
Abstract
Adenomyoepithelioma (AME) of the male breast is a rare tumor characterized by biphasic proliferation of gland epithelial cells and myoepithelial cells. Though pleomorphic adenoma (PA) is also known to be an epithelial-myoepithelial tumor in the breast, and these tumors are considered to exist on the same spectrum by some authors, to the best of our knowledge, there have been no reports of a clear transition from AME to PA in the male breast. Therefore, the case of an 85-year-old man with AME with PA-like components is presented.
Keywords
Introduction
Adenomyoepithelioma (AME) of the breast is a tumor characterized by biphasic proliferation of inner gland epithelial cells and prominent outer myoepithelial cells that was first described by Hamperl in 1970 and further classified by Tavassoli in 1991. 1 A few cases of male AME have been reported.2-4 Pleomorphic adenoma (PA) in the breast is a rare epithelial-myoepithelial tumor, the counterpart of the more common salivary gland tumor. 5 A case of male mammary AME that partially transformed to a PA-like component is presented. This clear transition has not been previously reported in the male breast.
Case Report
An 85-year-old man visited our hospital with a lump in the right breast. Ultrasonography showed the lump to be a well-defined cystic mass beneath the areola and multiple hypoechoic lesions in and outside of the cystic mass. The mass measured 24 mm. On examination of the biopsy specimen, the diagnosis was intraductal papilloma with sclerotic changes, and partial resection was performed. The patient was followed-up again 5 months after surgery; since there were no findings of recurrence, follow-up was terminated.
Macroscopically, the tumor measured 28 × 15 × 14 mm3 and was a tan-white solid mass with an area of cystic and hemorrhagic lesions. In the edge of the tumor, multiple branched glossy white nodules were found (Figure 1).
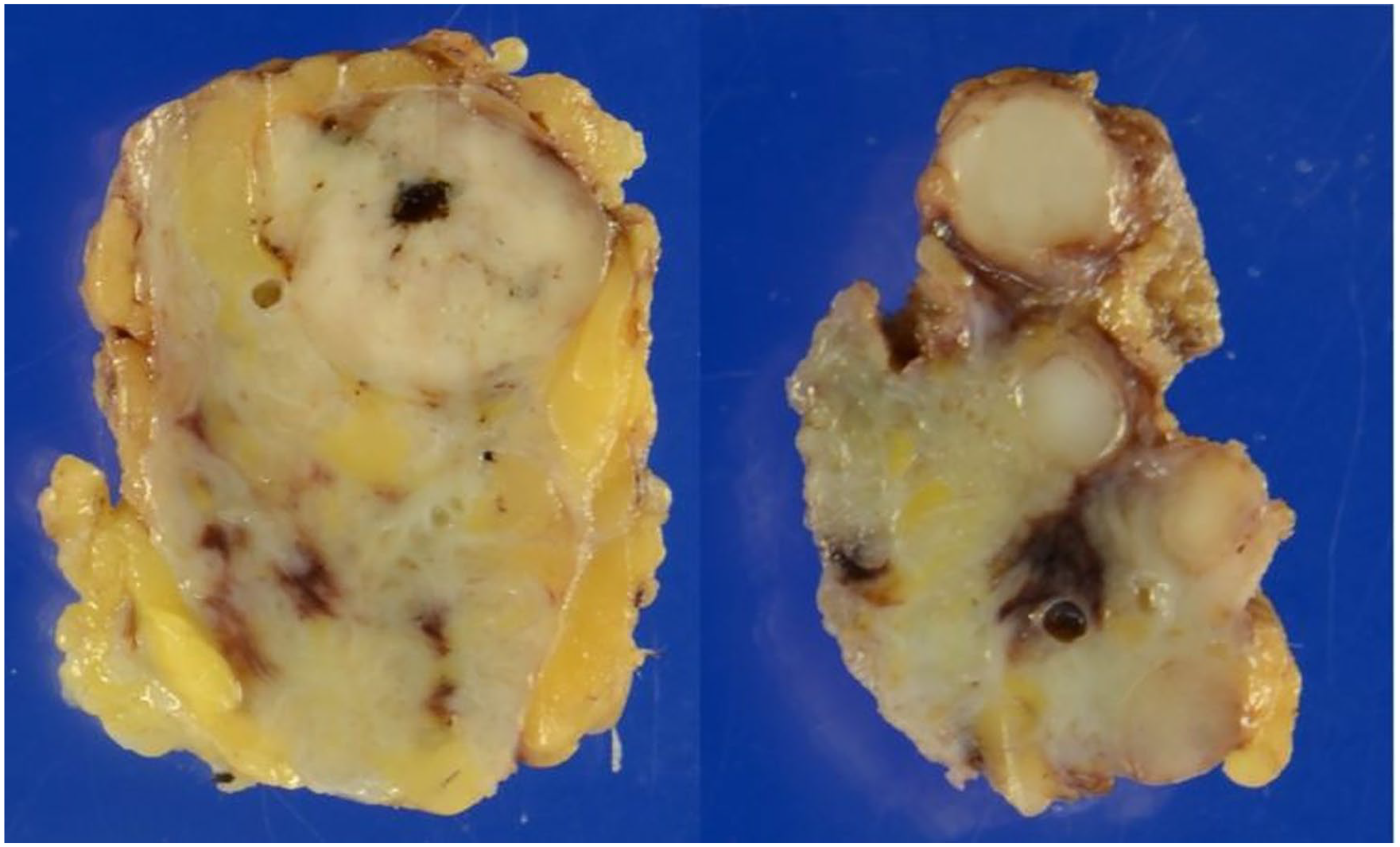
Gross findings. Left above: tan-white circumscribed solid mass with focal hemorrhage (adenomyoepithelioma component). Right: multiple branched glossy white nodules (pleomorphic adenoma component) in the edge of the tumor.
Microscopically, the tumor consisted of 2 continuous components (Figure 2). One component showed biphasic proliferation of both luminal and myoepithelial cells, composed of ductular, trabecular, and papillotubular patterns (Figure 3). They were separated by strands of eosinophilic basement membrane. Luminal cells showed hyperplasia and partial apocrine differentiation. Myoepithelial cells with clear cytoplasm were more prominent than luminal cells. No necrosis, cytological atypia, or increased mitoses were found. The tumor was circumscribed, with no infiltrating border, and it lacked a fibrous capsule. Another component was seen in the edge of the tumor, with transition to PA-like nodules with abundant myxochondroid matrix. Myxochondroid stroma formation was seen in the center of the nodule, surrounded by tubular epithelial cells and spindle or stellate myoepithelial cells.
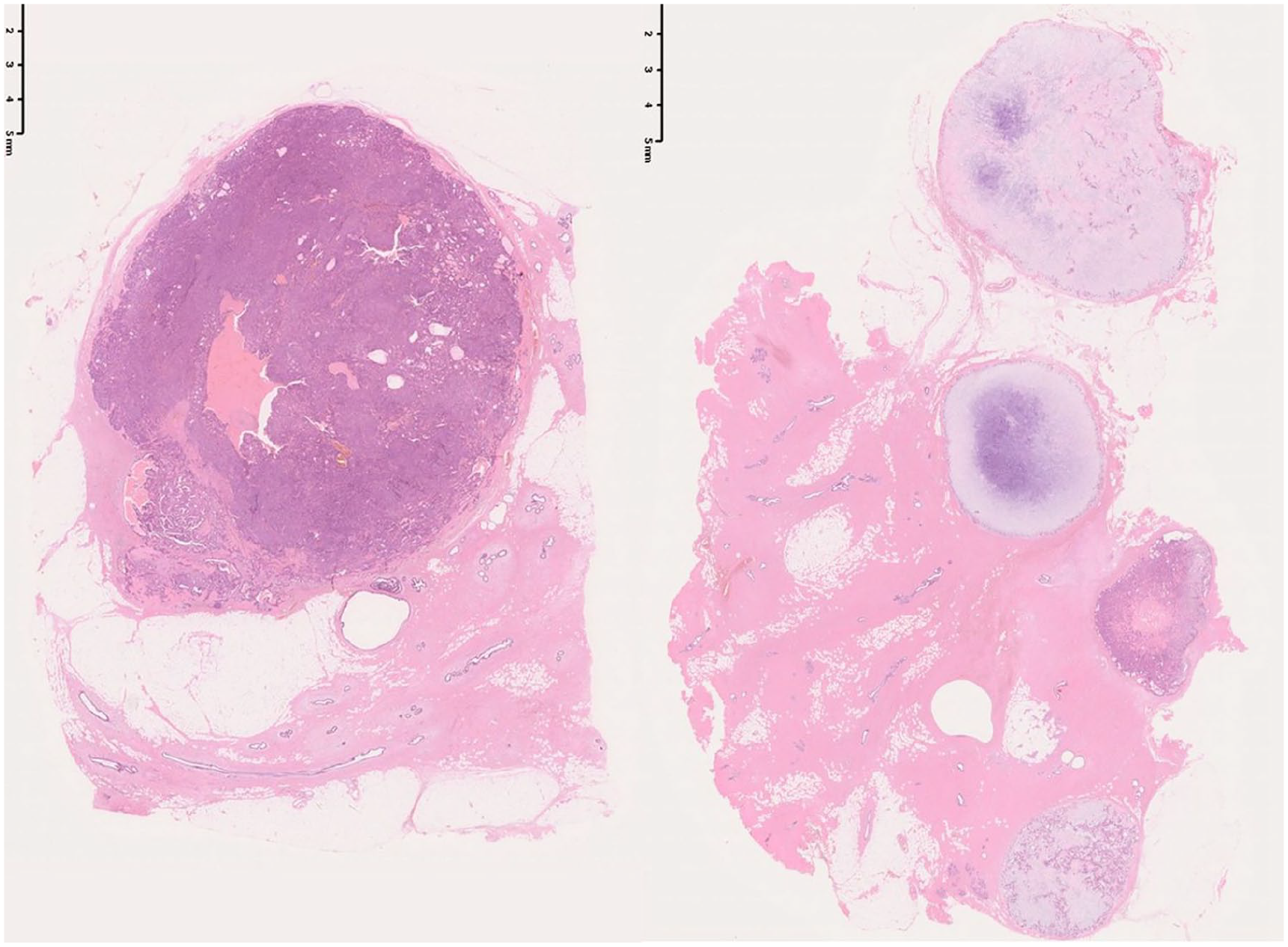
Pathological findings at low magnification. Left: adenomyoepithelioma component; right: pleomorphic adenoma component.
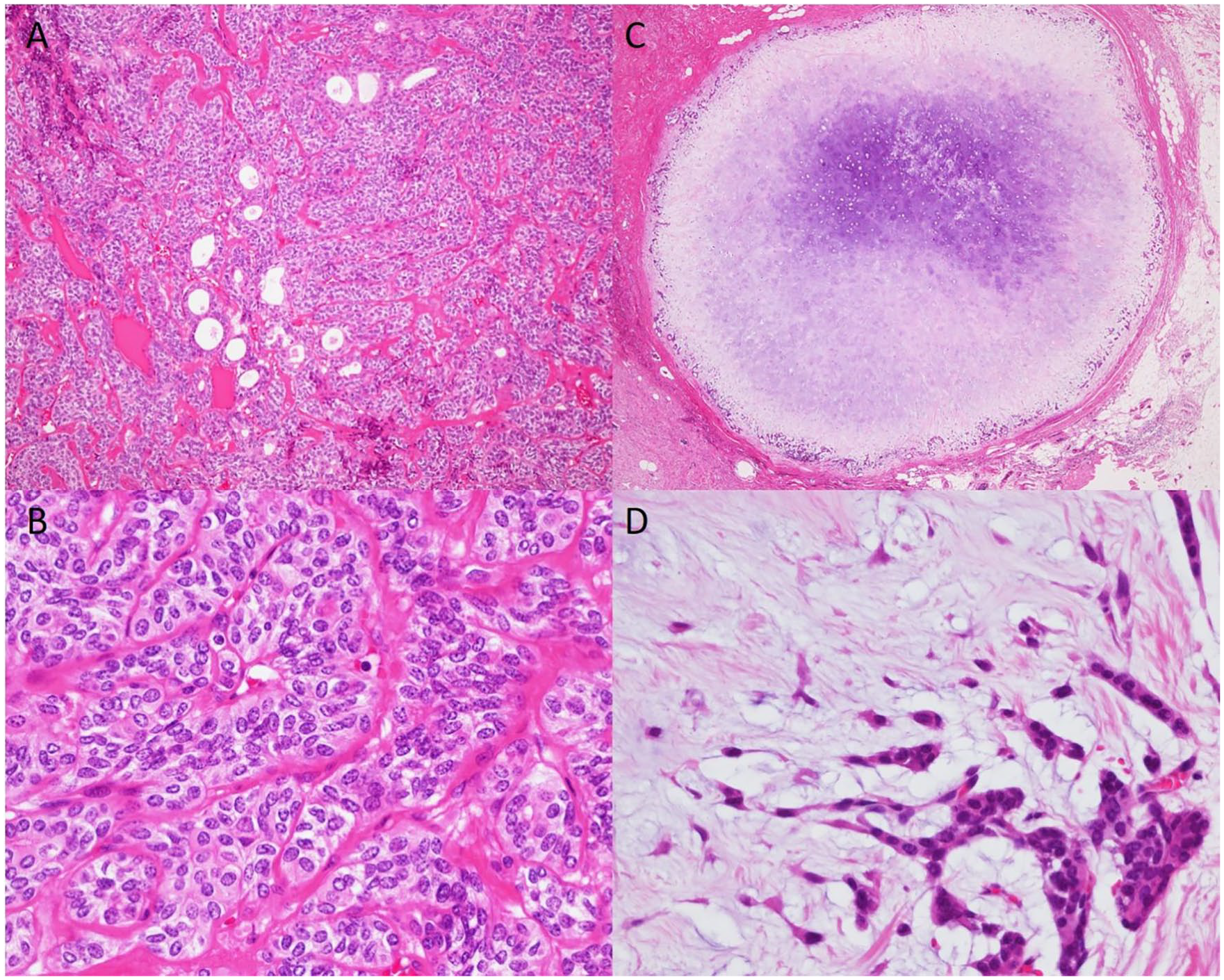
(A) Adenomyoepithelioma component. Biphasic proliferation of both luminal and prominent myoepithelial cells, which are composed of ductular and trabecular patterns. (B; high-power field of A) Myoepithelial cells have clear cytoplasm. Neither significant atypia nor increased mitoses are seen. (C) Pleomorphic adenoma component. The center of the nodules is occupied by myxochondroid stroma. (D; high-power field of C) Myoepithelial cells are spindle or stellate-shaped in myxochondroid stroma.
On immunohistochemistry, the myoepithelial cells were positive for S-100, smooth muscle actin (very focal), CK5/6 (partially), GFAP, and AE1/AE3, and negative for p63 and CD10. Luminal cells were positive for AE1/AE3, EMA, gross cystic disease fluid protein (GCDFP15), CK5/6, and ER (partially), and negative for PgR and HER2.
Discussion
Some authors have suggested that AME is associated with PA and intraductal papilloma.6,7 PA in the breast has the same histological features as in the salivary glands, with biphasic proliferation of glandular and myoepithelial cells, mingling with the myxoid stroma. 8 PA has only been reported in a few previous cases. 9 PA shares several histological features with other primary breast tumors, including matrix-producing metaplastic breast carcinoma or mucinous carcinoma, and some previous reports initially mistakenly diagnosed PA as these tumors on biopsy and fine needle aspiration.10,11
Immunohistochemical studies were performed to confirm biphasic proliferation of epithelial and myoepithelial cells. Though McLaren et al, who evaluated 35 cases of AME or closely related lesions, reported that p63 was consistently highly expressed in the myoepithelial cells of most sections, 12 in the current case, the myoepithelial cells were completely negative for p63. On the other hand, S-100 and GFAP were diffusely positive, and other myoepithelial markers were focally positive for myoepithelial cells. The possibility of failing to detect myoepithelial cells can be reduced by a panel-based approach including 2 or more markers. 13
The salivary gland counterpart, epithelial-myoepithelial carcinoma (EMCA), has been reported to harbor RAS and PIK3CA mutations, 14 downstream of the epidermal growth factor receptor family. 15 Urano et al investigated 87 cases of EMCA and showed that EMCA harbors a high frequency of HRAS mutations (82.7%). 16 Pleomorphic Adenoma Gene 1 (PLAG1) and High Mobility Group A2 (HMGA2) alterations have been identified exclusively in cases of EMCA ex PA, whereas HRAS mutations are predominantly represented in EMCA without PLAG1 and HMGA2 alterations. 17 Geyer et al subdivided breast AMEs depending on ER status and found that concurrent HRAS Q61 and PIK3CA or PIK3R1 mutations are frequently identified in the ER-negative group, and PIK3CA or AKT1 activating mutations are identified in the ER-positive group. 18 In an in vitro model, they found that induction of HRAS Q61R expression in breast epithelial cells resulted in proliferative activity and myoepithelial cell differentiation. 18 The coexistence of PA components and the expression of ER may be important factors in considering the pathogenesis of AME. The lack of molecular analysis is a limitation of this study. Information from future cases is needed to understand the molecular mechanism of mammary biphasic epithelial growth tumors including PA.
Extensive and diffuse myoepithelial proliferation was confirmed in the present case, which is characteristic of AME.12,13 On the other hand, we consider that the “PA-like component” described above is better diagnosed as PA than AME with cartilaginous metaplasia. No malignant features were seen in both components. The present case shows how tumors with biphasic epithelial growth in the breast present with diverse histological features, and these tumors should be carefully diagnosed when examining biopsy specimens and fine needle aspiration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.