
Abstract
Background. Adrenal rest (AR) is the presence of ectopic adrenal cortical tissue, often identified incidentally during autopsy (20% of postmortem examination). In the kidney, AR can be found in 6% of the general population. Ectopic adrenal tissue is of no functional significance but may in some cases, pose a diagnostic challenge for the pathologist, especially in the context of renal clear cell renal cell carcinoma (RCC) and small needle biopsies. Aim. To investigate the utility of immunohistochemical stains in distinguishing AR from RCC. Methods. Archival cases of AR, in our institution, were reviewed and compared with a cohort of RCC cases using a panel of immunohistochemical stains, including PAX2, PAX8, calretinin, and inhibin. Results. Nine of 10 (90%) cases of AR showed positive staining for inhibin and negative staining for calretinin, PAX2 and PAX8. One AR case was positive for PAX2 and PAX8 in addition to inhibin. All (100%) RCC cases were positive for PAX2 and PAX8, but negative for inhibin and calretinin. Conclusions. A panel of PAX2, PAX8 and inhibin may be useful markers for distinguishing AR from RCC. Calretinin was noncontributory in our study.
Introduction
The morphologic similarity between adrenal rest (AR) cells and renal cell carcinoma (RCC) has been well established ever since Grawitz introduced the term “hypernephroma” in 1883 to describe clear cell RCC, which was believed to be derived from “hypernephroid” (heterotopic adrenal rests) within the kidney. 1 The fact that these 2 tissues share those similarities makes it harder to distinguish them apart based solely on morphologic features. 1 Some of the stains often used to separate these entities include epithelial membrane antigen (EMA), cytokeratin, vimentin, melan-A, CD10, inhibin, and RCC marker. Unfortunately, due to inconsistent staining patterns observed with these antibodies, the reliability of this panel has been questioned. 1
The adrenocortical primordium (thickening of the coelomic mesothelium) forms by the invagination of the coelomic epithelium, proximate to the arising site of the gonadal blastema, roughly around the 30th day of gestation. Fragments of adrenocortical tissue might scatter along the descending path of gonadal migration and form ectopic adrenal glands.2,3 Even though the majority of these fragments settle in the vicinity of the adrenal gland or along its migratory course, in rare cases, ectopic adrenal tissue is found at distant sites.4,5
In this study, we observe the clinical features of ectopic AR tissue in the kidney and investigate the utility of immunohistochemical stains in distinguishing AR from RCC by using a panel of PAX2, PAX8, inhibin and calretinin.
Methods
Pathology files at Wake Forest Baptist Health were reviewed for AR cases in kidney from 2004 to 2015. Ten cases of AR and 10 cases of RCC, from the same period, were selected for the study. Clinical presentation, gross, and microscopic features, as well as patterns of immunohistochemical staining using a panel of immunostains (PAX2, PAX8, calretinin and inhibin) were reviewed.
Immunohistochemistry
Immunohistochemistry was performed using PAX2, PAX8, inhibin, and calretinin antibodies (Table 1) on the automated Leica Microsystem Bond III platform using their Polymer Refine DAB kit. The pretreatments ER2 (epitope retrieval solution-2) were supplied by Leica (Leica Biosystems Newcastle Ltd, Newcastle upon Tyne, UK). The evaluation was performed by 3 pathologists (MQY, ZTS, and SAQ), independently. Any appropriate staining above 5% of lesional cells was considered positive. In one case with interobserver variability, the case was reviewed by the group on a multiheaded microscope and a consensus was reached.
Antibody Sources, Dilution, and Retrieval Methods.

Results
Patients diagnosed with AR ranged in age from 17 to 76 years (mean = 54.3 years), with a 1:1.5 male to female ratio, and tumor sizes ranging from 0.4 to 1.6 cm (mean = 0.86 cm). Patients diagnosed with RCC ranged in age from 42 to 79 years (mean = 60.7 years), with a 1.5:1 male to female ratio, and tumor sizes ranging from 2.1 to 8.1 cm (mean = 4.16 cm). AR cases were found in the upper pole and subcapsular in 5 cases and the lower pole in 3 cases. In 2 of the 10 AR cases, the location of the lesion was not specified. RCC cases were found in the upper pole in 4 cases, in the middle pole in 2 cases, lower pole in 1 case, and the location for the remaining cases was not specified (Table 2).
Characteristics of Patients With Intrarenal Ectopic Adrenal Tissue Versus Clear Cell RCC, Including the Results of Immunohistochemical Studies.
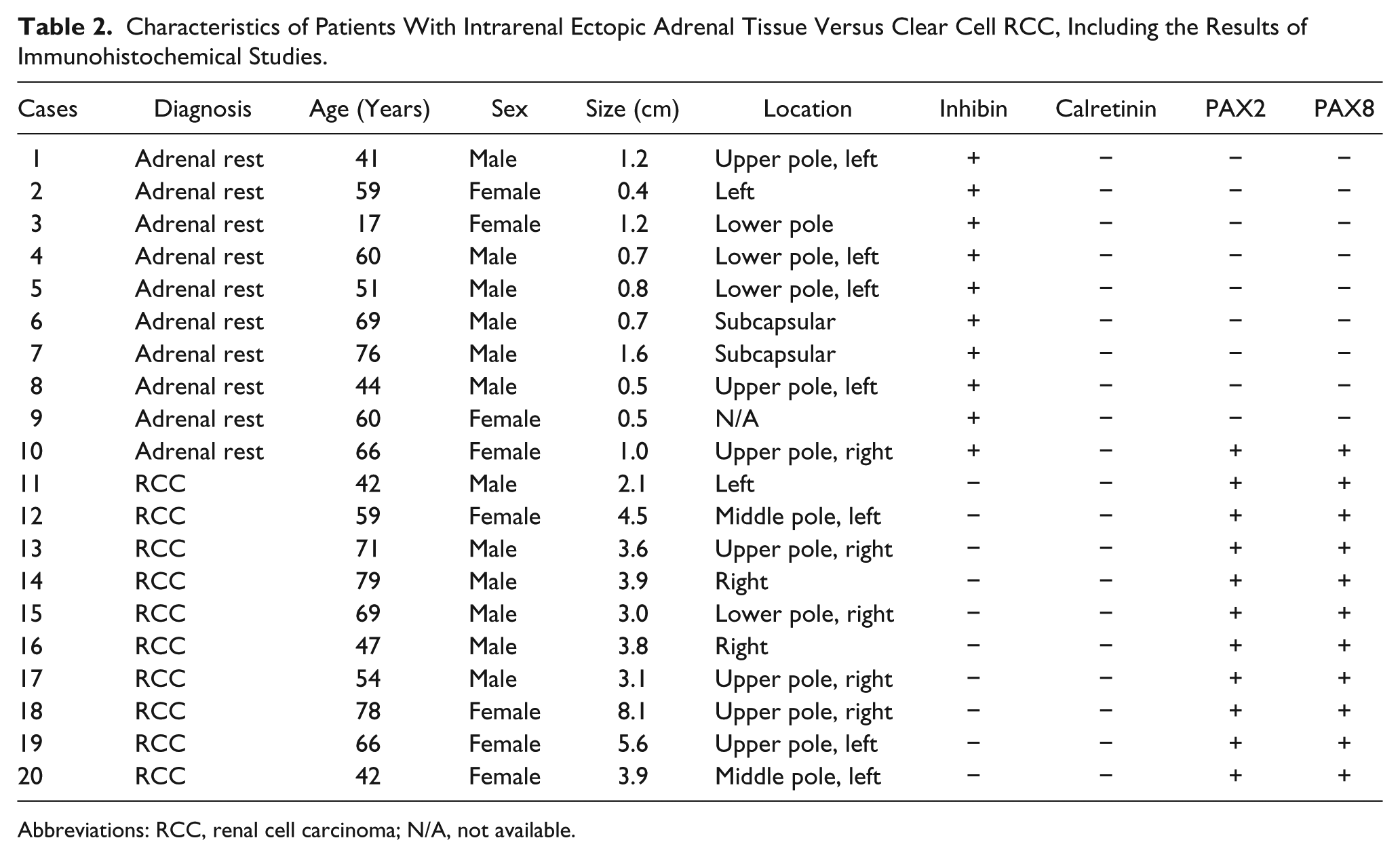
Abbreviations: RCC, renal cell carcinoma; N/A, not available.
All intrarenal ectopic adrenal tissue cases were incidentally identified. Eight out of 10 cases of AR were donor kidney tissue biopsy or wedge resection submitted for frozen section diagnosis during kidney transplantation. Frozen section diagnoses for these 8 cases were as follows: renal cell neoplasm in 1 case, adrenal rest cannot exclude RCC in 1 case, no malignancy identified in 2 cases, and adrenal rest in 4 cases. One AR case was an incidental abdominal mass discovered during workup for abdominal pain. This case was initially diagnosed as a clear cell lesion of uncertain type. An amendment was issued, subsequently, with the diagnosis of benign clear cell lesion most likely adrenal rest. One case was a radical nephrectomy due to poor renal function with multiple stones and cysts.
Six of the RCC cases were radical nephrectomies and 4 were partial nephrectomies. Six cases were diagnosed incidentally by computed tomography scan or ultrasonography, 3 cases presented with flank pain, and 1 case presented with hematuria.
By immunohistochemistry, all AR cases were positive for inhibin and negative for calretinin. In addition, all but 1 case was negative for PAX2 and PAX8. All RCC cases were positive for PAX2 and PAX8, and negative for inhibin and calretinin. PAX8 was weakly positive in 2 cases (Figure 1).
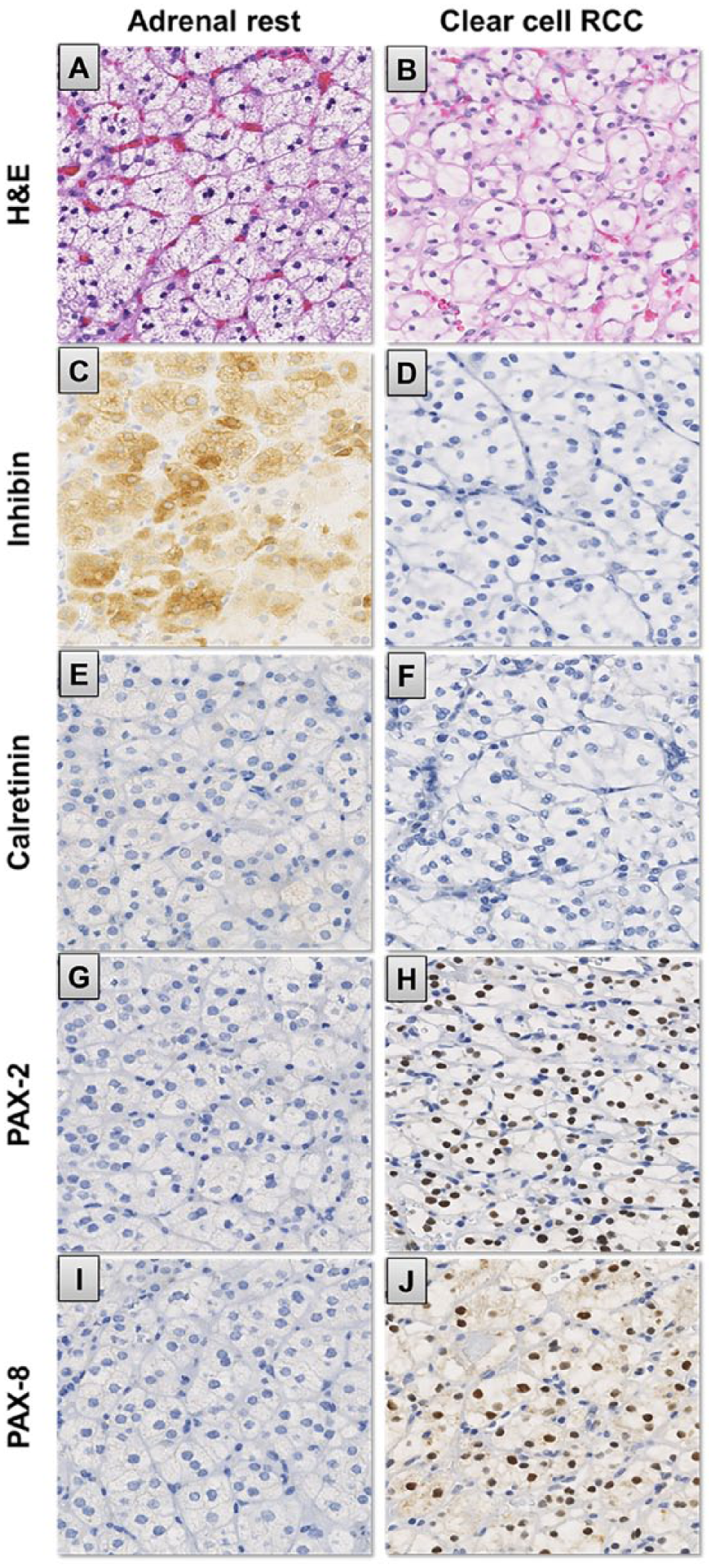
Immunophenotype of intrarenal ectopic adrenal tissue versus clear cell renal cell carcinoma (RCC). Significant morphologic overlap between (A) adrenal cortical lesions and (B) clear cell RCC on hematoxylin-eosin is noted. Adrenal cortical lesions showing positive cytoplasmic staining for inhibin (C) and negative staining for calretinin (E), PAX2 (G), and PAX8 (I). Clear cell RCC showing diffuse nuclear PAX2 (H) and PAX8 (J) staining but negative staining for inhibin (D) and calretinin (F).
Discussion
Ectopic AR tissue has been found in various anatomic sites including celiac plexus, kidney, testis, epididymis, broad ligament, the canal of Nuck, hernia, hydrocele sac, mesoappendix, liver, lung, intradural space, and brain.4,5 Cortical tissue is believed to be the single and only component of ectopic AR as there have not been any reports of accompanying medullary tissue. Occasionally, AR tissue undergoes significant hyperplasia and may develop adrenocortical adenoma and carcinoma. 5 Ectopic AR could be either functional or nonfunctional depending on their hormone secretion status. Unlike their functional counterparts, nonfunctional ectopic AR could go undetected since the patients are often asymptomatic.
Calretinin is a calcium-binding protein, which mediates the signaling pathway of intracellular calcium, an important messenger in cellular proliferation and differentiation. 6 Calretinin is often used in the diagnosis of malignant mesotheliomas.7,8 Its presence in certain steroid-producing neoplasms, such as ovarian stromal tumors, 7 suggests that neoplasms arising from the adrenal cortex, a steroid-rich tissue, could exhibit positive immunoreactivity for this antigen. In fact, several studies have shown its utility in identifying adrenal cortical tissue and neoplasms.
Inhibin is a disulfite-linked glycoprotein dimer, which belongs to the transforming growth factor-β peptide family and is composed of an α- and a β-subunit. 9 The α-subunit is evident in gonadal stromal cells and extragonadal tissues, including the adrenal gland. 10 The antibody against the α-subunit is utilized in the differential diagnosis of ovarian sex cord-stromal neoplasms. 10 The role of inhibin in the diagnosis of adrenal neoplasms is well established. 11
Cell lineage specific or restricted transcription factors are a group of regulatory proteins exhibited in certain primordial tissues in the embryonic stages and in differentiated adult tissues. 12 Neoplastic cells derived from these tissues are capable of maintaining the expression of these proteins, 12 thus these proteins can be utilized in identifying the probable tissue origin for these tumors. PAX2 is a transcription factor and is crucial in the development of nephric lineage cells and tissues.13,14 PAX2 is exhibited in the Wolffian (nephric) duct and renal tubular cells of both fetal and adult kidneys. It is also found in RCC, Wilms tumor, and nephrogenic adenomas.15-19 The detection of PAX2 in nephrogenic adenomas emphasizes the latest finding that nephrogenic adenomas develop from the proliferation of transplanted renal tubular cells in the urinary tract. PAX8 is another nephric-lineage determining transcription factor that is always co-expressed with PAX2 in embryonic and adult renal tissues. 20
When AR tissue is composed of predominantly clear cells, it may mimic RCC as both contain delicate intervening vasculature and it is often hard to see the cytoplasmic vacuoles that indent the nuclei, especially at the time of frozen section. This diagnostic pitfall could lead to improper management of patients and unnecessary surgery. We evaluated cases of ectopic AR tissue in the kidney, in our pathology archives, and investigated their immunohistochemical profile. In our series, AR tissue in kidney was difficult to diagnose in 2 cases at the time of frozen section, one was diagnosed as “favor neoplasm” and the other diagnosed as “cannot exclude renal cell carcinoma.”
In this study, all cases of AR were positive for inhibin and all cases of RCC were positive for PAX2 and PAX8. Grossly, only half of the AR cases were located in the subcapsular region and the upper pole. Most important, the majority of AR cases were discovered incidentally and were very small in size (average <1 cm). Interestingly, calretinin stain was noncontributory in our study, and we are not sure why this is the case. Other studies have shown calretinin to be a useful stain for adrenal cortical tissue. 21 The positive control worked appropriately in our laboratory. Our antibody for calretinin is monoclonal, which can account for reduced sensitivity according to Zhang et al. 21 It is also possible that ectopic adrenal tissue does not express calretinin in a similar manner to the adrenal cortex. Other studies have shown that inhibin and calretinin are less valuable in identifying adrenal tissue and recommended the use of other markers such as ENT1, melan-A, or SRC1. 22
Conclusion
Ectopic adrenal tissue is of no clinical significance, but sometimes it may pose a diagnostic challenge. A limited panel of inhibin (for AR), and PAX2 and PAX8 (for RCC), can be very helpful and informative. Pathologists and clinicians should be aware of small incidental AR tissue discovered in the kidney in the course of other procedures or workup.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.