
Abstract
Thymic typical and atypical carcinoids are rare and appear to be more aggressive than similar tumors in other sites. We retrospectively analyzed a group of biomarkers that hold therapeutic and prognostic utility, in 27 of these tumors. All cases were immunohistochemically stained with PAX5, MET, CRMP5, paxillin, p21, p27, EZH2, PDL-1, and Ki-67, and then H-scored. Clinicopathologic and survival data were statistically analyzed against staining (χ2 test). Five- and 10-year-survival rates were 53% and 18%, respectively. Mitotic counts ≥4 per 2 mm2 and tumor size ≥5 cm, associated with death of disease (DoD; P = .010 and .016). Ki-67 expression ≥1% associated with DoD (P = .003) and death within 5 years (P = .031). Biomarkers stained tumor cases as follows: PDL-1 = 0%, PAX-5 = 0%, MET = 7.4%, paxillin = 41%, CRMP5 = 78%, p21 = 63%, p27 = 63%, EZH2 = 37%, and MASH1 = 59%. Overall ± staining did not associate with survival or grade. Cases with low CRMP5 H-scores (<80) associated with DoD (P = .002), while CRMP5 H-scores >80 associated with 10-year survival (P = .022). Cases with high MASH1 H-score (>100) associated with DoD (P = .021). Accurate grading and staging remain paramount in predicting clinical outcome. Biomarkers may have significance in subsets of patients and the use of these studies likely should be focused on a more personalize type of approach.
Introduction
Low- and intermediate-grade neuroendocrine neoplasms (typical and atypical carcinoids) represent <5% of all mediastinal tumors. They may present at any age, can be associated with various paraneoplastic- and endocrine-related syndromes, and have a male predilection of approximately 3:1.1-4 It has been stated that thymic neuroendocrine neoplasms of low- and intermediate-grade appear to have a more aggressive course than their counterparts in other anatomic areas.1-9
Depending on the grade and stage, treatment for these tumors is surgical resection with or without chemotherapy and radiation.6,7 The data available to guide treatment are limited, but surgical resection has been shown to improve overall survival and remains the treatment of choice. Chemotherapy is regarded as an adjunctive option, although resistance has been shown to occur. 7 Neoadjuvant therapy with chemotherapy and radiation has shown some success in decreasing the size of the tumor in locally advanced disease, albeit only in a couple of case reports with limited follow-up intervals.8,9 In larger series of these tumors, it has been observed that the 5-year survival rates for low-grade neoplasms is approximately 50%, while for intermediate-grade neoplasms it is 25%. 10 Currently, with advancements in targeted immunological and inhibitor therapies, remarkable responses are being observed in subsets of patients with other solid tumor types. Even though there are reports on neuroendocrine tumors, much remains to be established with regard to information on predicting outcomes and potential responses to such therapies in patients with thymic low- and intermediate-grade neuroendocrine neoplasms. Therefore, in the current study, we have focused our efforts on a very specific group of neuroendocrine neoplasms (thymic neuroendocrine) attempting to highlight the potential use of these biomarkers and their possible therapeutic significance.
Materials and Methods
Materials
Twenty-seven cases of thymic neuroendocrine neoplasms (low and intermediate grade) were identified in the files of the Department of Pathology at MD Anderson Cancer Center and the personal files of one of the authors (CAM; 1995-2015). All available hematoxylin-eosin sections were available for review and all the cases were reviewed and graded according to current standards. All the patients’ demographic information was entered in a common database and subsequently correlated with the different biomarkers studied. This study was performed with an approved institution review board protocol.
Methods
Biomarker Staining
Representative unstained sections obtained from formalin-fixed paraffin-embedded tumor tissue blocks were used to perform immunohistochemical studies using automated staining instruments and antibody detection kits (Table 1). All staining was performed according to vendor’s instructions. Negative and positive controls were included in all studies.
Biomarker Manufacturer Details and Staining Protocol.
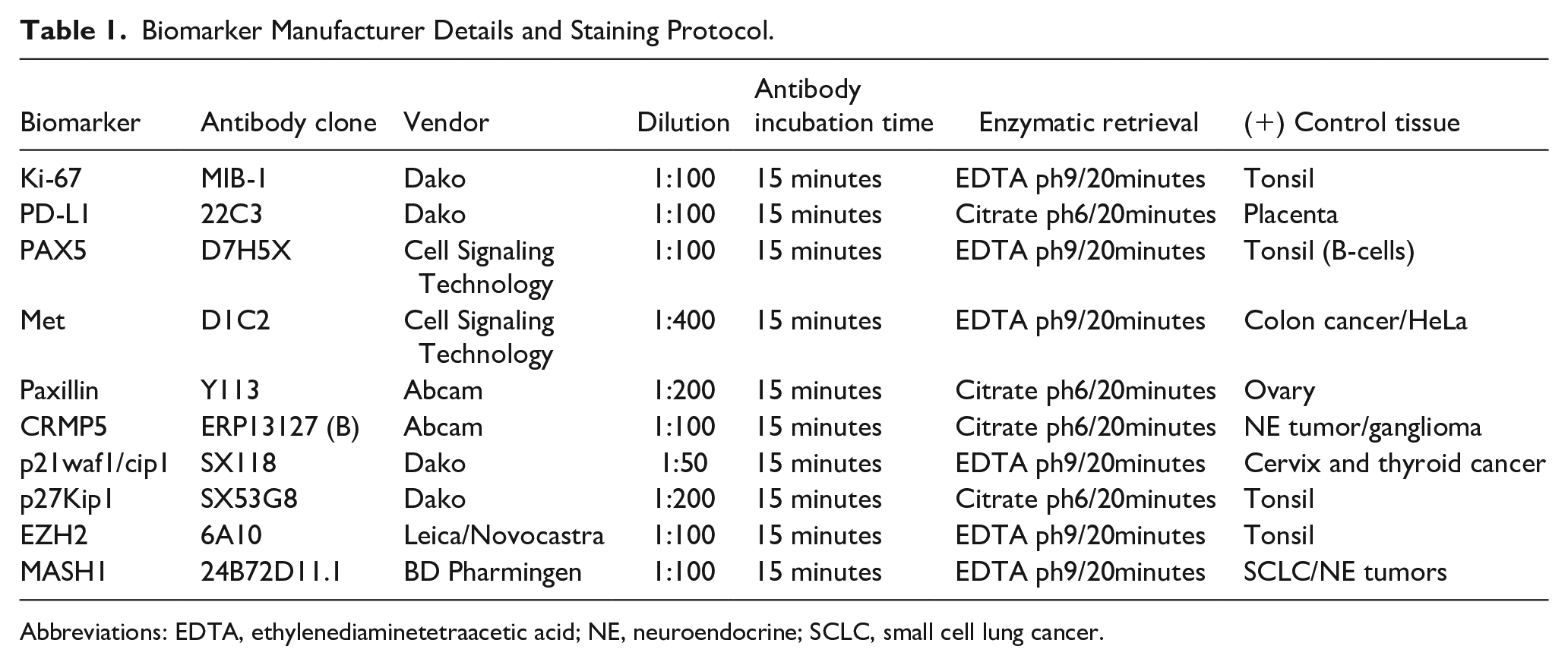
Abbreviations: EDTA, ethylenediaminetetraacetic acid; NE, neuroendocrine; SCLC, small cell lung cancer.
PAX5 tumor cell staining was scored on a sliding scale of 0 to 4+ according to the percentage of reactive cells (0, negative; 1+, 1% to 25%; 2+, 26% to 50%; 3+, 51% to 75%; 4+, 76% to 100%). The staining intensity was graded as weak, intermediate, or strong. PD-L1 expression was scored depending on the percentage of tumor cells showing membranous staining (0% to 100%). CRMP5 (collapsin response-mediator protein-5), Paxillin, p21waf1/cip1, p27Kip1, EZH2 (enhancer of Zeste Homolog 2), MET, and MASH1 (Mammalian achaete-scute complex-like 1) were scored as percent of tumor cell positivity (nuclear, cytoplasmic, membranous) relative to all tumor cells and intensity of the staining was assigned as 1, 2, or 3, corresponding to weak, moderate, and strong. From the tumor cell staining patterns, H-scores were calculated as follows: H-Score = % positive tumor cells × intensity. Ki-67–positive nuclear labeling was obtained via image analysis, performed with the instrument Arperio AT2 (Leica), and quantitated using the software Arperio ScanScope (v12.0.1.5027; Leica).
Statistical Analysis
All data were statistically analyzed using IBM SPSS Version 24 for Windows (SPSS Inc). Chi-square tests were performed to evaluate potential correlations between tumor characteristics (size, presence of necrosis, biomarker staining pattern, mitotic activity, and grade) and disease-specific survival, as well as correlations between biomarker staining patterns and grade. Logistic regression analysis was performed to evaluate for significance between patient’s age and disease-specific survival. The Kaplan-Meier method was used to plot survival curves then differences between these curves were analyzed for significant differences using the log-rank test.
Cutoff values for analyzing Ki-67, tumor size, and mitotic index were established by receiver operating characteristic (ROC) analysis, performed using raw data from each categorical group against each survival category (disease-specific survival, 5- and 10-year survival). The cutoff value for Ki-67 for analyzing death within 5 years was determined to be 0.47, with a sensitivity of 88% and a specificity of 74%, an area under the curve (AUC) of 0.842 (P = .006) at a 95% confidence interval. ROC curves for Ki-67 against disease-specific death (DSD) and 10-year survival, demonstrated AUCs of 0.692 and 0.25, respectively, which are unacceptable for use in cutoff selection (<0.7). On review of local maxima and minima for these parameters, the Ki-67 cutoff values of 0.5 and 1 were chosen as reasonable cutoff for each categorical group, respectively. ROC curves for mitotic count and survival data demonstrated AUCs of <0.7 for each survival category, thus on review of the local maxima and minima, the mitotic cutoff value of 4 was chosen as a reasonable cutoff for each survival group. ROC curve for tumor size and DSD showed a cutoff value of 5 cm to have 92% sensitivity and 65% specificity, with an AUC of 0.832 (p = .003) at a 95% confidence interval. ROC curves for tumor size against 5- and 10-year survival-generated curves with AUC of <0.7; thus, the cutoff value of 5 cm was chosen for analysis.
Results
Clinical Features
The 27 patients with low- and intermediate-grade thymic neuroendocrine neoplasms are 21 males and 6 females with an age range from 20 to 89 years (mean 49 years). Clinically, the patients presented with nonspecific symptoms of cough, dyspnea, and chest pain. Diagnostic imaging revealed the presence of an anterior mediastinal mass. Complete surgical resection of the mediastinal mass with intent to cure or complete remission (R0 resection) was performed via thoracotomy.
Pathological Features
Grossly, tumors were described as tan, ovoid tumor masses with infiltrating borders. In some cases, areas of hemorrhage were described. The tumor measurements ranged from 2 to 20 cm in greatest diameter. Nineteen tumors measured more than 5 cm in greatest diameter.
Histologically, the tumors show the classical features of a nested growth pattern with a discrete fibrovascular tissue. Areas of neoplastic cells arranged in festoons, ribbons, with presence of Rosettes observed in all the cases. Oncocytic features were observed in 4 cases, while spindled cell morphology was observed in 1 case. Areas of necrosis in the form of comedo-like necrosis were present in 11 cases. Mitotic activity was variable and ranged from 1 to 10 mitotic figures per 2 mm2 (22 eyepiece). Eighteen cases were classified as intermediate grade (atypical carcinoid) and 9 cases as low grade (typical carcinoid; Figure 1A and B).
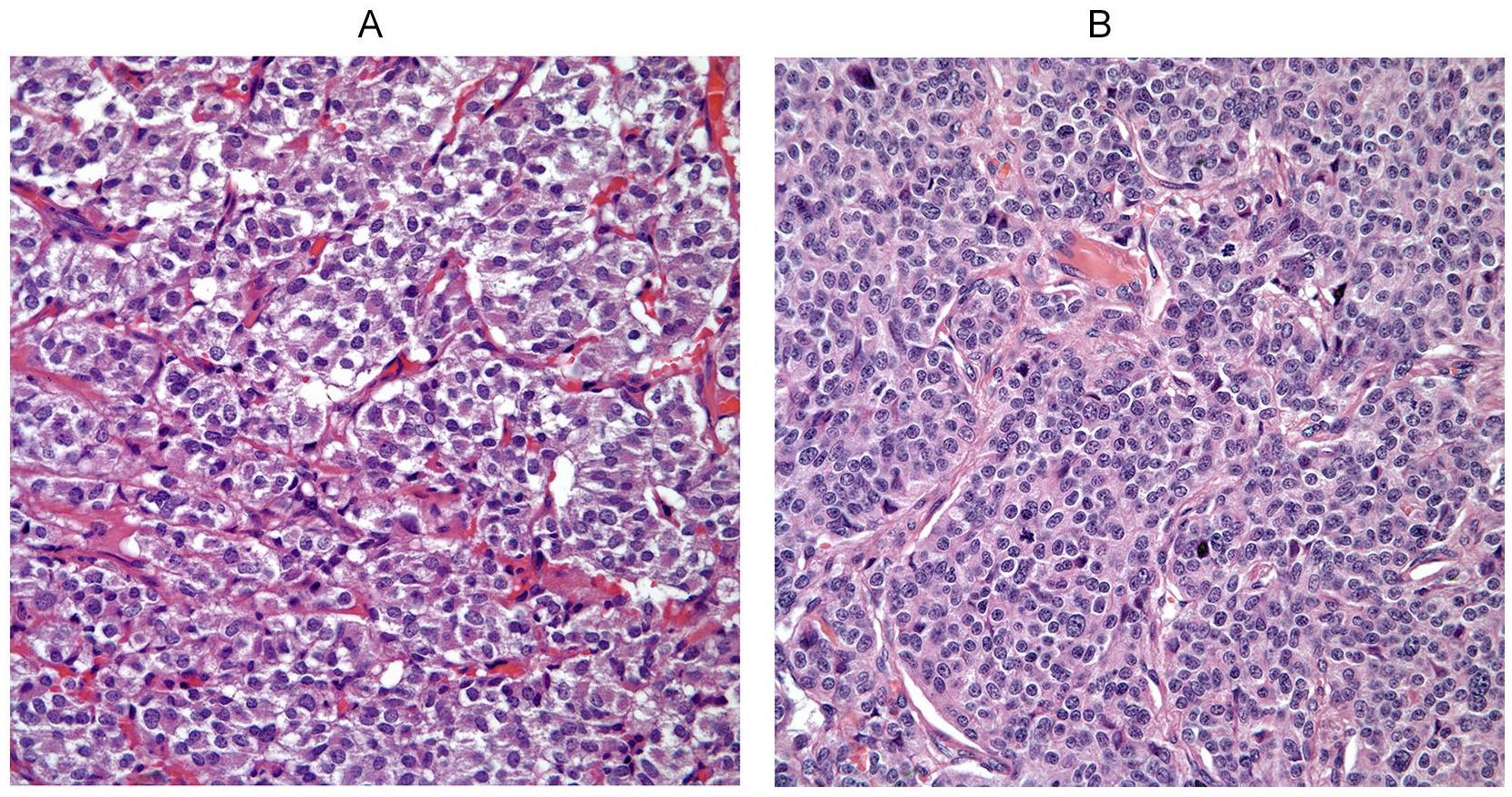
(A) Carcinoid tumor of the mediastinum showing a subtle-nested pattern with mild nuclear atypia and absence of mitotic activity. (B) Atypical carcinoid tumor in which mitotic activity is easily identifiable (hematoxylin and eosin–stained sections, 40×).
Immunohistochemical Features
Ki-67% via automated analysis ranged from 0.01615% to 8.47294% (Figure 2A). Nineteen of our cases had a Ki-67% nuclear positivity of <1%, while 6 cases had a Ki-67% nuclear positivity within the 1% to 3% range, and only 2 cases had a Ki-67% nuclear positivity above 5% (Table 2). Chi-square comparison between Ki-67% and mitotic counts showed no association when assigning cutoff values of Ki-67% nuclear positivity at 0.1%, 0.3%, or 1% with a mitotic count cutoff of 1 mitosis per 2 mm2. Furthermore, a Ki-67%-positive nuclear expression with a cutoff of 1% did not associate with grade (P = .166).
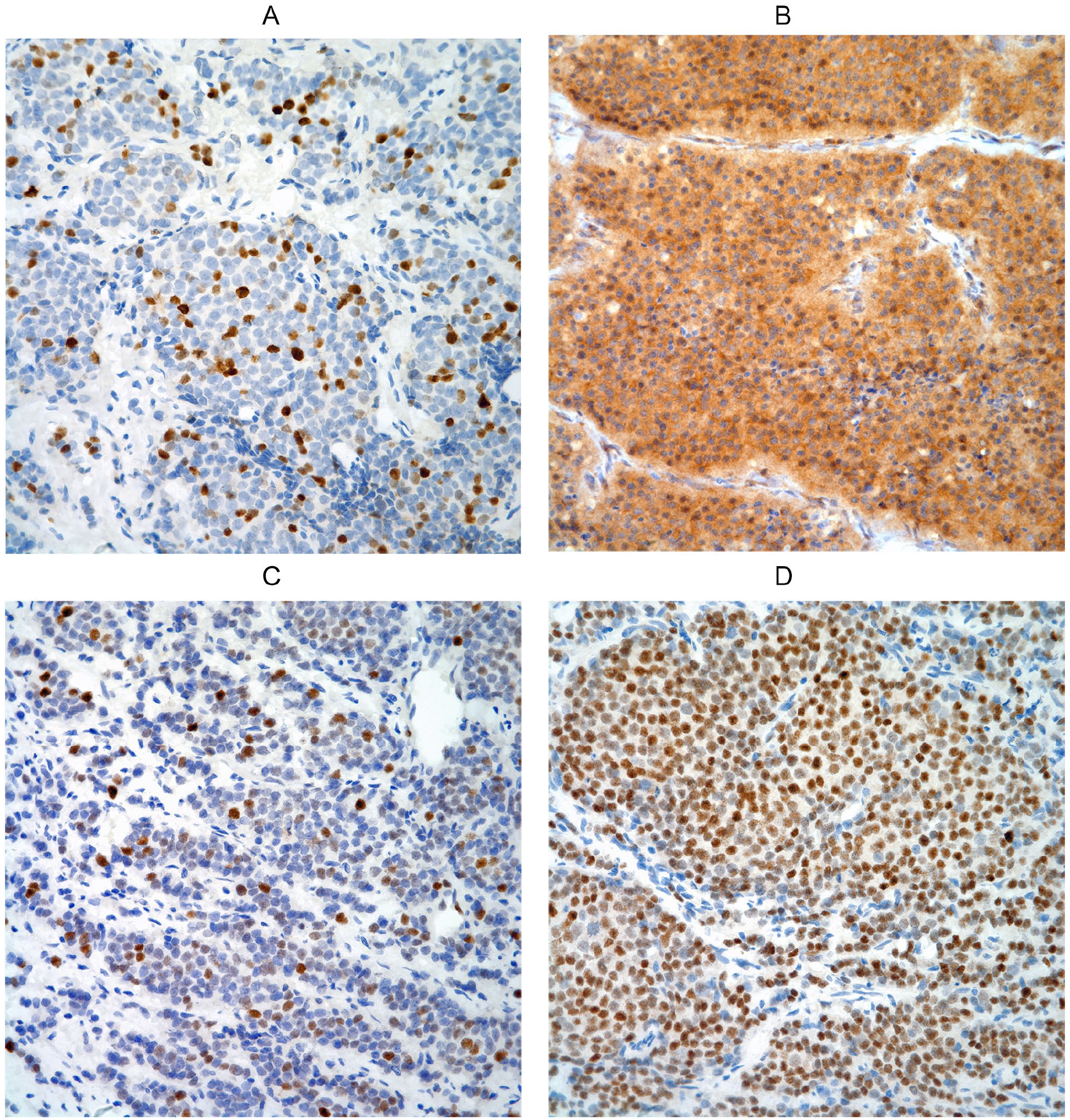
(A) Ki-67 immunostain showing >5% of nuclear labeling (40×). (B) CRMP5 immunostain showing positive cytoplasmic staining in tumor cells (40×). (C) EZH2 immunostain showing positive nuclear staining in tumor cells (40×). (D) MASH1 immunostain showing positive nuclear staining in the majority of tumor cells (40×).
Biomarker Staining Pattern of Location, Tumor Cell Positivity, and Staining Intensity, and Relationship to Survival.
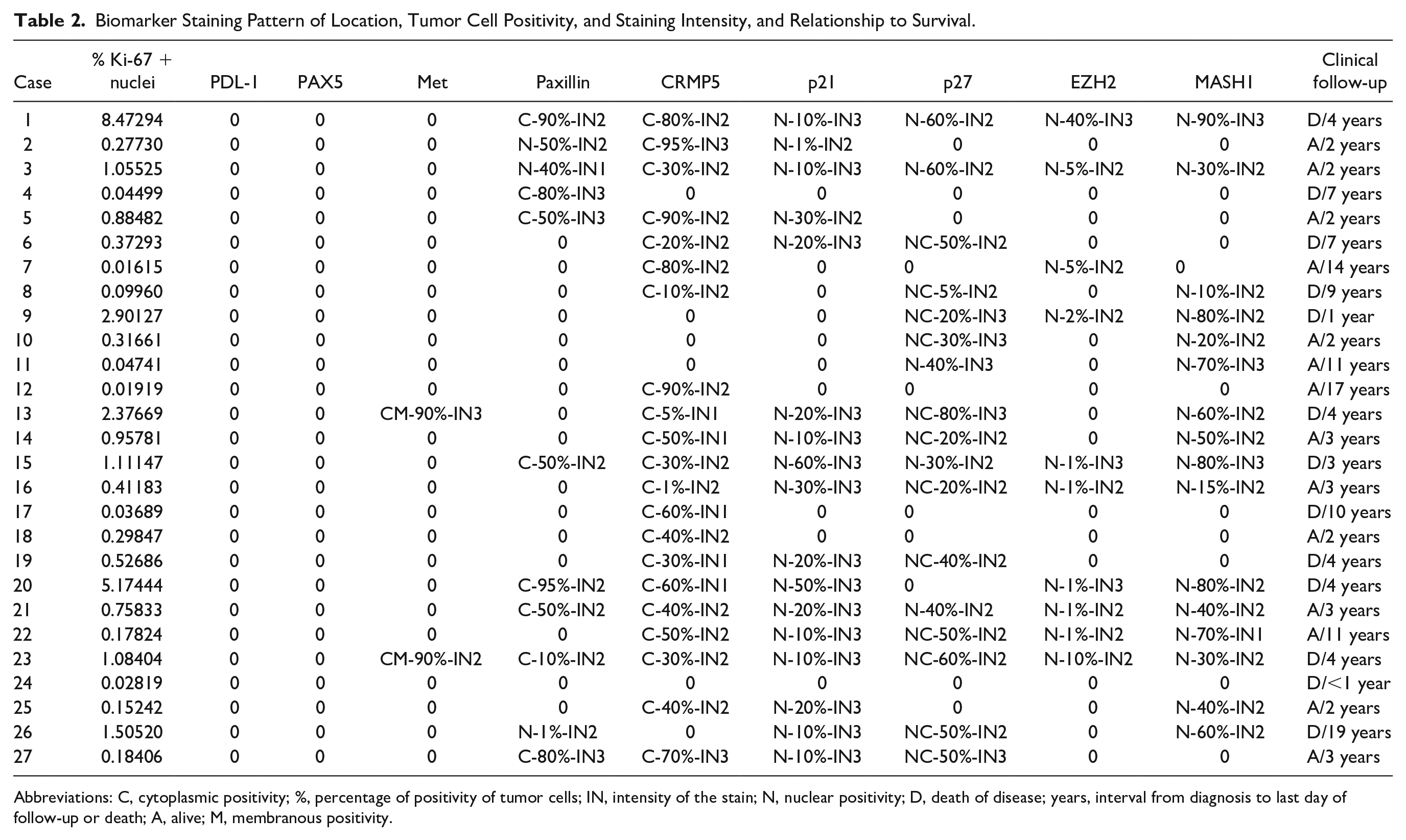
Abbreviations: C, cytoplasmic positivity; %, percentage of positivity of tumor cells; IN, intensity of the stain; N, nuclear positivity; D, death of disease; years, interval from diagnosis to last day of follow-up or death; A, alive; M, membranous positivity.
As displayed in Table 2, all of our cases were completely negative for PDL-1 (programmed death-ligand 1; negative membranous staining in tumor cells) and PAX-5. MET showed positive cytoplasmic and membranous tumor cell reactivity in 2/27 cases (7.4%), with 90% of the tumor cells showing reactivity with intensities of 2+ and 3+. Paxillin was reactive in 11/27 cases (41%). Tumor cells displayed cytoplasmic staining in 8 cases and nuclear staining in 2 cases with a range of tumor cell positivity from 1% to 80%, and staining intensities from 1+ to 3+. CRMP5 was reactive in 21/27 cases (78%), all with cytoplasmic expression and a range of tumor cell positivity from 1% to 90% and staining intensities from 1+ to 3+ (Figure 2B). P21 was reactive in 17/27 cases (63%), all with nuclear expression and a range of tumor cell positivity from 1% to 60% and staining intensities of 2+ or 3+. P27 was reactive in 17/27 cases (63%), with either nuclear or nuclear and cytoplasmic staining but none with cytoplasmic staining alone. Tumor cell positivity ranged from 5% to 80% with staining intensities of 2+ or 3+. EZH2 was reactive in 10/27 cases (37%), all with nuclear expression and a tumor cell positivity ranging from 1% to 40% and staining intensities of 2+ or 3+ (Figure 2C). MASH1 was reactive in 16/27 cases (59%) with tumor cell positivity ranging from 10% to 90% with staining intensities ranging from 1+ to 3+ (Figure 2D).
Overall positive or negative antibody expression did not statistically associate with survival or tumor grade. Positive staining with relatively high or low H-scores did not associate with tumor grade.
Clinical Follow-up
Follow-up time ranged from 1 to 19 years. For cases with appropriate follow-up time intervals (17 cases), 5- and 10-year survival rates were at 53% and 18%, respectively. Ki-67 expression of 1% or more significantly associated with death of disease (P = .003) and death within 5 years (P = .031), but not with 10-year survival. A Ki-67 index of 0.5% or more associated with death in 5 years (P = .002), but not with DSD or 10-year survival. Only 2 of our cases had a Ki-67% nuclear positivity above 5%, which is too few for a meaningful statistical analysis. Cases with mitotic counts of 4 or more per 2 mm2 significantly associated with death of disease (P = .010), but not 5- and 10-year survival. Mitotic counts of 1 to 3 mitosis per 2 mm2 did not associate with patient death, or 5- and 10-year survival. Tumor size of 5 cm or greater significantly associated with death of disease (P = .016), but not 5- and 10-year survival. The presence of necrosis did not associate with survival. Logistic regression analysis showed no association between age and death of disease.
Chi-square tests comparing biomarker’s staining patterns with DSD, and 5- and 10-year survival showed that MASH1 overall positivity did not associate with death, or 5- and 10-year survival. Cases with a relatively high MASH1 H-score (>100) associated with death (P = .021), but did not associate with 5- and 10-year survival. CRMP5 overall positivity did not associate with death, or 5- and 10-year survival. A relatively low CRMP5 H-score (<80) associated with death (P = .002), while CRMP5 H-scores over 80 associated with survival at 10 years (P = .022), but not at 5 years (P = .312). P21 and p27 overall positivity and high H-scores (>30 and >100, respectively) did not associate with death, or 5- and 10-year survival. EZH2 stained only 10 cases with relatively low H-scores. EZH2 overall positivity and positivity at relatively high H-scores (>10) did not associate with death or 5- and 10-year survival. Paxillin overall positivity and high H-score (>100) did not associate with death, or 5- and 10-year survival. Only 2 cases stained positive for MET that was too few to run a meaningful statistical analysis; however, both patients died at 4 years.
Discussion
Over the years, the use of innovative biomarkers in the assessment of neuroendocrine neoplasm with the idea of bringing new approaches to treatment have been reported in the literature. Song et al 11 evaluated the expression of PAX5, c-MET, and paxillin in 89 neuroendocrine neoplasms of the lung including typical (38 cases) and atypical carcinoids (6 cases), small cell carcinoma (34 cases), and large cell neuroendocrine carcinoma (11 cases) using tissue microarrays. The authors observed different expressions of these markers in the different types of neuroendocrine neoplasms and concluded that the co-expression of PAX5 with c-MET or phosphorylated c-MET in intermediate- and high-grade tumors was in favor of the treating these patients with strategies to co-inhibit those proteins. Also Meyronet et al 12 focusing more in high-grade neuroendocrine carcinomas of the lung observed 98.6% expression of CRMP5 in these tumors. Some of these biomarkers have been evaluated in similar tumors in other anatomical areas. For instance, Mpilla et al 13 evaluated pancreatic neuroendocrine tumors for p21-activated kinase 4 (PAK4) as a possible therapeutic target. Sadowski et al 14 also evaluated p27/p18 in pancreatic neuroendocrine tumors in MEN1 patients. On the other hand, Roininen et al 15 evaluated p27 in neuroendocrine carcinomas of the breast identifying significant nuclear overexpression, which appear to correlate with longer cancer-specific survival. Kwon et al 16 focusing on small cell carcinoma of the prostate evaluated the expression of EXH2. The authors concluded that overexpression of EZH2 was associated with short overall survival. On the contrary, Krushkal et al 17 observed that EZH2 was associated with response to Aurora kinase inhibitors and a FGFR inhibitor. On the contrary, PDL-1 has become a broader biomarker essentially in non–small cell carcinomas of the lung; however, PDL-1 has also been reported as potential therapeutic targets for women with high-grade neuroendocrine carcinomas of the cervix. Carroll et al 18 evaluated 40 such cases in which the authors concluded that PD-L1 expression was not present in their cases evaluated.
Based on this background, we determined to focus the study of some of these biomarkers in a subset of neuroendocrine neoplasms that albeit uncommon, represent a therapeutic challenge. Given the emerging targeted therapies under investigational studies and those currently available for treatment, we investigated the immunohistochemical expression of a panel of biomarkers, some of which currently have targeted treatment available, while others have treatment that is currently being investigated in clinical trials, and some that best serve as prognostic indicators with the potential for a therapeutic target in the distant future. Current immunotherapies anti-PDL-1 and tyrosine kinase inhibitors utilize positive immunohistochemical staining for PDL-1, and MET, respectively, to indicate which patients might benefit from each therapy. PDL-1 is an inhibitor receptor notably expressed on the cell surface of cytotoxic T-cells that when engaged by PD-1 ligand present on tumor cells, immunosuppression is mediated allowing for a pro-tumorigenic tumor microenvironment and tumor cell survival. 19 Blocking this interaction with inhibitors may allow for a robust immune response and clearance of tumor cells in subsets of patients with solid tumors.19,20 While MET is a proto-oncogene that encodes a transmembrane MET tyrosine receptor kinase that activates oncogenic molecular pathways including PI3K/AKT/MAPK, which facilitates tumor cell motility and invasion. 21 In patients with non–small cell lung cancer (SCLC), MET immunochemistry staining is a robust predictor of overall survival and progression-free survival with treatment with onartuzumab plus erlotinib. 22 While many patients have had great therapeutic responses to these therapies, it remains to be seen only in a subset of patients; thus, immunohistochemical staining of tumor cells with anti-PDL-1 and MET currently serve as predictive biomarkers to direct therapy with immune checkpoint inhibitors. 23 None of our cases showed positive staining for PDL-1, and only 7.4% had positive expression for MET, which may be an indication that patients with low- and intermediate-grade neuroendocrine neoplasms of the thymus might not benefit from immunotherapy with anti-PDL-1 and only a small subset might benefit from tyrosine kinase inhibitors. It is important to note here that this study is completely retrospective in design and none of the treatments or their effects are being analyzed.
Our cohort showed 37% and 41% of the cases to have positive staining for EZH2 and paxillin, respectively. Biomarker studies with EZH2 and paxillin have shown promising results for potential development of targeted therapies. EZH2 is a methyl transferase that acts as a gene silencer by methylating H3K27, playing a crucial role in cell cycle regulation, and driving malignant transformation of many human cancers.24,25 Paxillin is a scaffold protein that is involved in cellular signaling that aides in the organization of cytoskeletal components (ie, actin) that plays an important role in cell motility, proliferation, survival, and angiogenesis.26-28 Overexpression of these proteins has been shown to associate with elevated aggressive clinical behavior and worse prognosis in several solid tumor types.26,29,30 Furthermore, paxillin overexpression was shown to be an independent predictor of survival and relapse in patients with lung cancer, and targeting suppression of paxillin with microRNAs showed decreased proliferation and migration in human lung cancer cells.31,32 Knockdown of EZH2 in tumor cell culture and in mice-inhibited cancer cell growth, motility, and invasion, 33 and several clinical trials have been established that have shown encouraging results for EZH2 inhibitors to become a targeted therapy. 34
In addition, in our experience we observed that some tumors might show biomarker staining for proteins that hold prognostic significance with positive staining of MASH1 (59%), CRMP-5 (78%), p21waf1/cip1 (63%), p27Kip1 (63%), and a wide range of Ki-67% positivity staining (0.01615% to 8.47294%). MASH1 is a transcription factor, which drives neuroendocrine cell differentiation,35-37 and positive immunohistochemical staining is demonstrated in high-grade neuroendocrine carcinomas, differentiating these from carcinoid tumors.36,38-40 However, the utility of such has not been well established in neuroendocrine neoplasms of the thymus; however, in our cohort of cases with a relatively high MASH1 H-score (>100), we observed association with death (P = .021). CRMP-5 is a protein present in SCLC that is associated with the development of autoantibodies and paraneoplastic neurologic disorders in patients with SCLC, thymoma, and other various solid tumor types. 41 Honnorat et al 42 have demonstrated that patients with SCLC and CRMP5 autoantibodies had increased median survival compared with patients with SCLC and autoantibodies, which correlates with our finding of cases with CRMP5 H-scores over 80 associated with survival at 10 years (P = .022). Interestingly, a relatively low CRMP5 H-score (<80) associated with death (P = .002). Cyclin-dependent kinase inhibitors p21waf1/cip1, p27Kip1, act to negatively regulate the cell cycle and induce apoptosis, when located in the nucleus but in the cytoplasm they possess oncogenic functions by inhibiting apoptosis and promoting invasion.43-45 Immunohistochemical expression of these proteins has been shown to serve as prognostic markers in various solid tumor types.46-48 PAX-5 is a transcription factor protein involved in organ development and tissue differentiation, 49 and is overexpressed in poorly differentiated neuroendocrine carcinoma (ie, small cell carcinoma) and Merkel cell carcinoma, but negative in typical carcinoid tumors.49-51 We observed similar results as none of our 27 cases of low- and intermediate-grade neuroendocrine neoplasms show positive staining. Ki-67 is often used as a reliable prognostic indicator of cellular proliferation that is expressed in all phases of the cell cycle (G1, S, G2, and M), but undetectable in cells in G0 or the resting phase. Our results show that cases with Ki-67 tumor cell expression of over 1% associate with death; however, it is interesting to note that our Ki-67 expression patterns did not associate with mitotic activity, which is in keeping with Rudolph et al, 52 who have shown that Ki-67 expression and mitotic activity may not always correlate, and in fact sometimes display inverse relationships.
In short, based on our experience with this panel of biomarkers, we consider that the prognosis of low- and intermediate-grade neuroendocrine neoplasms of the thymus is best estimated by combining grade and stage at the time of diagnosis. The use of biomarkers is important and crucial in order to determine targets that could be used for treatment purposes to improve the survival rate in this group of patients. However, the use of biomarkers needs to be more individualized from case to case rather than seen all these biomarkers as an overall feature of these tumors. Even though we were not able to observe a statistical significance between the overall positive staining of any of these biomarkers and the survival of these patients, the fact that some of these biomarkers showed positive staining in some of these tumors and that positive tumor cell staining at relatively high percentages and intensities associated with survival for MASH1 and CRMP5, raises the importance of pursuing larger studies and possibly expanding any study with other biomarkers. However, we are fully aware that the anatomical site chosen for our study represents only a small subset of these tumors in the general scheme, as the great majority of these neoplasms (carcinoid tumors) occur in the gastrointestinal area. Therefore, our findings should not be construed as representing the entire spectrum of neuroendocrine neoplasms body length. As far as thymic neuroendocrine neoplasms, it is possible that at the individual level some targeted treatments may aid in the survival.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was performed with an approved institution review board protocol.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.