
Abstract

A 79-year-old woman was found to have a 0.9 cm polypoid lesion in the colorectum during colonoscopy. The lesion was removed by snare polypectomy and sent to our department for pathological evaluation (Figure 1A). Histologically, the colonic mucosa showed elongated, serrated crypts with maintained maturation toward the surface, consistent with a colorectal hyperplastic polyp (Figure 1B). In addition, our attention was drawn to prominent subepithelial lymphoid aggregates, which were composed of monomorphic, small lymphoid cells without visible germinal centers (Figure 1C). No sheets of blasts were detected. Immunohistochemically, the lymphoid aggregates showed a strong and homogenous staining for CD20 (Figure 1D), bcl-2, and cyclin D1 (Figure 1E) and a partial reactivity for CD5 while being negative for CD3, bcl-6, CD10, and CD23. No light chain–restricted neoplastic B-cell population was identified. Ki-67 staining revealed a proliferation activity of approximately 30% in the neoplastic cell population. In summary, the morphological and immunohistochemical findings were consistent with a colonic manifestation of mantle cell lymphoma (MCL), found coincidentally on excision of a hyperplastic polyp. Further workup revealed multiple other manifestations of MCL throughout the gastrointestinal tract, compatible with a typical presentation of MCL as multiple lymphomatous polyposis (MLP).
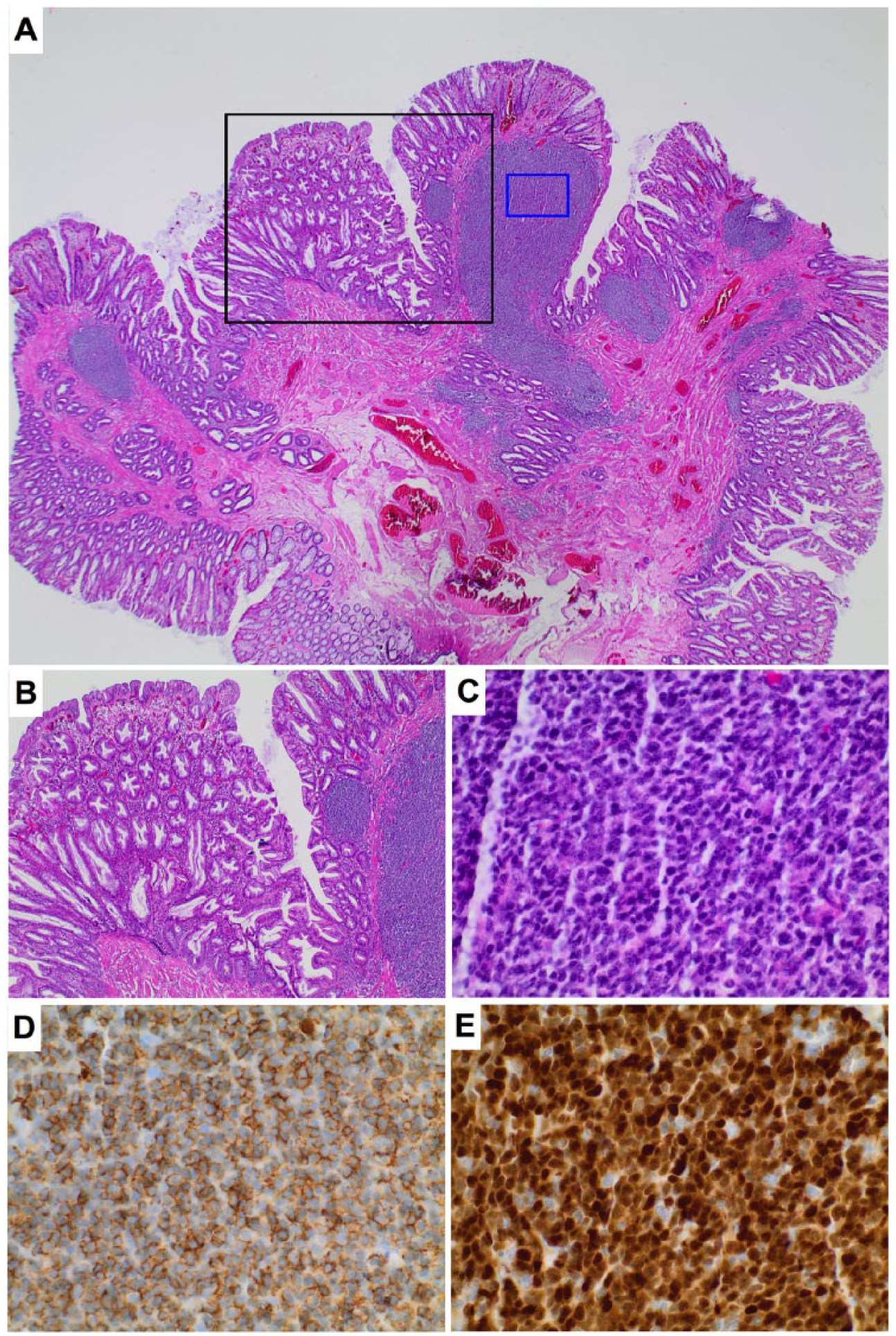
(A) A 0.9 cm polypoid lesion of the colorectum was noted on colonoscopy. (B) The colonic mucosa showed typical features of a hyperplastic polyp including straight, serrated, and funnel-shaped crypts (black rectangle in “A”). (C) Subepithelial lymphoid aggregates composed of monomorphic, small lymphoid cells without visible germinal centers were detected (blue rectangle in “A”). The neoplastic cell population homogenously and strongly expressed CD20 (D) and cyclin D1 (E), consistent with mantle cell lymphoma. Original magnifications: 12.5× (A), 40× (B), and 400× (C, D, and E).
MCL is a B-cell non-Hodgkin lymphoma with a most often aggressive clinical behavior. It is characterized by the t(11;14)(q13;q32) hallmark translocation transposing the cell cycle regulator CCND1 under the control of the immunoglobulin heavy chain locus. Gastrointestinal involvement of MCL at primary diagnosis is reported to be below 30% and usually presents as MLP, which was first described in 1961 by Cornes et al as a diffuse proliferation of atypical lymphocytes at different sites of the gastrointestinal tract.1,2 It has been considered to exclusively represent MCL, though some studies cast doubt on this concept. 3 The clinical presentation of MLP is heterogeneous, but most commonly includes gastrointestinal symptoms like abdominal pain, diarrhea, and hematochezia. 4 MLP is treated as any MCL, regularly compromising either conventional chemoimmunotherapy (eg, R-CHOP), involved-field radiation, or intensive chemoimmunotherapy (eg, R-Hyper-CVAD/cytarabine/MTX), which was recently shown to considerably improve the prognosis of young patients reaching a median overall survival of 13.4 years.5,6 In light of the huge clinical impact, the demonstrated case underscores the necessity to closely examine submucosal lymphoid aggregates in specimen received as simple polyps for signs of atypia in order not overlook a gastrointestinal lymphoma manifestation.