
Abstract
Villous morphology in urinary bladder biopsy is a relatively uncommon finding. Villi are slender, finger-like structures that are commonly seen in the small intestine or in neoplastic lesions of gastrointestinal lineage/differentiation. Importantly, placenta also exhibits villi that are morphologically and functionally different from the intestinal one. Majority of the neoplastic lesions of urinary bladder are urothelial in origin with a minor subset showing glandular differentiation. While the presence of benign villi in urinary bladder biopsy necessitates a search for an occult perforation, provided a sample mismatch is ruled out, cytoarchitecturally abnormal/dysplastic villi indicate a neoplastic lesion of the urinary bladder encompassing villous adenoma and adenocarcinoma and urothelial carcinoma with villoglandular differentiation. The dysplastic villi in urinary bladder also imply a lower gastrointestinal endoscopy to rule out a colorectal primary. The development of the villous lesions in the urinary bladder and the colorectum are embryologically related and pose a major diagnostic challenge to the clinicians and surgical pathologists due to identical histomorphology and immunohistochemistry. We tend to discuss the morphological differentials and diagnostic approach to the villous lesions in the urinary bladder biopsy.
Keywords
Introduction
Villi are finger-like structures that are normally found in the small intestine. These light microscopic structures are about a millimeter long and increase the absorptive surface area of the small intestine. Naturally, they are regularly encountered by the gastrointestinal pathologists. The life of uropathologists, in contrast, revolves around papillae, similar looking structures that project as fingers within the lumen of the urogenital tract. Both villi and papillae are light microscopic finger-like projections with central fibrovascular cores. Nevertheless, the villi are the normal structures in the small intestine and serve absorptive function. Instead, the papillae arise out of pathology in the urinary bladder, reactive or neoplastic in nature, and do not serve any normal function. Consequently, majority of the urinary bladder biopsies reveal papillary structures due to reactive papillary hyperplasia of the bladder mucosa or papillary urothelial neoplasms. Only occasionally, villi are encountered in the urinary bladder biopsies and their presence is usually indicative of a neoplastic pathology. This review article highlights the importance of villous morphology in the urinary bladder biopsies, their pathogenesis, and differential diagnosis.
How to Differentiate Papillae and Villi?
The villi provide absorptive surface and hence requires a thin epithelial layer for easy diffusion of the nutrients through it. In contrast, the papillae are reactive or neoplastic in nature. Consequently, the villi have a thin (usually single) layer of epithelium around the fibrovascular core whereas the papillae have multiple epithelial layers around the core as a result of epithelial hyperplasia or neoplasia (Figure 1a and b). It is important to note that the presence of both papillae and villi in the urinary bladder biopsy is pathological.
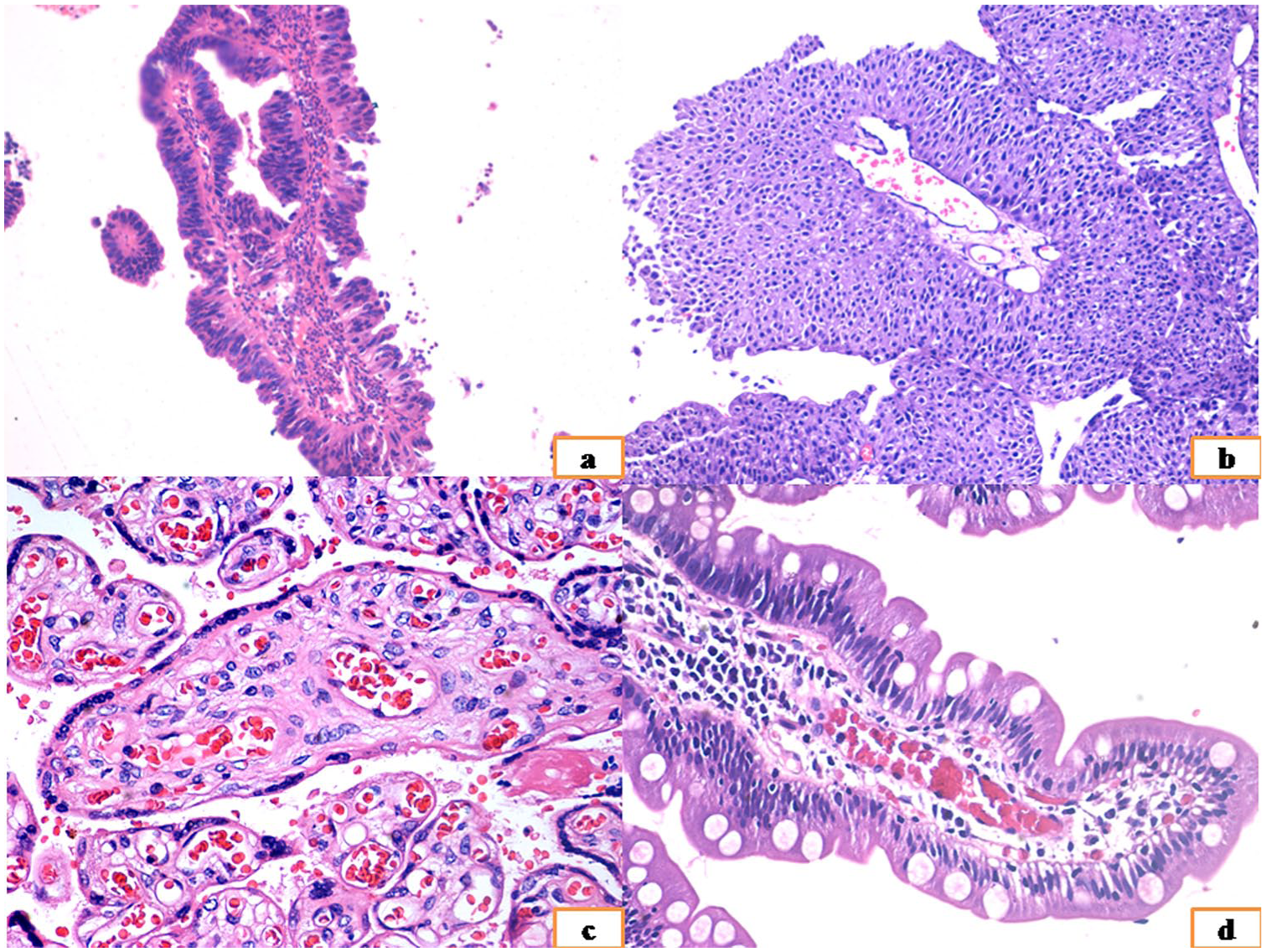
The difference between a dysplastic intestinal villus (from a case of villous adenoma; a) and papilla (from a case of low-grade non-invasive papillary urothelial carcinoma; b). The difference between placental villi (c) and a normal intestinal villus (d). Also note the features of dysplasia in (a) as compared with (d).
Pathogenesis of Villous Neoplasms in Urinary Bladder
There are many pathogenetic theories of villous adenoma (VA) of which the embryogenic theory is the most popular. The urinary bladder is derived from the cloaca that gets separated into a urogenital sinus and anal canal by the urorectal septum by seventh week of the life. Hence, the urinary bladder is an endodermal derivative. Similarly, the anal canal, also an endodermal derivative differentiates into the terminal part of the gastrointestinal tract. VA is proposed to arise from the embryological remnant of the cloaca in the urinary bladder. 1
The development of glandular neoplasm in urinary bladder may also follow a chronic irritation–metaplasia–dysplasia–neoplasia sequence.2,3 The common occurrence of VA with cystitis cystica glandularis, similar type of mucins and similar genetic aberrations in these lesions support this theory.1,2 However, long-term follow-up of cystitis cystica glandularis and intestinal metaplasia usually does not augur into malignancy of urinary bladder, an observation that challenges the latter theory. 4
Differential Histomorphology and Immunohistochemistry of Villous Morphology in Urinary Bladder Biopsy
Usually, villous morphology in the urinary bladder is associated with a benign or malignant neoplastic process, once a sample mismatch is ruled out. A perforation following transurethral resection of bladder tumor (TURBT) is an uncommon complication. A surgical neo-bladder is constructed by parts of small and/or large intestine following radical cystectomy. Obviously, the biopsy from a neo-bladder would show gastrointestinal morphology and villi, provided small intestine is used for its construction. Importantly, although villi are usually equated with gastrointestinal tract or intestinal differentiation of a tumor, they can also be seen in relation to placenta. The morphology of placental villi is different from the intestinal type of villi.
Please Rule Out a Sample Mismatch!
A surgical pathologist first must rule out a possibility of a sample mismatch before considering any of the mentioned organic lesions. This is by far the commonest cause of finding a villous architecture in the urinary bladder biopsy in my experience.
Perforation: A Wolf in Sheep’s Clothing
Perforation can be iatrogenic or organic. Approximately, 0.5% TURBT cases are complicated by post-procedural perforation. 5 The surgical pathologist may find separately lying benign intestinal tissue along with the lesion of the urinary bladder. The intestinal epithelium does not show any evidence of dysplasia and may be associated with fragments of intestinal submucosa, muscularis, and serosa. The presence of serosa containing lobules of adipocytes or the mesothelial lining of the peritoneum may alert the pathologist. In addition, the biopsy may exhibit areas of hemorrhage and necrosis. A high index of suspicion and conversation with the urologist is often warranted due to the possibility of an occult perforation. Suggestive corroborative clinical history includes severe pain complained by the patient following the procedure.
Intestinal mucosa can also be sampled in cases of enterovesical fistula caused by trauma, surgical intervention, Cröhn’s disease, or intestinal malignancy. Approximately, 2% to 6% patients with Cröhn’s disease develop enterovesical fistula.6,7 These cases are usually diagnosed on the basis of suggestive clinical history and presentation.
A malignant fistula is usually formed when a colorectal or uterine malignancy directly invades the urinary bladder. A tumor deposit in the rectovesical or rectouterine pouch can also enlarge in size and infiltrate the bladder mucosa. One of the authors (SM) has the experience of seeing an unusual case where the TURBT chips showed a villiform lesion with high-grade dysplasia. The colonic biopsy of the same patient revealed an adenocarcinoma arising from dysplastic colonic lining. The radiology of the case showed a single communicating mass. An extensive panel of immunohistochemistry failed to reveal the origin of the tumor. Nevertheless, the tumor showed microsatellite instability and was considered to arise from colon as colonic adenocarcinoma is more commonly associated with microsatellite instability and can arise from non-polypoidal dysplastic mucosa. The synchronous dysplasia in the lining of both colon and the urinary bladder can occur as the colonic adenocarcinoma can colonize the surface mucosa of the urinary bladder. 8
Perforation of the urinary bladder can also occur due to direct invasion by placenta. This is caused by abnormally invasive placenta (AIP), which does not show an intervening layer of decidua and invades the uterine wall to a variable extent. The AIP is classified as placenta accreta, placenta increta, and placenta percreta according to the depth of invasion. Placenta percreta comprises of only 5% of the AIP. 9 The invasion of the urinary bladder by placenta percreta is a nearly fatal condition due to massive hemorrhage. Hematuria occurs in only one fourth of these cases. 9 A clinical diagnosis and management is the norm and this is unlikely to be biopsied. Prenatal diagnosis of AIP is also possible via cystoscopy. 10 The lesion typically occurs at the posterior wall of the urinary bladder. Biopsy may reveal chorionic villi that are morphologically different from the intestinal type villi. The chorionic villi are lined by a layer of syncytiotrophoblastic giant cells and mononuclear cytotrophoblasts. These cells are cuboidal and lack the columnar shape of the intestinal villi, basally located oblong nuclei and cytoplasmic mucin (Figure 1c and d). Immunohistochemistry for βHCG (human chorionic gonadotrophin) is positive in the syncytiotrophoblasts in doubtful cases.
Villous Adenoma (VA)
The VA of the urinary bladder mimics its intestinal counterpart. It is typically a solitary lesion with an affinity for the dome, urachus, and trigone. Hematuria, dysuria, and mucusuria are the usual manifestations. The mean age of the patients is above 69 years in a large series by Seibel et al, 11 whereas a smaller series showed much lower mean age (40 years) in Indian population. 12 The mean age was 62 years in the largest series of VA comprising of 23 cases. 13 The architecture shows villous or tubulovillous morphology with low- to high-grade dysplasia of the lining epithelium (Figure 2a and b).13,14 The features of dysplasia include nucleomegaly, nuclear crowding, nuclear stratification, hyperchromasia, anisonucleosis, and anisochromia. Luminal mitosis is seen in high-grade areas. The nuclei are basally oriented, elongated with vesicular chromatin, and conspicuous to prominent nucleoli. The loss of basal orientation and polarity is usually a feature of high-grade dysplasia or in situ adenocarcinoma. The cytoplasm contains microvesicular mucin, goblet-cell mucin, or is devoid of it. No umbrella cell or urothelial cell is noted within the lesion though it can be collared by a cuff of normal urothelium. The bladder mucosa in the immediate vicinity of the VA may exhibit chronic inflammatory changes, cystitis cystica glandularis, and intestinal metaplasia. 15 Squamous metaplasia and calcification of the VA can be seen.11,12
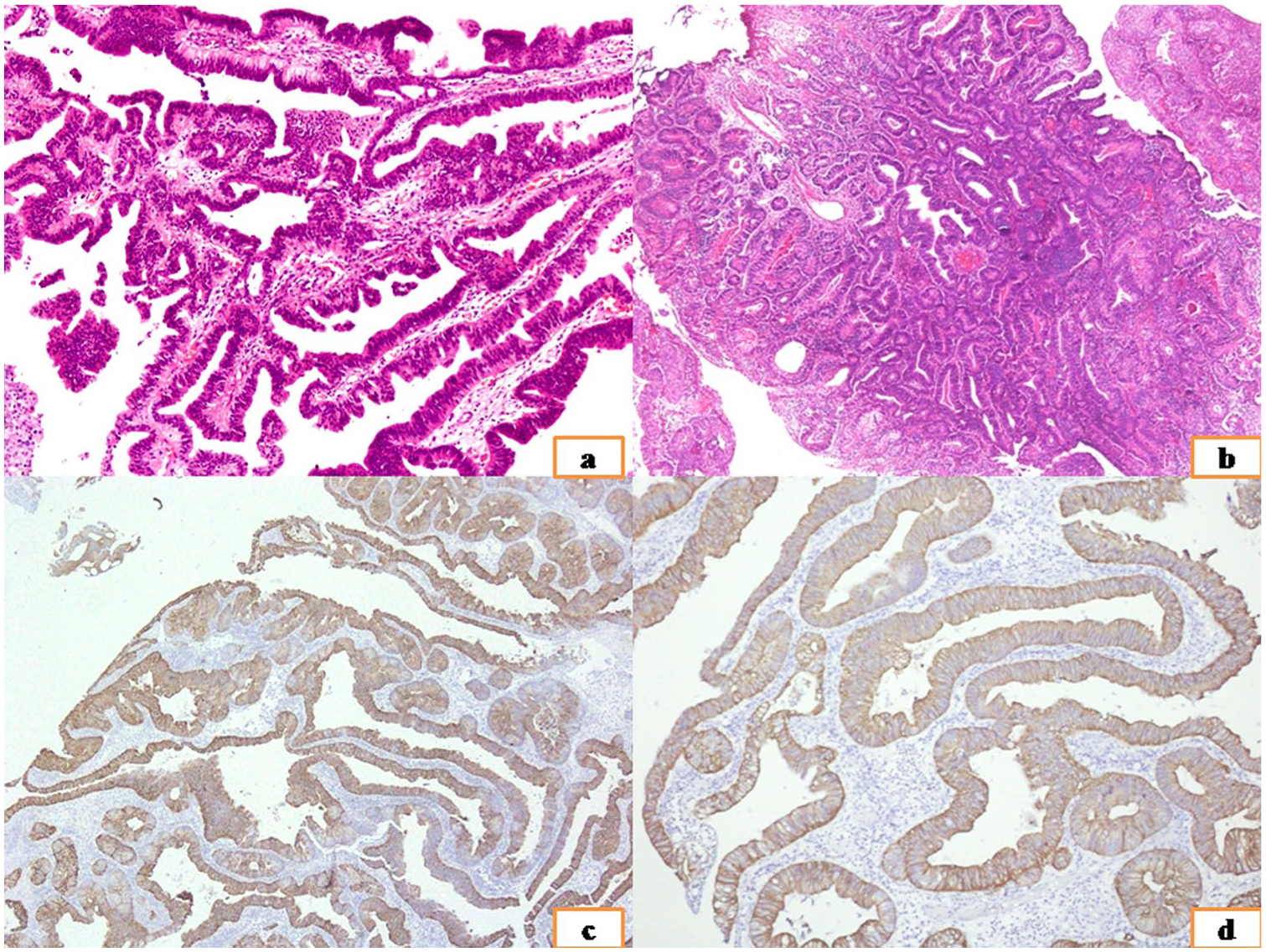
Two cases of villous adenoma showing villous (a) and tubulovillous (b) architecture. Diffuse strong membranous positivity for CK20 (c) and β-catenin (d).
Immunohistochemistry of VA shows CK20 (membranous; Figure 2c) and CDX2 (nuclear) positivity in 100% cases. The positivity of CK20 is intense, complete membranous, and involves majority of the tumor cells in contrast to CK7 positivity, which is positive in 33% to 50% cases, incomplete membranous and less intense. Majority of the cases show luminal positivity for carcinoembryonic antigen. EMA is positive in a minor subset of cases. 1 β-catenin shows membranous positivity (Figure 2d) highlighting no role of β-catenin pathway in the tumorigenesis. GATA3 is negative to focally cytoplasmic positive. Nuclear positivity is not seen. Similarly p63 nuclear positivity is absent in the tumor cells although the myoepithelial cells can be highlighted by p63 immunostain. Nuclear GATA3 and p63 negativity distinguish this lesion from being a part of urothelial carcinoma with villoglandular differentiation. 12
A pure VA usually does not pose a diagnostic challenge to a pathologist. However, it may be associated with and is a precursor lesion of adenocarcinoma. VA is reported to be associated with in situ and invasive adenocarcinoma, and noninvasive and invasive papillary urothelial carcinoma.11,16 A complex lesion can show the presence of all these in situ and invasive neoplastic lesions making the diagnosis challenging. At times, extensive cystitis cystica glandularis with intestinal metaplasia mimic a tubulovillous adenoma. However, cystitis cystica glandularis does not show the dysplastic changes associated with VA. 1 Nephrogenic adenoma is a great mimicker of glandular malignancies of the lower urinary tract due to its wide distribution, often incidental detection and protean morphology. The papillary/polypoid and tubulocystic or a combinatorial morphology may mimic VA. The papillary lining is usually double cell-layer thick similar to a villus although the lining cells have a flat cuboidal to low columnar morphology. Nucleolar prominence is a feature and the lesion exhibits PAX2/PAX8 positivity rendering its distinction from VA. CDX2 is negative in nephrogenic adenoma.17-19
Villous Adenoma With In Situ and Invasive Adenocarcinoma
In their seminal series, Cheng et al 13 and Seibel et al 11 have described 23 and 18 cases of VA, respectively. The series by Seibel et al 11 included a case arising from the prostatic urethra while 2 of their cases involved the urinary bladder and the prostatic urethra. 11 Eight out of these 23 cases and 11 out of these 18 cases showed an in situ or invasive adenocarcinoma.11,13 The diagnosis of an in situ or an invasive carcinoma is similar to that of its intestinal counterpart. VA shows variable degree of epithelial dysplasia. An in situ carcinoma shows full-thickness dysplasia. The cytological atypia is usually associated with architectural atypia in the form of complex architecture, cribriforming, and lack of orderly maturation. However, an architectural atypia is usually not a mandate for in situ carcinoma.
An in situ carcinoma needs to be distinguished from an invasive one by assessing the breach of basement membrane and lamina propria invasion. This becomes particularly difficult as VA can show tubular architecture with endophytic growth pattern. Broad invaginations into the underlying tissue can also be seen in VA, which appears invasive. Moreover, the VA arising from the urachus can exhibit intramuscular presence of the glandular epithelium. 11 The presence of smaller invasive nests and irregular glands, and desmoplastic stroma are the most important clue to the diagnosis of an invasive component. Low-grade dysplasia of the true invasive component is unlikely and such area tends to represent an endophytic component of a VA. Displacement/prolapse of the VA is possible due to the ischemia/infarction of the stalk. A broad based invagination as deep as the submucosa can be seen in such case. However, the presence of low-grade dysplasia, scattered siderophages (due to prior ischemic injury), and a thin rim of lamina around the dysplastic epithelium help distinguish it from a true invasion.
Metastatic Adenocarcinoma
An adenocarcinoma of the urinary bladder comprises only 0.5% to 2% of all urinary bladder malignancies. 8 The occurrence of secondary bladder adenocarcinoma (SBA), metastatic or directly invasive, is more common.8,20,21 Importantly, the morphological distinction between a primary bladder adenocarcinoma (PBA) and an SBA of colorectal primary are not possible as both originate from similar groups of cells.22,23 Moreover, a PBA and an SBA of colorectal primary can occur synchronously or the colorectal carcinoma can colonize the epithelium of the urinary bladder.24,25
One of the necessary clues to the diagnosis of a PBA and an SBA of colonic primary is radiology although it is not highly sensitive or specific. Nevertheless, the major brunt of the disease can often be determined by radiology and forms the basis of the origin of the tumor. Many articles have focused on the immunohistochemical stains to distinguish PBA and SBA of colonic primary due to their morphologic similarities. Majority of the immunomarkers including cadherin-17, GATA3, p63, CK7, CK20, villin, and CDX2 are ineffective to differentiate between these 2 entities.8,20,26 Abnormal nuclear/nucleocytoplasmic expression of β-catenin shows some promise in this regard, which is more commonly expressed in the SBA of colonic primary. Similarly, abnormal nuclear E-cadherin expression is more commonly see in PBA.8,20 While these markers may aid in the diagnosis of colonic or bladder primary, they lack in their specificity. Nuclear β-catenin is expressed in about 75% to 80% colonic adenocarcinoma due to APC/β-catenin pathway activation. However, rest of the cases of colonic adenocarcinoma show microsatellite instability and are unlikely to show nuclear expression of β-catenin. In the example cited above, the colonic adenocarcinoma developed via microsatellite instability pathway and did not express nuclear β-catenin.
The metastatic adenocarcinoma can have non-colonic primaries, the diagnosis of which is dependent on adequate clinical history, sometimes histomorphological clues and immunohistochemistry.
Villous Adenoma/Adenocarcinoma Associated With Noninvasive/Invasive Papillary Urothelial Carcinoma and Urothelial Carcinoma With Villoglandular Differentiation
The complexity of VA has been depicted by Seibel et al 11 who described coexisting papillary urothelial lesions in 18% cases (n = 3/18). This series depicted one case each of VA with noninvasive papillary urothelial carcinoma, VA with in situ change and invasive papillary urothelial carcinoma, and VA with adenocarcinoma arising from it associated with invasive papillary urothelial carcinoma. The classification scheme by Seibel et al 11 did not highlight any low-grade or high-grade morphology of the urothelial lesion. Later, Lim et al 27 has introduced the terminology of urothelial carcinoma with villoglandular differentiation (UCVGD) in 2009. The case series of Lim et al 27 was composed of 14 unique cases occurring predominantly in elderly males where the malignancy showed both urothelial and villoglandular differentiation. This case series showed noninvasive papillary urothelial carcinoma in the urothelial counterpart of UCVGD in about one fifth of the cases whereas rest of the cases showed a high-grade invasive papillary urothelial component. In fact, a significant proportion of these cases even show detrusor invasion, extravesicular extension, angiolymphatic invasion, and association with adenocarcinoma or other aggressive morphological subtypes of urothelial carcinoma like plasmacytoid, small cell, and sarcomatoid variant portending a poor prognosis. Similar observation has later been reported by Mitra et al and Tajima et al12,28-30 We believe that the 3 cases initially described by Seibel et al 11 may actually represent UCVGD forming the first description of this uncommon entity under a different rubric.
UCVGD is characterized by the presence of both urothelial and villoglandular architecture of the tumor that usually blends with each other (Figure 3a). The urothelial component may exhibit divergent differentiation and hence variable morphology. The cytoarchitectural features of the papillary urothelial and the villoglandular areas are quite different and easily appreciable. While the papillae are short, stubby, and show multiple epithelial layers, the villoglandular areas show filiform, long, slender projections with one third cell layer thickness of the epithelium. 12 The villoglandular areas with high-grade nuclear morphology show cribriform pattern and cuboidal cells (Figure 3b) in contrast to the fused papillae in the urothelial areas. The cells in the villoglandular areas are usually columnar apart from the cribriform areas with basally oriented elongated nuclei and intracytoplasmic mucin vacuoles. In contrast, the urothelial cells are polygonal with centrally located round to oval to grooved nuclei, and abundant eosinophilic to clear cytoplasm. The villoglandular areas can show low- and high-grade nuclear morphology. 12
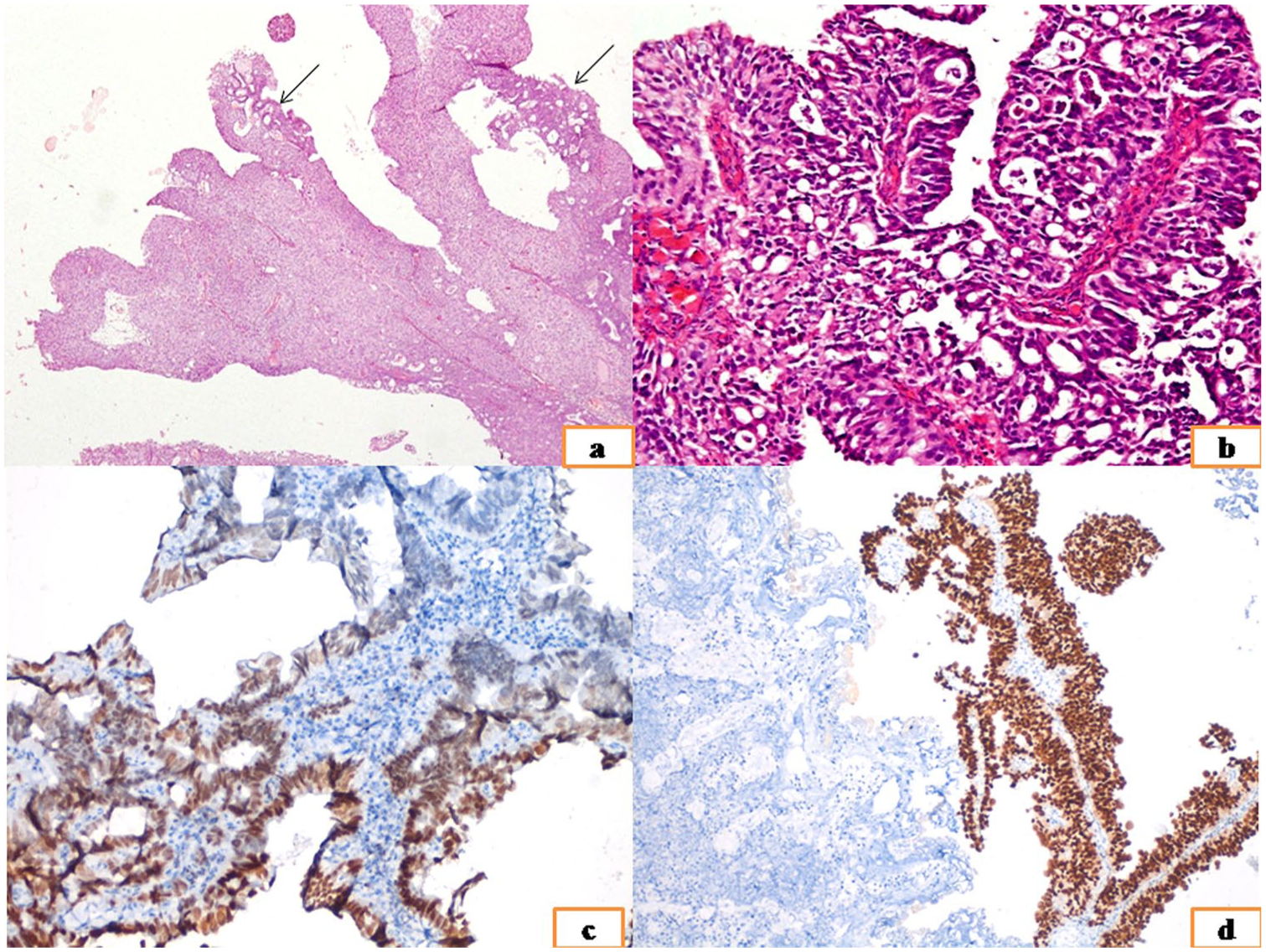
(a) A case of UCVGD showing dominantly papillary urothelial component with tiny foci of villoglandular areas (black arrows) having a cribriform architecture. (b) High-grade villoglandular areas of UCVGD usually exhibit cribriform architecture and cuboidal tumor cells. (c) Focal variable intensity nuclear GATA3 expression in the villoglandular component of a UCVGD. (d) The urothelial areas of the same tumor showed strong diffuse nuclear GATA3 expression.
The major morphologic differentials of UCVGD are VA with or without in situ and/or infiltrative changes, high-grade invasive urothelial carcinoma with glandular differentiation, in situ adenocarcinoma, and SBA of colonic primary.12,27 A VA can be an incidental finding that may coexist with any other malignancy of urothelial origin. Hence, it is of paramount importance to distinguish a VA from a UCVGD especially in small biopsies as a variable admixture of urothelial and villoglandular components can be sampled in the biopsy specimen. Moreover, UCVGD is usually associated with poor prognosis whereas complete surgical resection usually suffices for a pure VA. The prognosis of VA may depend on the associated noninvasive or invasive lesion rather than the lesion itself. The presence of both urothelial and villoglandular components in a biopsy is the main clue to the diagnosis of UCVGD. The diagnosis is usually straightforward in the cases where the urothelial component imperceptibly blends with the villoglandular component. The problem arises if the biopsy shows separately lying villoglandular and urothelial components. The presence of cribriform spaces within the villoglandular areas usually represents part of UCVGD rather than VA. 27 Moreover, the villoglandular areas of UCVGD express strong nuclear CDX2 and faint to moderate nuclear GATA3 in about 10% population with high-grade nuclear morphology.12,28 The nuclear expression of GATA3 in villoglandular component, though faint and in a smaller subset of cells (Figure 3c), is typical of UCVGD as none of the other urinary bladder lesions with villoglandular morphology exhibit this peculiarity. In fact, the GATA3 expression by the villoglandular cells justifies the nomenclature of UCVGD rather than a VA coexisting with a urothelial lesion as GATA3 is strongly expressed (nuclei) in urothelial malignancies including the urothelial component of UCVGD (Figure 3d) and is a reliable albeit nonspecific marker of urothelial differentiation. Typically, the glandular areas and bladder adenocarcinoma exhibit absence of nuclear GATA3 expression. In contrast to a VA, UCVGD exhibits only focal nuclear positivity for CDX2 in its villoglandular component. UCVGD typically shows surface villiform architecture unlike high-grade urothelial carcinoma with glandular differentiation that dominantly depicts an otherwise high-grade urothelial carcinoma. In situ adenocarcinoma can have flat, papillary or cribriform areas and typically lack the long, slender villiform projections even in the papillary subtype. The cribriform subtype of in situ adenocarcinoma exhibits columnar cells in contrast to the cribriform areas of UCVGD where the cells adopt cuboidal nature. 12 The distinction from SBA with colonic primary depends on the identification of areas where the urothelial areas blend with the villoglandular architecture. However, β-catenin is of some help in difficult cases. Notably, β-catenin has to be performed in all such cases to rule out a primary colonic etiology. 12
Role of Urine Cytology
The identification of glandular morphology in urine sample is difficult and only a few anecdotal case reports are present exemplifying and documenting this issue.31-33 Urine cytology of VA shows clusters of mucin-filled columnar cells. 33 The identification of both transitional epithelium with atypia and glandular epithelium should arouse suspicion of a UCVGD in urine cytology. However, the glandular lesions of urinary bladder are relatively uncommon and a suspicion/diagnosis in urine cytology is challenging.
An Algorithmic Approach
An algorithmic approach to the diagnosis of the villous lesions is depicted in Figure 4. The first step in the diagnosis of villous lesions of the urinary bladder is the histological distinction between villi and papillae. The histopathologist should be certain about this distinction. Once villi are noted in the biopsy, the surgical pathologist should first rule out a sample mismatch, possibly the commonest cause of the presence of villi in a surgical biopsy from urinary bladder. The next step is to distinguish the intestinal and placental type of villi, the latter possibly representing an abnormally invasive placenta especially if associated with the suggestive clinical history and tissue reaction. The presence of normal intestinal villi may represent an iatrogenic perforation that needs to be interpreted cautiously, preferably following a conversation with the urologist. The presence of villi with cytoarchitectural dysplasia in a urinary bladder biopsy after ruling out a mismatch usually suggests any of the above-mentioned villiform lesions. Obviously, a possibility of mismatch is not considered if the lesion is seen arising directly from the urothelial tissue.
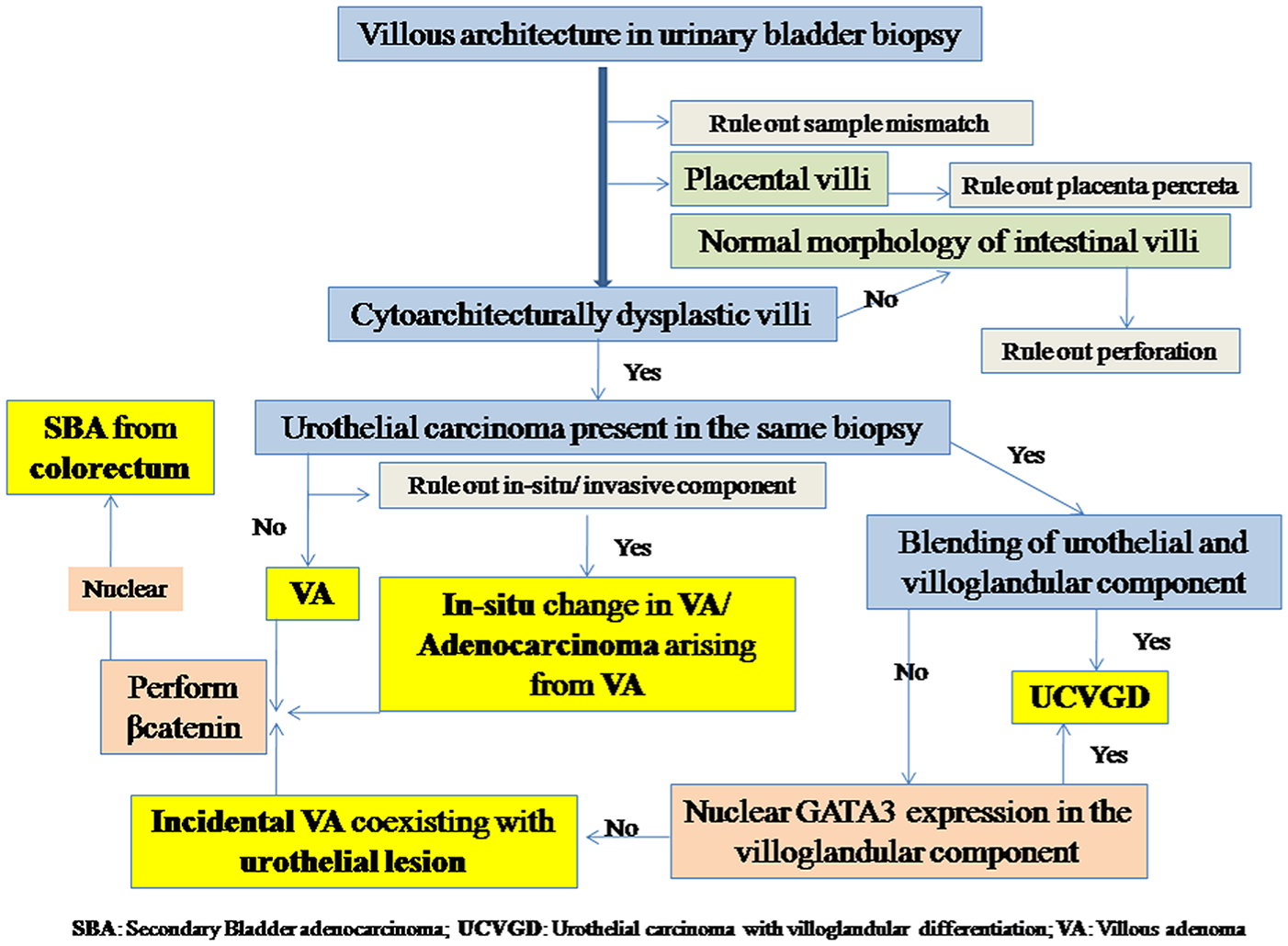
Algorithm for the diagnosis of villous lesions of urinary bladder.
The biopsy should first be screened for the presence of any neoplastic urothelial lesion in the absence of which the diagnosis is usually VA. The lining of the VA should be thoroughly screened for the presence of any in situ lesion or any focus of stromal invasion to rule out an invasive adenocarcinoma arising from a VA. If a villoglandular lesion coexists with a neoplastic urothelial lesion, a diagnosis of UCVGD is suspected. UCVGD exhibits blending of the villoglandular and urothelial components and such blending help the pathologist to make a confident diagnosis of UCVGD. However, the villoglandular component may be seen separately from the urothelial component. The nuclear expression of GATA3 in the villoglandular component, even focally, indicates a diagnosis of UCVGD in these cases. The absence of nuclear GATA3 expression in this scenario usually indicates the coexistence of an urothelial malignancy with an incidentally detected VA. The presence of any neoplastic villoglandular lesion in urinary bladder other than a definite UCVGD necessitates β-catenin immunohistochemistry to rule out an SBA with colorectal primary.
Conclusion
The presence of villi in urinary bladder biopsies is an uncommon finding. However, this finding has immense significance as it may either indicate a few complications of disease or a rare group of neoplasia, the diagnosis, implication, management, and prognosis of which are variable. The pathologists should be aware of these lesions as they often form diagnostic conundrum despite detailed clinical, histomorphological, and immunohistochemical examinations.
Footnotes
Author Contributions
SM conceptualized the manuscript and prepared it. PA and GK were involved in the literature search, data collection, and review of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.