malignant tumors may otherwise be missed.
Case Report
A 75-year-old female presented with loss of appetite and weight. A contrast-enhanced computed tomography (CT) of the abdomen showed a multicystic lesion in the head of pancreas, suspicious of SCN. A Whipple resection was performed. The head of pancreas measured 5 × 5 × 4 cm and contained a multicystic lesion measuring 4 × 3.5 × 3.5 cm (Figure 1A). The patient had no history of gastritis, and no ulcers were found in the antrum or duodenum at macroscopic evaluation. Microscopically, the multicystic nature of the lesion was confirmed. The single cysts measured between 0.1 and 9 mm in diameter (Figure 1B-C). They were lined by cuboidal epithelial cells with a glycogen-rich cytoplasm lacking any atypia. The cysts were separated by fibrous septa. The epithelial cells lining the cysts showed positive immunohistochemical reaction for VHL gene product (pVHL) (Figure 1D). The diagnosis of a pancreatic SCN was made. According to the definition by Reid et al, the SCN was of the classical microcystic type. 13 The patient was not specifically examined for VHL after receiving the SCN diagnosis. However, she did not have any prior history of VHL, such as hemangioblastoma of the central nervous system or retina, and at contrast-enhanced CT prior to pancreatic surgery, no renal or hepatic tumors were found. Also, at surgery there were no abnormalities related to the broad ligament of the uterus. Our protocol states that a minimum of 15 lymph nodes should be examined, as long as the presence of a malignant neoplasm has not been excluded. In this case, a total of 14 lymph nodes were identified, and in 2 of them, lesions measuring 1.5 and 2.5 mm consisting of rounded nests of uniform epithelial tumor cells with small round nuclei and eosinophilic cytoplasm were found (Figure 2A). At immunohistochemistry, these cells were positive for synaptophysin (Figure 2B), chromogranin A, CKAE1/3, CDX2, cadherin-17, gastrin, islet-1 (Figure 2C), CK7 (focally), and serotonin (a few scattered cells), supporting their neuroendocrine phenotype. The tumor cells were negative for CK20, insulin, glucagon, pVHL, and somatostatin. The Ki67 proliferation index was 0.5%. Hence, these lesions represented lymph node metastases of a NET of unknown primary. Multiple sections from the SCN were examined without any evidence of a NET. As the NET tumor cells expressed gastrin, a duodenal or gastric primary was suspected. Hence, a supplementary dissection of the ampullary region, duodenum, and antrum was performed. Macroscopically, an area with a light grey color, measuring around 4 mm, was identified in the duodenal mucosa close to the ampulla of Vater. The lesion was submitted for microscopy, together with additional multiple sections from the periampullary region. At microscopy of these additionally examined sections, a 4 mm NET was found in the duodenal mucosa, clearly separate from the pancreatic SCN that did not permeate the tunica muscularis of the duodenum (Figure 2D). The duodenal NET was located within the submucosa and lamina propria and surrounded by Brunner’s glands. A minimum distance of 6 mm was measured between the tumor and the SCN. The NET was well circumscribed and consisted of uniform eosinophilic cells with uniform nuclei. The Ki67 proliferation index was 1%. The tumor cells showed expression of CKAE1/3, CK7, synaptophysin (Figure 2E), chromogranin A, CDX2, islet-1 (Figure 2F) and cadherin-17. There were a few serotonin- and somatostatin-positive tumor cells, while the majority strongly expressed gastrin. There was no expression of pVHL (Figure 2G). Overall, the immune profile was identical to the lymph node metastases, supporting the diagnosis of a duodenal NET grade 1, measuring 4 mm in greatest dimension and metastatic to 2 peripancreatic lymph nodes (Table 1). No vascular or neuronal invasion was seen. At our institution, we routinely sample the ampulla and submit at least on section from this region for microscopy. We cut the surgical specimen into slices with a thickness of as close to 3 mm as possible. However, in this specific case, the original slice later found to contain a duodenal NET had a thickness of around 7 mm. The resident performing the original dissection was possibly biased due to the presence of a large, multicystic tumor. This may have contributed to that the NET was not observed at the initial evaluation of the surgical specimen.
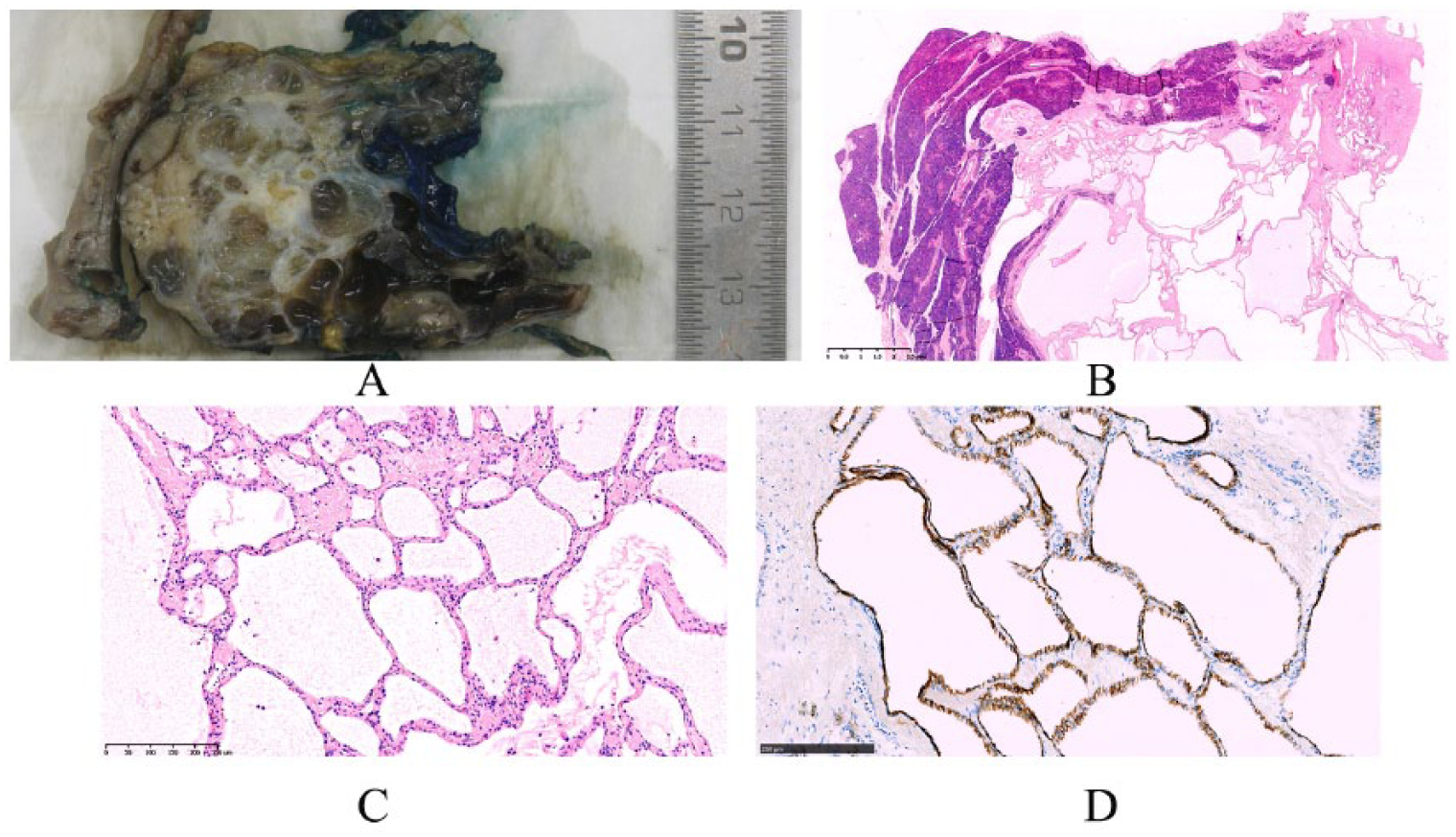
Morphological features of a pancreatic serous cystic neoplasm (SCN), microcystic type, in a patient with synchronous neuroendocrine tumor of the duodenum. (A) Macroscopically, numerous cysts of different size are shown. (B) At microscopy, small cysts of varying size separated by fibrous septa, partly surrounded by normal pancreatic tissue, are appreciated (hematoxylin and eosin [H&E]). (C) Larger magnification of “B” showing numerous cysts, each measuring less than 1 mm in diameter (H&E). (D) The SCN is pVHL-positive (pVHL immunostaining).
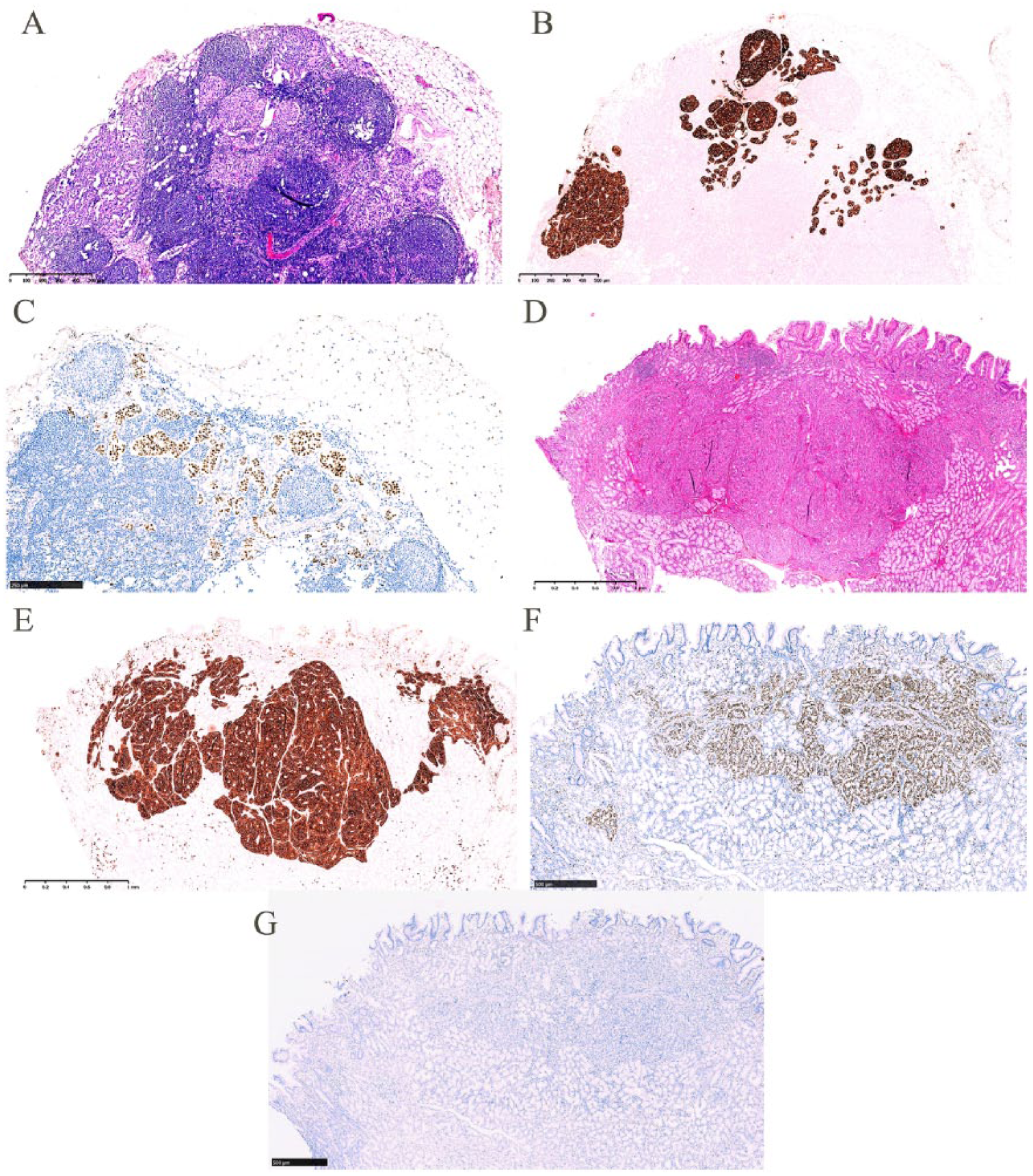
Histological and immunohistochemical features of a lymph node metastasis (A, B, C) originating from a duodenal neuroendocrine tumor (NET; D, E, F, G) in a patient with synchronous pancreatic serous cystic neoplasm. (A) Lymph node with metastatic NET cells, forming small nests (hematoxylin and eosin [H&E]). (B) Strong expression of synaptophysin in the metastatic NET (synaptophysin immunostaining). (C) Islet-1 expression in the metastatic NET. (D) Primary NET in the duodenal submucosa, surrounded by Brunner’s glands (H&E) showing (E) synaptophysin and (F) islet-1 expression. (G) The duodenal NET is pVHL-negative (pVHL immunostaining).
Summary of Reported Cases of Synchronous Pancreatic Serous Cystic Neoplasm (SCN) and Pancreatic or Duodenal Neuroendocrine Neoplasm (NEN) in Patients Without Evidence of von Hippel-Lindau Disease.
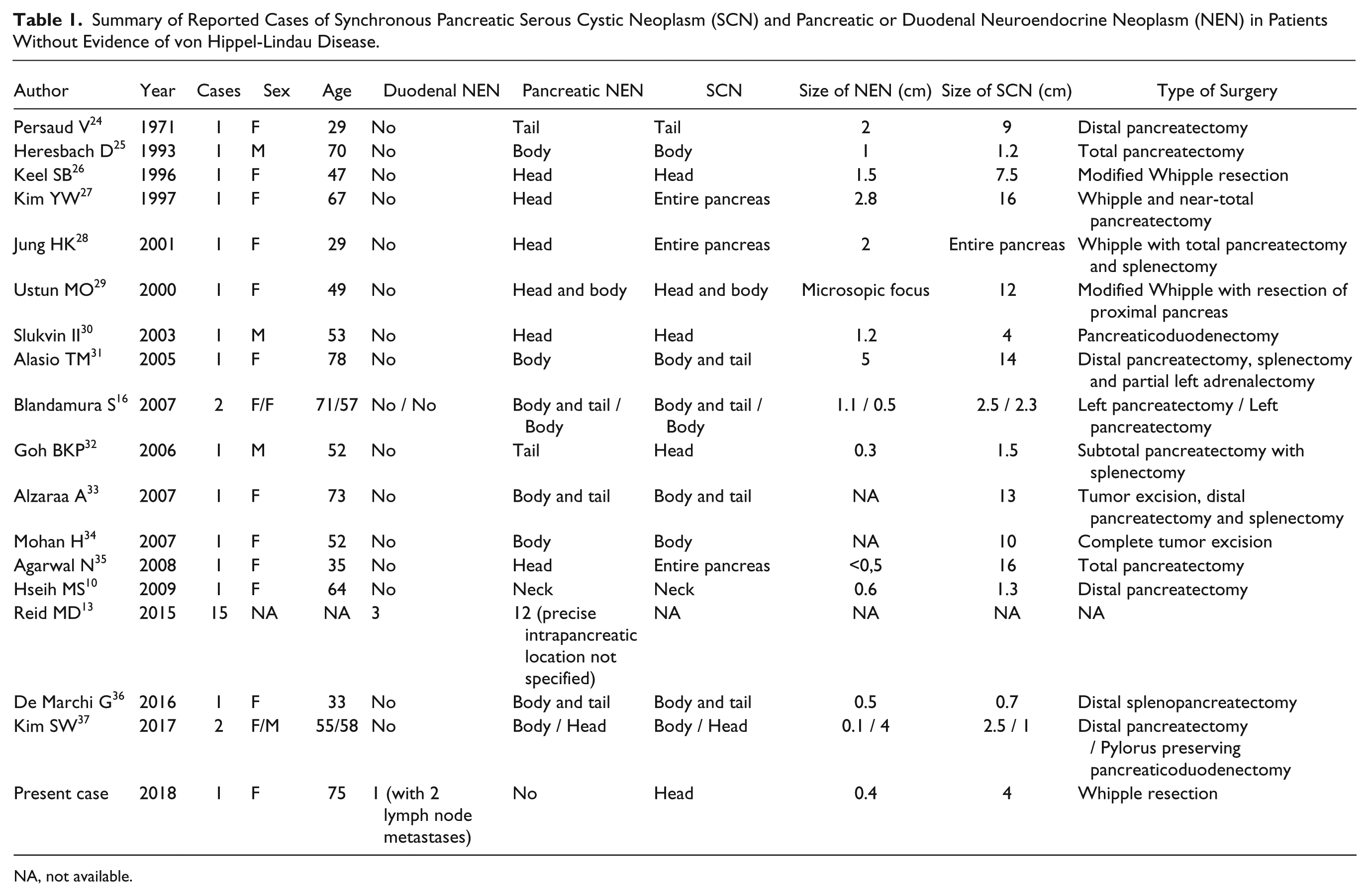
NA, not available.
Discussion
NENs of the duodenum are rare, and constituted, in a recent epidemiological study from Norway, 9 only 2.5% of all GEP-NENs. 9 Ampullary NENs represent only about 20% of duodenal NENs, hence accounting for less than 1% of all GEP-NENs. 14 The case presented here emphasizes that a pancreatic SCN, a usually benign lesion, can be associated with clinically inapparent synchronous NENs not only of the pancreas but also of the duodenum. To our knowledge, this association has only been reported in one previous English-language publication. 13
A PubMed search using the terms “pancreas” together with “serous cystic neoplasm,” “serous cystadenoma and neuroendocrine tumor,” “neuroendocrine neoplasm,” and “neuroendocrine carcinoma” was performed. A review of the identified literature revealed that the association of pancreatic SCN with a pancreatic, duodenal, or ampullary NEN had been reported 69 times. The vast majority of these cases were located in the pancreas (n = 64), followed by the duodenum (n = 4) and ampulla of Vater (n = 1). The 4 SCNs associated with a duodenal NEN were all reported in the same publication by Reid et al. 13 The ampullary NEN associated with pancreatic SCN was also associated with multiple pancreatic NENs. 15 Approximately half of the reported cases of synchronous pancreatic SCN and NEN were in patients with VHL disease (n = 36).10,13,15-23 We found 33 published cases of pancreatic SCN coexisting with pancreatic (n = 30) or duodenal (n = 3) NEN in patients without VHL disease (Table 1).10,13,16,24-37 These NENs were located in the head, body, or tail of the pancreas. Of the reviewed literature, most publications were case reports with 1 or 2 cases. One large series described a cohort of 193 pancreatic SCNs in order to elucidate the different morphological variants of SCNs and the frequency and nature of serous cystadenocarcinoma. 13 In a study by Kim et al, a total of 274 resected SCNs were reviewed. Fifteen cases showed association with another pancreatic neoplasm, and 6 of these were NENs, two in patients without evidence of VHL disease. 37 It was not reported if the NENs had metastasized. Hence, this seems to be the first English-language report of the association of pancreatic SCN with metastasized duodenal NEN. The duodenal NET in our case measured only 4 mm in greatest dimension but had already metastasized to 2 peripancreatic lymph nodes.
It is not clear whether synchronously developing neoplasms originate from 2 different neoplastic cell lines or from the same precursor cell. In the reviewed literature, 2 main hypotheses for concurrent SCN and intrapancreatic NEN are proposed. It is possible that the intrapancreatic NENs associated with SCNs arise from the same stem cell through biphasic differentiation.26,38 Another hypothesis proposes coincidental neoplastic change in 2 different cell types, and in some cases, the 2 tumors simply become admixed due to close proximity (collision tumors).10,27 As the 2 tumors described in our case, however, clearly were located separately, they most likely arose from 2 different neoplastic precursor cells. Besides, the NET showed loss of pVHL while the SCN was pVHL-positive, in accordance with the literature on these entities. 39 The duodenal gastrin-producing NET likely arose from gastrin-producing G cells of the duodenal mucosa, 40 whereas SCNs are thought to originate from pancreatic centroacinar or intercalated duct cells.41,42
In conclusion, this is the first report of a pancreatic SCN synchronous with a metastasizing duodenal NEN. It emphasizes the importance of careful examination of pancreatic resection specimens including the peripancreatic lymph nodes also when dealing with SCNs, as coexisting and more malignant tumors may otherwise be missed.
Footnotes
Author(s) note
Sönke Detlefsen is also affiliated to Odense Pancreas Center (OPAC), Odense University Hospital, Odense, Denmark.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.