
Abstract

We illustrate a case of SMARCA4-deficient thoracic sarcoma (SDTS), which occurred in the mediastinum of a male in his fifth decade (Figure 1). SDTS is a recently described entity with particular clinicopathologic and molecular features. These typically present as compressive mediastino-pulmonary masses in young to predominantly middle-aged males with a previous history of smoking. 1 They are highly aggressive and, in the absence of effective therapies, lead rapidly to death (median overall survival 5-7 months).2,3 Thoracic imaging shows compressive and infiltrative chest masses with ill-defined necrotic lymphadenopathy. 4
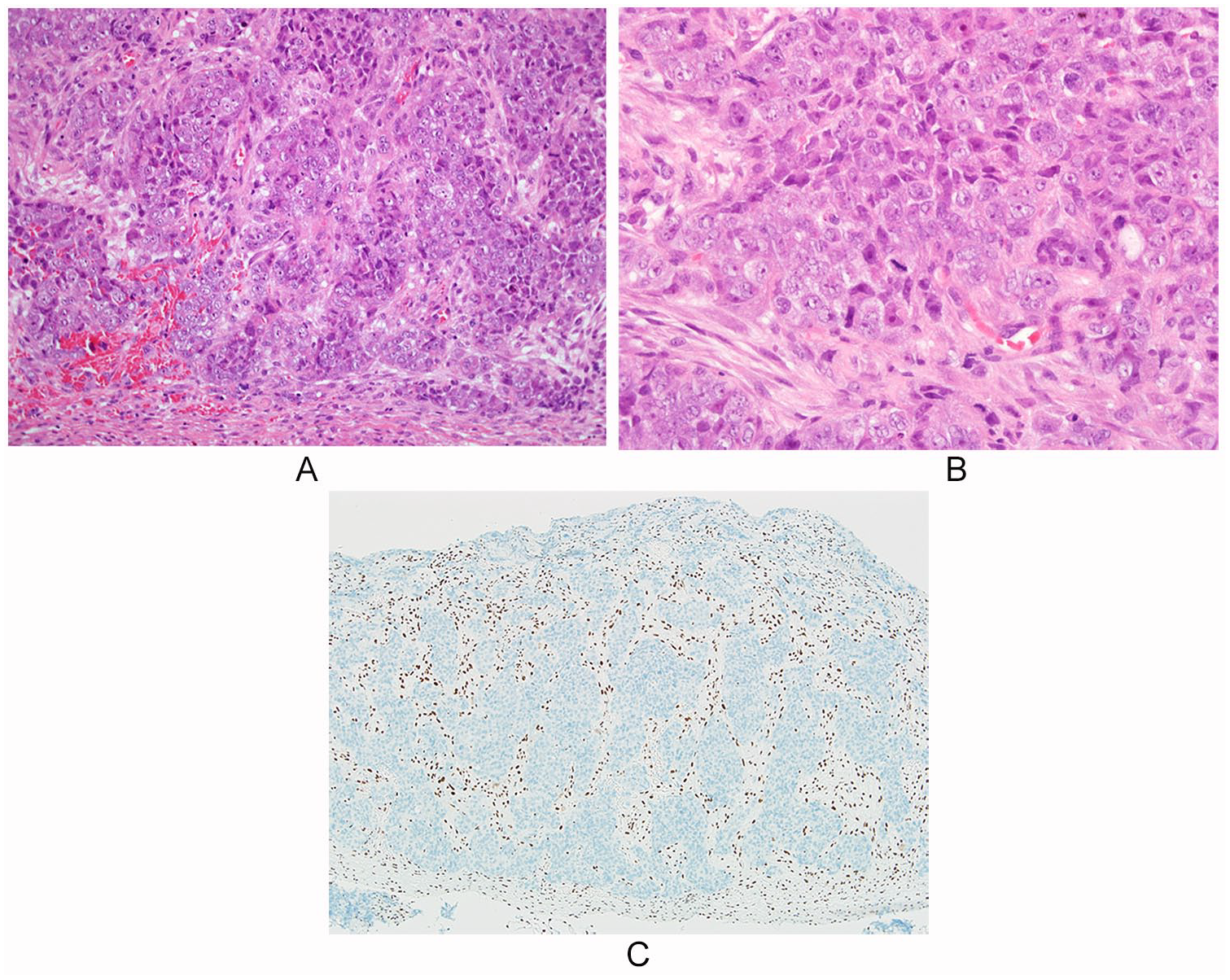
SMARCA4-deficient thoracic sarcoma. This tumor comprises nests and sheets of large, atypical, polygonal, and ovoid cells, with large, prominent nucleoli, and moderate amounts of amphophilic cytoplasm (A, B); tumors are frequently associated with necrosis, and mitotic activity is typically evident (B). Immunohistochemistry for SMARCA4 (BRG1) shows diffuse loss of expression in tumor nuclei. This is in contrast to diffusely retained nuclear expression in the surrounding population of stromal fibroblasts, lymphocytes, and endothelial cells.
Histologically, these are cellular neoplasms comprising infiltrating sheets or trabeculae of poorly differentiated- or undifferentiated-appearing, medium-sized to relatively large epithelioid cells with ovoid vesicular nuclei, moderate amounts of darkly eosinophilic cytoplasm (Figure 1), and sometimes rhabdoid differentiation, with areas of geographic necrosis. Less frequently, there is surrounding desmoplastic stroma reminiscent of desmoplastic small round cell tumor, and rare cases with myxoid/edematous stromal changes. 5 Immunophenotypically, tumors usually show at least focal, strong expression of epithelial markers (AE1/AE3 or epithelial membrane antigen) and CD34 and/or focal strong SALL4, 3 and frequent diffuse expression of SOX2. Only very rare cases express TTF-1 or p63, and only focally, while p40 and NUT are negative. 5 There is typically dual nuclear loss of SMARCA4 (BRG1) and SMARCA2, 5 while SMARCB1 expression is retained in all cases. 5 Molecularly, these neoplasms show alterations in the switch/sucrose non-fermenting complex, also known in humans as BRG1-associated factors. This key complex is responsible for chromatin remodeling through changes in the nucleosome conformation, hence, regulating DNA transcription, replication, and repair. Comparative transcriptomic profiling analyses have suggested distinctness from lung carcinomas, and instead relationship to malignant rhabdoid tumors and small cell carcinoma of the ovary, hypercalcemic type. 3 However, their precise nature still remains to be fully elucidated, and there remains ongoing debate as to whether these truly represent “sarcomas.” Using various molecular platforms, other authors have suggested that these neoplasms may instead primarily represent smoking-associated undifferentiated or dedifferentiated carcinomas rather than primary thoracic sarcomas, with a relationship with non–small cell lung carcinoma (NSCC) supported, variably, (1) by the presence of areas of NSCC components juxtaposed with sarcoma-like areas; (2) focal expression of TTF-1 and p40 (ie, NSCC lineage markers); (3) smoking history in most patients, with genomic smoking signature; and (4) high tumor mutation burden and NSCC-characteristic mutations in a proportion of patients. 1 As our diagnostic awareness of SDTS increases, it appears that these neoplasms may not be as rare as might have previously been envisaged, and many of these have likely previously been diagnosed as poorly differentiated or undifferentiated lung carcinomas. Together with appropriate clinicopathologic correlation, correct identification of this group of neoplasms can provide important prognostic information and likely potential future therapeutic implications.