
Abstract
During breast cancer staging, histological evaluation of axillary sentinel lymph nodes (SLN) is usually straightforward. However, the exact characterization of a small epithelial deposit in an SLN can be challenging, especially during the frozen section examination. We report the first case of endosalpingiosis involving bilateral axillary lymph nodes. We review published literature on axillary endosalpingiosis and discuss the differential diagnosis of small epithelial deposits in an axillary SLN. Pathologists should consider benign epithelial rests and displaced epithelium as differential diagnoses for the microscopic epithelial nodal deposit, especially during the frozen section examination.
Introduction
The histological evaluation of axillary sentinel lymph nodes (SLN) is a crucial component of the surgical management of invasive breast carcinoma. The goal is to identify metastatic epithelial deposits involving the SLN. The presence of benign epithelial nodal deposits can make this process challenging. Rarely, especially during an intraoperative evaluation, the benign epithelial deposits can be misinterpreted as metastasis. The differential diagnoses of microscopic epithelial deposit(s) in axillary SLN include microscopic metastasis (isolated tumor cells and micrometastasis), displaced epithelium, and benign epithelial inclusions. 1 The epithelial inclusions are classified as mammary, Mullerian, and squamous inclusions. 1
We report an unusual case of endosalpingiosis involving bilateral axillary SLN. The epithelial deposits were identified during SLN sampling for metachronous bilateral breast carcinoma. During the frozen section examination, the benign Mullerian-type glands were suspected to be metastasis; however, exact categorization was deferred to permanent sections. We review previously published cases of axillary endosalpingiosis (Table 1).2-17 We also discuss the differential diagnosis of microscopic epithelial deposits in the axillary SLN.
Previous Reports of Axillary Endosalpingiosis.
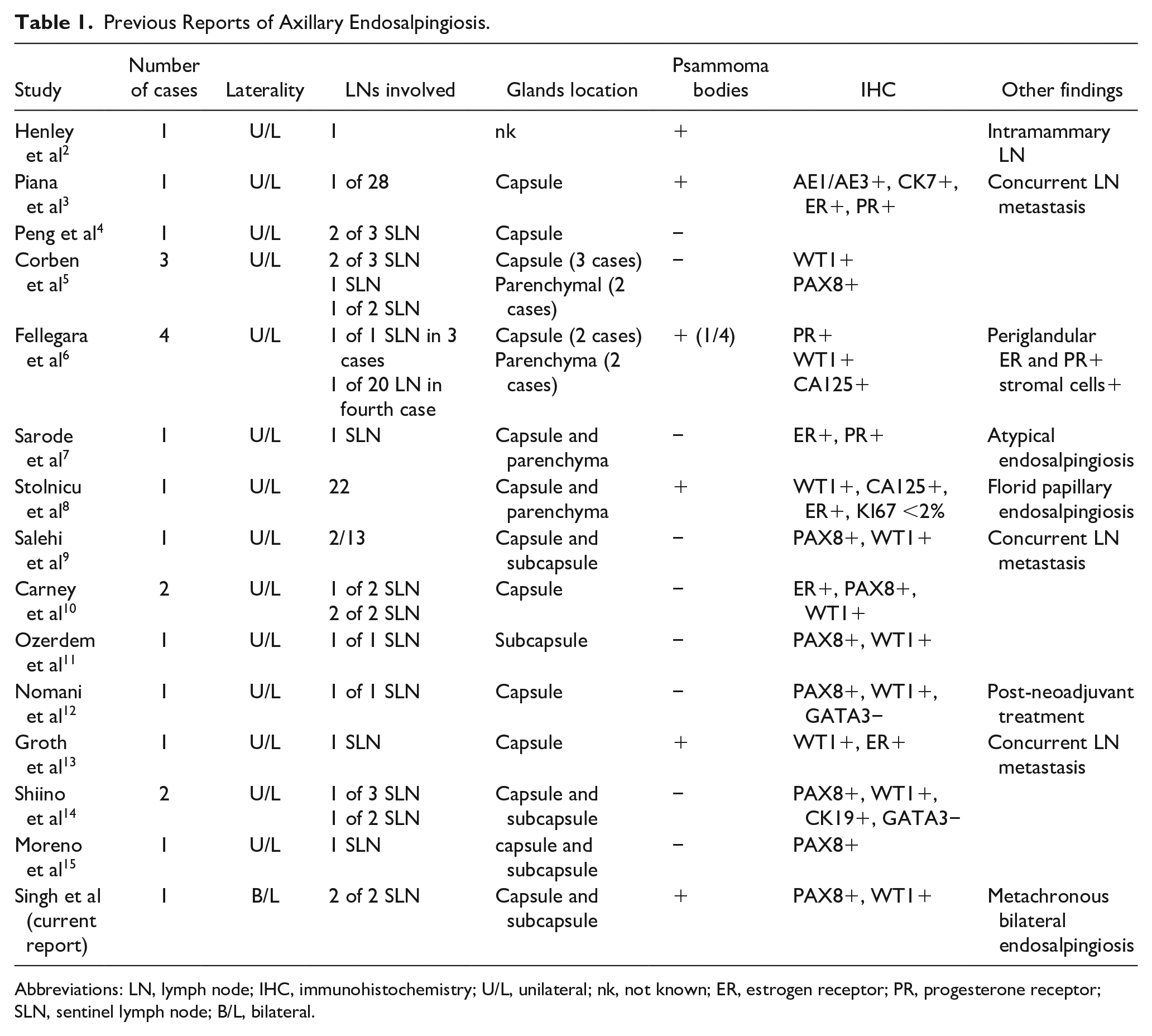
Abbreviations: LN, lymph node; IHC, immunohistochemistry; U/L, unilateral; nk, not known; ER, estrogen receptor; PR, progesterone receptor; SLN, sentinel lymph node; B/L, bilateral.
Case Report
A 77-year-old Caucasian female underwent left breast lumpectomy and axillary SLN sampling for histologic grade 2 invasive carcinoma of no special type (ductal). She was otherwise in good health, with no history of gynecological malignancy. During an intraoperative evaluation, the microscopic examination of the left axillary SLN revealed well-formed glands in the lymph node capsule (Figure 1A). The glands were focal and spanned 0.5 mm. A micrometastasis was suspected on the frozen section examination, and the definite diagnosis was deferred to permanent sections. The glands were lined by Mullerian-type epithelium composing of low columnar cells with scattered ciliated cells. Psammomatous calcifications were present. By immunohistochemistry, no myoepithelial cells (p63 and calponin) were identified, and the glands showed nuclear positivity for WT-1 and PAX-8. A diagnosis of endosalpingiosis was rendered. Two other SLNs were benign.
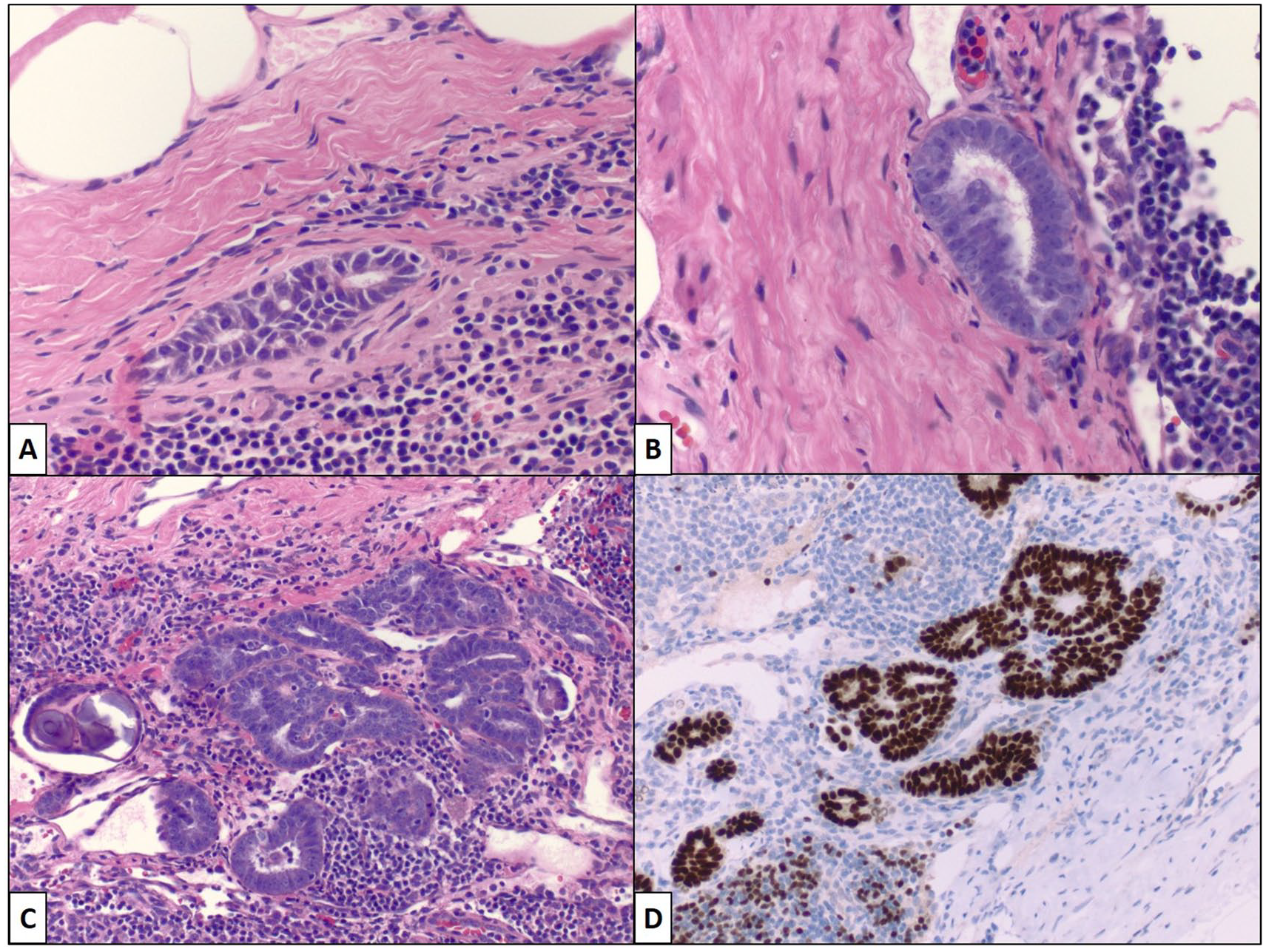
Endosalpingiosis involving axillary lymph nodes. Left (A) and right (B-D) axillary lymph nodes with benign Mullerian-type glands embedded in the lymph node capsule and subcapsular tissue. The luminal border displays terminal bars and cilia (B) and glands are PAX8 positive (D).
Eight years later, the patient underwent a right breast localized excision and right axillary SLN sampling for multifocal invasive lobular carcinoma. One of the 2 sentinel lymph nodes was remarkable for the presence of circumferentially dispersed well-formed glands in the lymph node capsule and subcapsular tissue. The inclusions were lined by a benign-appearing single layer of low columnar epithelium interrupted by ciliated cells (Figure 1B and C). Psammomatous calcifications were present. No mitotic activity was noted, and Ki-67 immunostaining highlighted a rare nucleus. The diagnosis of endosalpingiosis was confirmed by positive nuclear PAX-8 (Figure 1D) and WT-1 immunostaining. The follow-up abdominal imaging was unremarkable.
Discussion
Sampson first used the term “endosalpingiosis” in 1930; it represents glands lined by benign epithelium recapitulating the normal mucosa of the fallopian tube. 18 The incidence of endosalpingiosis in axillary SLNs is estimated to be 0.1%. 14 In the published English literature, we found 20 cases of axillary lymph node endosalpingiosis, all of which were unilateral.2-15 To the best of our knowledge, this is the first case of endosalpingiosis involving bilateral axillary lymph nodes (metachronously). It is important to note that 2 previously published cases of axillary endosalpingiosis with atypical features, later presented with low-grade serous carcinoma in the gynecological tract.16,17 Conversely, 2 cases, each of atypical and florid papillary endosalpingiosis of axillary lymph nodes did not have any Mullerian lesion on presentation, or follow-up.7,8 These observations suggest that a primary Mullerian lesion should be excluded when superimposed hyperplastic changes complicate nodal endosalpingiosis. Our patient had bilateral axillary nodal endosalpingiosis; however, follow-up radiologic workup was negative for gynecological lesion. Interestingly, endosalpingiosis involving intramammary lymph node can present with calcifications on a routine mammogram. 2 Although the epithelium of endosalpingiosis is keratin-19 positive, the 1-step nucleic acid amplification assay revealed negative results on the involved axillary SLNs. 14
The critical message of this report is to make pathologists aware of the pitfall where benign epithelial rests involving the axillary lymph node can mimic metastatic carcinoma. The differential diagnoses of axillary SLN epithelial deposits include metastasis, displaced benign and malignant mammary epithelium, and benign epithelial inclusions. 1 The right axillary epithelial inclusions in our case were interpreted as suspicious for carcinoma. Other studies have cautioned this pitfall to avoid unnecessary axillary dissection or adjuvant treatment.5,9 The distinction of benign epithelial rests from metastasis can be challenging, especially during the frozen section examination. Knowledge of breast carcinoma histologic type and histologic grade, and morphological comparison of the primary breast carcinoma with the nodal epithelial deposits can help when deposits are small and limited to the fibrous capsule. Most benign epithelial inclusions are limited to the lymph node capsule. When endosalpingiosis is suspected, the presence of psamommatous calcifications, absence of nuclear atypia, and the presence of terminal bars or cilia will clinch the diagnosis. The rounded expansile epithelial nests populated by solid sheets of epithelial cells with cytoplasmic clearing, and bland-appearing round to oval nuclei with spindling and squamoid features are seen with benign mammary inclusions. The mammary-type epithelial inclusions can display a spectrum of proliferative changes that are seen in native breast tissue. 6 Demonstration of an intact myoepithelial layer on permanent sections will confirm benign nature and mammary differentiation in this setting.
The displaced mammary epithelium is another incidental histological finding that can mimic micrometastasis. 19 The variable-sized epithelial clusters of displaced benign mammary tissue usually populate the capsular and subcapsular sinuses. The displaced epithelium shows heterogeneity in the cell population, and often shows admixed inflammatory cells including lymphocytes and histiocytes, some of which can also show hemosiderin pigment. The displaced epithelium is often identified in a setting of a papillary lesion. The morphological comparison with primary breast carcinoma can help distinguish displaced epithelium from metastasis. Otherwise, the demonstration of a mixed epithelial population by myoepithelial immunohistochemical markers and variable heterogeneous estrogen receptor expression can confirm the benign nature of the displaced epithelium. With ambiguous morphology, an immunohistochemical panel consisting of p63, smooth muscle myosin heavy chain, ER, PAX8, and GATA3 can help in the differential diagnosis of axillary lymph node epithelial deposits. The myoepithelial cells are absent in endosalpingiosis and displaced mammary carcinoma cells; a pitfall that one should be aware of while working up lymph node epithelial deposits.
In conclusion, endosalpingiosis of axillary lymph nodes is a rare lesion. Pathologists should exercise caution while diagnosing microscopic epithelial deposits involving axillary lymph nodes, especially during the frozen section examination. A careful microscopic examination supplemented by immunohistochemistry can differentiate metastasis from benign epithelial inclusions of the lymph node.
Footnotes
Author Contributions
RS: Data curation, writing; KS: Conceptualization, writing, reviewing, and editing; MRQ: Photographs and editing; MH: Conceptualization, writing, and reviewing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.