
Abstract
Papillary carcinoma in the male breast is uncommon. Here, we report a case of a large encapsulated papillary carcinoma (EPC) in a 62-year-old male. The patient presented with a left breast mass of 1-year duration and bloody nipple discharge for several days. Mammography and breast ultrasonography showed a large left breast mass. The initial biopsy demonstrated fat necrosis with acute and chronic inflammation only. Due to clinical suspicion, a repeat biopsy was performed and revealed scant fragments of papillary carcinoma in a background of inflammation. The patient underwent left total mastectomy. Grossly, the breast contained a 9.0 cm entirely cystic lesion lined by a hemorrhagic thick fibrotic wall. No solid area was identified in the cyst. The entire cyst wall was examined under microscopy; only a few sections with papillary carcinoma were identified. The lesion was confined to the cyst wall; so, a diagnosis of EPC was made. Compared to the previously reported EPC cases of male breast, the lesion of this case was unusually cystic, which making the diagnosis challenging. Therefore, awareness of this unusual feature, repeat biopsy when the pathology result is discordant, and extensive sampling of the lesion are essential for making the correct diagnosis and guiding patient management.
Introduction
Male breast cancer is an uncommon disease with an incidence of ∼1% of all breast cancers and 0.17% of all male cancers. 1 The predominant histological subtype of invasive mammary carcinoma in males is infiltrating ductal carcinoma, which is diagnosed in more than 90% of all male breast tumors. 2 Papillary breast carcinoma is the second most common histological subtype and accounts for 4% of breast carcinomas in men. 3 Papillary carcinoma in males spans a wide spectrum that includes multiple types of invasive and noninvasive tumors. Papillary ductal carcinoma in situ is the most common subtype (75%).4,5 Encapsulated papillary carcinoma (EPC) only accounts for a small proportion of papillary carcinomas (12%). EPC is characterized morphologically by fine fibrovascular cores covered by neoplastic epithelial cells of low or intermediate nuclear grade and surrounded by a fibrous capsule. In the majority of cases, there is no myoepithelial cell layer within the papillae and at the periphery of the lesion. Due to its rarity, only a handful of cases and a relatively small case series of EPC in males have been reported in the literature.6-12 Here, we report a rare case of EPC, encountered as a large, entirely cystic lesion in a male breast, and discuss the diagnosis and management.
Case Report
A 62-year-old Hispanic male with no past medical history presented with a gradually enlarging left breast mass of 1-year duration with associated swelling, nipple retraction, erythema, and ulceration (Figure 1A). Computed tomography (CT) scan found an 8.6 × 7.3 × 2.6 cm thick-walled peripherally enhancing mass with calcification in the left anterior chest wall (Figure 1B). The differential diagnosis included abscess, hematoma, or malignancy. Mammography showed a 6.5 cm oval left breast mass with linear pleomorphic calcifications (Figure 1C). Breast ultrasonography (US) demonstrated an 8.0 × 5.0 cm irregular mass in the left breast with mixed echogenicity and septate with internal echoes (Figure 1D).
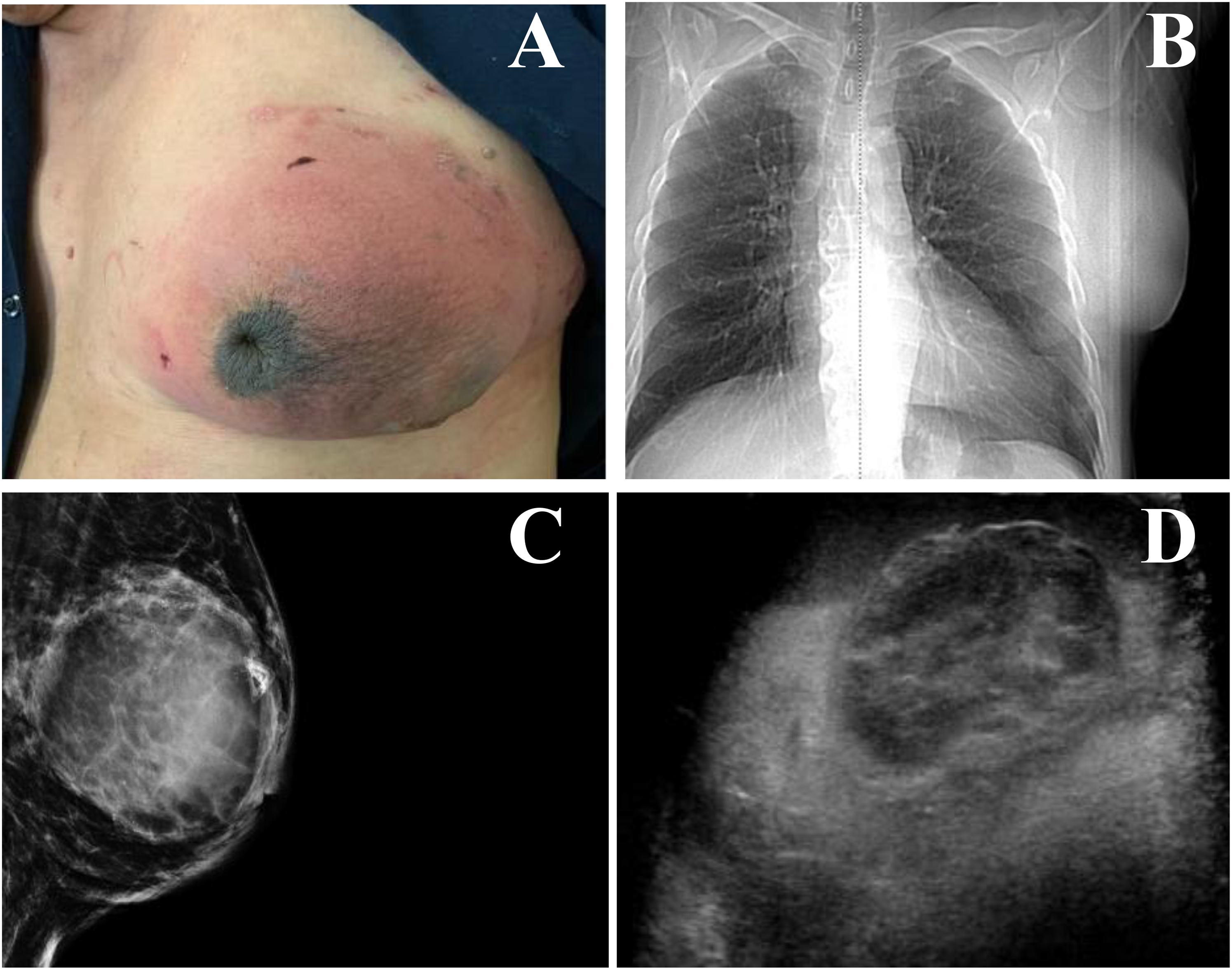
(A) Photograph of the left breast mass with swelling, nipple retraction, skin erythema, and ulceration. (B) Computed tomography (CT) image showing an 8.6 cm left chest wall mass. (C) Mammogram showing a 6.5 cm oval left breast mass with linear pleomorphic calcifications. (D) Ultrasound showing an 8 cm irregular left breast mass.
An US-guided core needle biopsy was performed for this left breast mass. The specimen contained fat necrosis with acute and chronic inflammation only. The case was discussed in the multidisciplinary tumor board. Due to clinical suspicion, a repeat biopsy was performed. Rebiopsy revealed scant fragments of papillary carcinoma in a background of inflammatory changes similar to that seen in the initial biopsy specimen (Figures 2A). The tumor cells were of low-to-intermediate nuclear grade. No definitive invasion was identified. Immunohistochemical (IHC) stains directed against p63 and smooth muscle myosin (SMM) heavy chain demonstrated lack of a myoepithelial cell layer both within the papillae and at the periphery of the lesion (Figure 2B). IHC stains directed against estrogen receptor (ER) and progesterone receptor both demonstrated strong nuclear reactivity in tumor cells (Figure 2C and D). Subsequently, the patient underwent left total mastectomy with axillary sentinel lymph node (SLN) biopsy. Grossly, the left breast had a 9.0 × 7.0 × 4.0 cm unilocular cystic lesion surrounded by a thick hemorrhagic wall and filled with serosanginous fluid (Figure 3A). No solid areas were identified in the cyst. The entire cyst wall was submitted for histological examination. Microscopically, the cyst was lined with a fibrotic wall composed of abundant foamy and hemosiderin-laden macrophages, cholesterol granulomas, and chronic inflammatory infiltrate (Figure 3B). Few (3 out of 38) submitted cyst wall sections contained an intracystic monotonous epithelial cell proliferation with a papillary configuration (Figure 3C). There was no frank invasion into the stroma or the surrounding benign breast parenchyma. IHC stains with p63 and SMM again demonstrated a lack of a myoepithelial cell layer both within the papillae and at the periphery of the papillary lesion (Figure 3D). The 4 SLNs were all negative for metastatic carcinoma. A diagnosis of EPC, an in situ carcinoma, was rendered.

(A) Papillary carcinoma shown by H&E (100 × ). (B) p63 stain showing lack of myoepithelial cell layer both within the papillae and at the peripheral of the papillary lesion (100 × ) SMM heavy chain with similar findings not shown. (C) Tumor cells strongly positive for ER (100 × ). (D) Tumor cells positive for PR (100 × ).
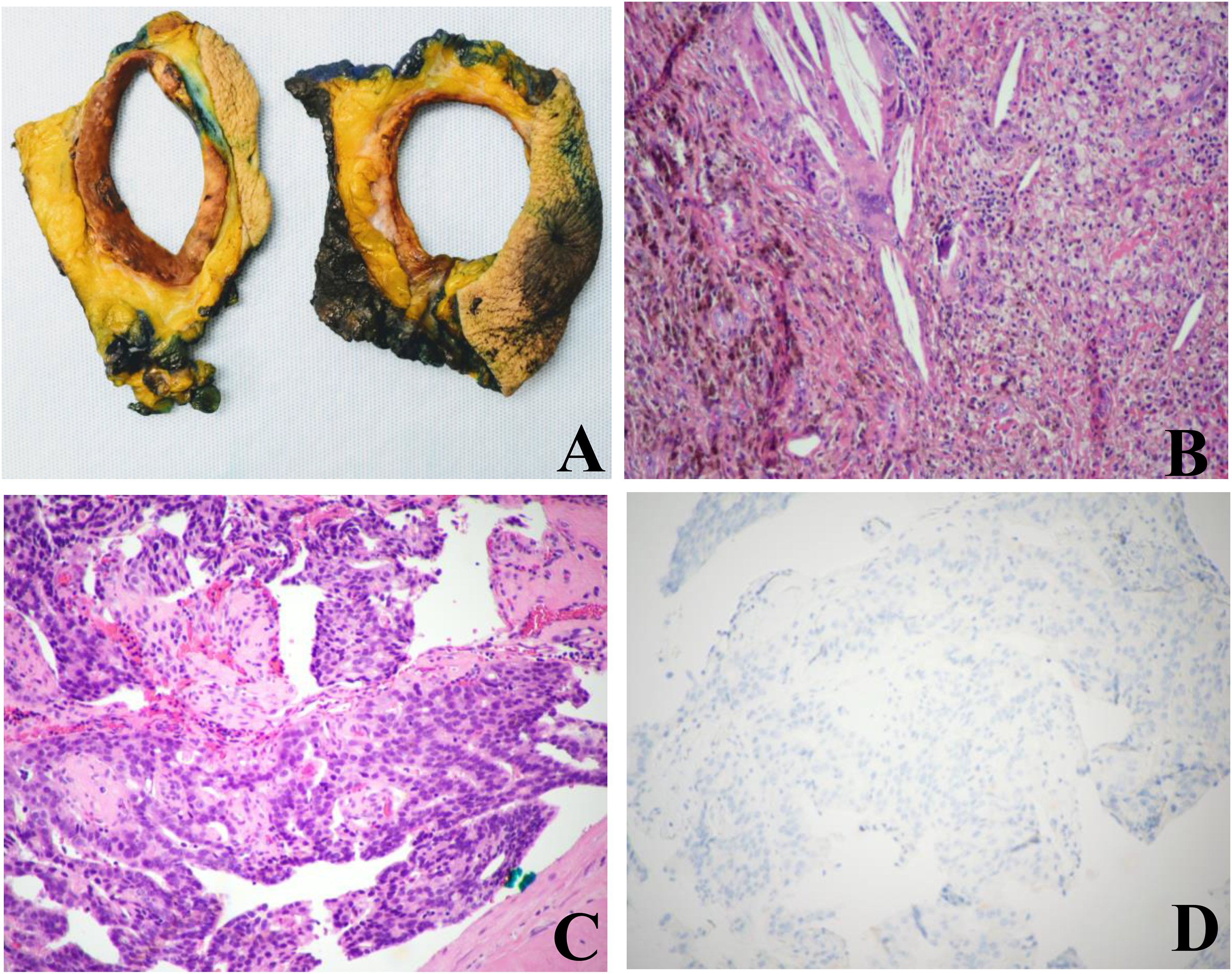
(A) Gross picture of the cystic mass (the photograph was taken after specimen fixation). (B) Hemorrhagic and fibrotic cystic wall with abundant foamy and hemosiderin-laden macrophages, cholesterol granulomas shown by H&E (100 × ). (C) Intracystic papillary carcinoma shown by H&E (100 × ). (D) p63 stain showing a lack of a myoepithelial cell layer both within the papillae and at the peripheral of the papillary lesion (100 × ) SMM heavy chain with similar findings not shown.
The patient was offered genetic counseling. His saliva sample was submitted for sequence analysis and deletion/duplication testing of 11 genes included in the Invitae Breast Cancer Guidelines-Based Panel (Invitae) to test for germline mutations. These genes include ATM serine/threonine kinase (ATM), breast cancer 1 gene (BRCA1), breast cancer 2 gene (BRCA2), cadherin 1 (CDH1), checkpoint kinase 2 (CHEK2), nibrin (NBN), neurofibromin 1 (NF1), partner and localizer of BRCA2 (PALB2), phosphatase and tensin homolog (PTEN), serine/threonine protein kinase 11 (STK11), and tumor protein p53 (TP53). No reportable genetic variants were identified. The patient did not receive radiation therapy or adjuvant endocrine therapy. As of 14 months post surgery, there was no evidence of recurrence or metastasis.
Discussion
EPC is a rare subtype of breast cancer and is usually diagnosed in the elderly. Grabowski et al 13 reported a median age of 69.5 years (range 27-99) in 917 cases. Male patients account for 3.5% of the total cases in their study. EPC originates as a solitary tumor in a cystic and dilated duct. Most reported male patients with EPC presented clinically with breast mass or swelling, with or without nipple discharge. The neoplastic cells are usually of low or intermediate grade, with no evidence of necrosis, and are strongly ER positive and human epidermal growth factor receptor 2/neu negative.6-12 EPC can be found in situ or associated with invasion.
Early and accurate diagnosis is essential for subsequent management and outcome evaluation for a patient with EPC. Clinical examination, radiological assessment, and histological examination are important to make the diagnosis prior to surgery. However, there are no specific clinical and imaging features that can distinguish EPC from other papillary lesions. 5 Fine-needle aspiration cytology and core biopsy are usually performed before performing surgery. However, the false negative results with fine-needle aspiration or biopsy are relatively frequent.11,13,14 In this mastectomy specimen, only 3 out of a total of 38 sections showed focal papillary carcinoma confined to the cyst wall. Therefore, excision is recommended in all cystic lesions in the male breast if the initial results are inconclusive and there is a high clinical suspicion for malignancy.
Due to the scarcity of EPC in males, there are no clear guidelines for management. Surgery, either breast-conserving surgery or mastectomy, is the mainstay of treatment. Axillary staging is recommended by most authors.13,15 There is no clear indication for radiation therapy and adjuvant endocrine therapy, even among patients with ER-positive tumors. In the absence of associated invasive carcinoma, EPC has a very favorable prognosis. The presence of associated ductal carcinoma in situ in the adjacent breast tissue confers a higher risk of local recurrence. 16
Similar to female breast cancer, genetic predisposition is an important risk factor in male breast cancer. It is necessary to increase genetic testing in male breast cancer in order to identify hereditary breast cancer and offer the pertinent preventive measures to patients and their families. Although multiple genes, especially BRCA2, have been reported to be involved in breast cancer predisposition in males, so far there is no report of hereditary genetic alterations associated with EPC.17,18 In this reported case, the patient underwent genetic testing to detect germline mutations. Although it is limited by only testing 11 genes, there are no reportable genetic variants identified in the commonly reported genes associated with hereditary breast cancer, including BRCA1, BRCA2, and PALB2. Somatic phosphatidylinositol 3-kinase, catalytic, alpha (PIK3CA) gene mutation has been reported to be the most common genetic alteration across the spectrum of papillary breast neoplasms, including EPC.19,20 However, the frequency of PI3KCA mutation seems to be lower in ER-positive male breast cancer.20,21 Further genomic studies are worth exploring this in detail.
In conclusion, EPC of the breast is a rare disease entity especially in males. We report a large entirely cystic EPC in the male breast. Therefore, cystic lesions in men should be worked up as potentially malignant lesions. Clinical examination, radiological findings, and histopathological evaluation provide valuable information for the optimal work-up and diagnosis for patients with this rare entity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.