
Abstract
Germ cell differentiation has been described in association with somatic tumors arising from several organ systems; rare cases arising from urothelium have been reported. Here we present a 62-year-old male with a remote history of lung cancer, a left adrenal gland mass, and a 5.6 cm left bladder wall mass; cystoscopy demonstrated a large papillary mass on the left anterior bladder wall. A transurethral resection specimen was sent for review in consultation and showed extensive papillary structures with thin fibrovascular cores lined by neoplastic cells with clear cytoplasm. These neoplastic cells were diffusely positive for pancytokeratin, CDX2 (caudal-type homebox 2), SALL4 (sal-like transcription factor 4), glypican-3, AFP (alpha-fetoprotein), while negative for PAX-8 (paired box gene 8), NKX3.1 (NK3 homeobox 1), PSA (prostate specific antigen), TTF-1 (thyroid transcription factor 1), Napsin A, inhibin, and OCT4 (octamer-binding transcription factor 4). Conventional urothelial conventional carcinoma and focal squamous differentiation were also identified as minor components. Urothelial carcinoma was focally positive for GATA3 (GATA-binding protein 3) and p63; SALL4 and glypican-3 were negative. Overall findings supported a yolk sac tumor with a smaller component of squamous cell carcinoma (<1%). Subsequent cystectomy showed similar morphologic features and immunoprofile in addition to foci of urothelial carcinoma and urothelial carcinoma in situ. No chromosome 12p abnormalities were identified by fluorescent in-situ hybridization study. A diagnosis of yolk sac tumor derived from urothelial carcinoma was made. Yolk sac tumor should be considered in the differential diagnosis of a high-grade urothelial carcinoma, particularly when glandular or other unusual architectural patterns are present. A somatic origin with underlying genomic instability similar to what has been described in the uterus and ovaries is suggested.
Keywords
Introduction
Germ cell differentiation has been described in association with somatic tumors arising from several different organ systems1-4; it is well established that urothelial carcinoma may show divergent differentiation, and several variants have been recognized by the 2016 World Health Organization (WHO) classification of urothelial carcinomas. 5 These include but are not limited to squamous, glandular, trophoblastic, neuroendocrine, nested, micropapillary, plasmacytoid, and sarcomatoid variants of urothelial carcinoma. Although currently not considered a histologic variant of urothelial carcinoma, yolk sac tumor (YST) differentiation in urothelial carcinoma has been previously reported. 3 Transformation of totipotent malignant cells and genomic instability of tumor cells are believed to be the mechanisms behind the development of nongermline differentiation like yolk sac cells in somatic malignancies.6,7 Herein, we describe a rare case of YST arising as a predominant component of bladder urothelial carcinoma with likely origin as differentiation of urothelial carcinoma. The purpose of this article is to provide awareness of this divergent differentiation and formulate a differential diagnosis when high-grade urothelial carcinomas showing unusual or glandular patterns are encountered. Recognition of variant histologic features in urothelial carcinoma is crucial as there may be therapeutic and prognostic implications.
Case Presentation
A 62-year-old Caucasian man presented with gross hematuria, which prompted him to seek medical attention. He had a prior history of low-grade well to moderately differentiated adenocarcinoma of the lung diagnosed in 2014, post-radiotherapy and under surveillance. A computed tomography scan showed a 5.6 cm left bladder wall mass. Cystoscopy demonstrated a large papillary mass involving the left anterior bladder wall. A transurethral resection specimen was sent for review in consultation and showed extensive papillary structures with thin fibrovascular cores lined by neoplastic cells with clear cytoplasm (Figure 1A and C). The neoplastic cells were diffusely positive for pancytokeratin, CDX2 (caudal-type homeobox 2), SALL4 (sal-like transcription factor 4) (Figure 1B), glypican-3 (Figure 1D), AFP (alpha-fetoprotein), with negative expression for PAX-8 (paired box gene 8), NKX3.1 (NK3 homeobox 1), PSA (prostate specific antigen), TTF-1 (thyroid transcription factor 1), Napsin A, inhibin, and OCT4 (octamer-binding transcription factor 4); the tumor was focally positive for expression of GATA3 (GATA-binding protein 3) and p63 with negative expression of SALL4 and glypican-3 in an area that carried the morphologic appearance of urothelial carcinoma component. Overall findings supported a YST with a small component of squamous cell carcinoma. A cystectomy was performed 3 months after the initial presentation. The mass was exophytic, ill-defined, pink-tan, and friable on gross examination, with estimated dimensions of 6 cm and extended into perivesical soft tissue. Histologic sections showed a tumor with a reticular appearance and a meshwork of irregular channels with diffuse papillary architecture. The elongated papillary structures contained central fibrovascular cores and were lined by tall columnar cells containing subnuclear vacuoles (Figure 2A). In addition, smaller components of urothelial carcinoma showing a micropapillary pattern (10%) (Figure 2B) and urothelial carcinoma in situ with squamous differentiation (5%) involving the prostatic urethra (Figure 2C) and bilateral ureters were also identified.

Microscopic features of YST of the bladder. (A) YST composed of a predominant papillary architecture. (C) High power view of YST showing tumor cells with clear to eosinophilic cytoplasm, distinct cytoplasmic membranes, and large vesicular nuclei, some with prominent nucleoli. Immunohistochemical stains showed the tumor cells to be immunoreactive for (B) SALL4 and (D) glypican-3.

Microscopic features of yolk sac tumor (YST) of the bladder. (A) Bladder tumor showing YST with a complex papillary growth pattern. (B) Deep invasive component of micropapillary showing tight nests of tumor cells in lacuna-like spaces. (C) Urothelial carcinoma in situ with squamous differentiation involving prostatic urethral epithelium, periurethral glands, and proximal prostatic ducts.
Immunohistochemical results are summarized in Table 1. Fluorescent in-situ hybridization (FISH) was performed and showed no alterations in chromosome 12p. A diagnosis of YST derived from urothelial carcinoma was established. Genetic alterations and tumor mutation burden were determined by next-generation sequencing and showed gene mutations in LACE1, CDK4, RB1, STAG2, TSC1, TP53, and MLH. NY-ESO-1 (New York esophageal squamous cell carcinoma 1) cancer-testis antigen was overexpressed. Tumor mutation burden was low, measuring 6.3 muts/mb, and the tumor was classified as microsatellite stable. Some of these gene mutations have been identified in other germ cell tumors, although not specific enough to distinguish.8,9 At present, the patient is being considered for adjuvant chemotherapy and remains free of disease 7 months after initial diagnosis.
Immunohistochemistry: Antibody Specifications.
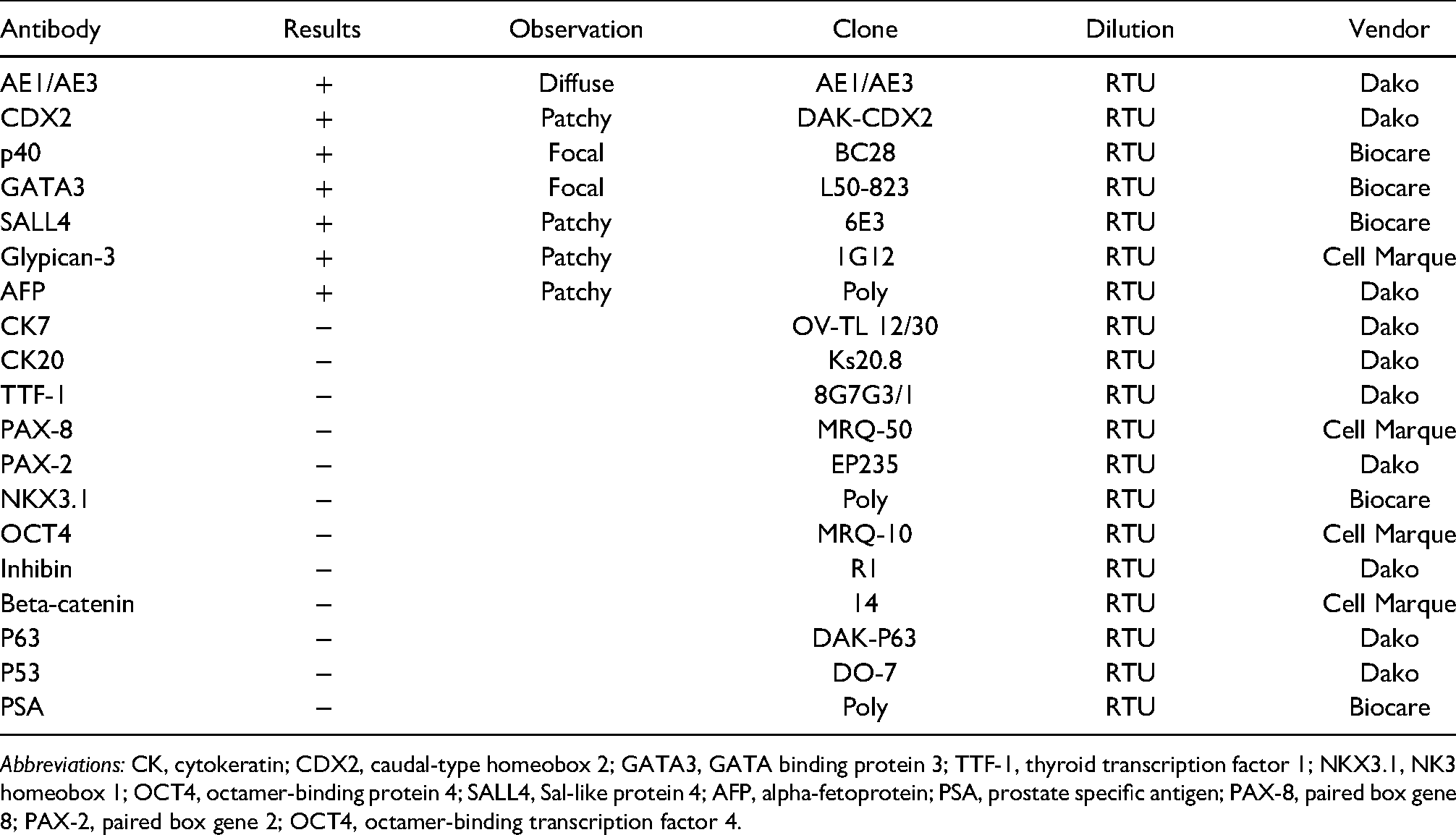
Abbreviations: CK, cytokeratin; CDX2, caudal-type homeobox 2; GATA3, GATA binding protein 3; TTF-1, thyroid transcription factor 1; NKX3.1, NK3 homeobox 1; OCT4, octamer-binding protein 4; SALL4, Sal-like protein 4; AFP, alpha-fetoprotein; PSA, prostate specific antigen; PAX-8, paired box gene 8; PAX-2, paired box gene 2; OCT4, octamer-binding transcription factor 4.
Discussion
YST differentiation may occur in a variety of anatomic sites, including the sinonasal region, stomach, colon and lung, and endometrium, especially in postmenopausal women, in benign and some malignant somatic lesions.7,10-12 Due to the rarity of this entity, the 2016 WHO classification has not yet included the YST differentiation as a histological variant of urothelial carcinoma. 5
In a case report, Samaratunga et al, 13 described a high-grade urothelial carcinoma with an extensive glandular component resembling hepatoid adenocarcinoma and AFP positivity. They suggested that AFP production precedes the genetic changes that give rise to hepatoid morphology. Hepatoid morphology is included in the spectrum of YST, and those tumors that are characterized as hepatoid may represent a somatic type YST differentiation. Immunohistochemical profile and molecular characterization of these tumors may shed light on the precise nature of these tumors. There are 9 previously reported cases of adenocarcinoma of the bladder in addition to 2 cases of urothelial carcinoma with AFP expression.14-21 There are 4 previous reports from the renal pelvis with elevated serum AFP, 3 with glandular differentiation, and 2 with an associated urothelial carcinoma.22-25 SALL4 positivity in urothelial carcinoma has also been described. 26 Among those cases, additional immunohistochemistry studies were not performed to confirm YST differentiation. Histologically, our case showed a range of morphologic features, including a classic microcystic pattern with intracellular lumens imparting a “sieve-like” arrangement and frequent intracellular and extracellular hyaline globules. Frond-like papillae or branched tubulopapillary structures lined by columnar cells with subnuclear vacuolation were also observed; the latter more frequently observed among somatic neoplasms with YST differentiation. 27 Immunohistochemistry plays an important role in diagnosing YST differentiation, which typically shows positive immunoreactivity for AFP, SALL4, while immunonegative for epithelial markers, especially cytokeratin 7 (CK7) and epithelial membrane antigen (EMA). 27 Markers of intestinal differentiation such as CDX2 and HepPar1 may be positive in areas with glandular and hepatic differentiation, respectively. Our case showed an immunohistochemical profile confirming the diagnosis of urothelial carcinoma with predominant divergent YST features in both the previous transurethral resection and cystectomy specimens. No chromosome 12p abnormalities were identified by FISH study. In malignant germ cell tumors and tumors with somatic malignant transformation, isochromosome 12p (i(12p)) is the most common alteration followed by 12p overexpression. 28 Thomas et al 29 reported i(12p) and other alterations of chromosome 12 in support of malignant transformation, while other investigators favored a YST of somatic origin in the absence of a chromosome i(12p).10,30 Acosta et al 7 reported all cases of mixed Mullerian and germ cell or trophoblastic tumors containing YST and trophoblastic component were negative for i(12p) by FISH study; however, revealed copy-number variants by next-generation sequencing, findings suggesting that the presence of YST or trophoblastic tumor component may indicate an underlying genomic instability. Additionally, a recent study found that 12p overrepresentation, including i(12p), in other tumors apart from germ cell neoplasms. 31 McNamee et al, 27 have proposed these tumors may arise from a process referred to as neometaplasia or retrodifferentiation or transformation of totipotent malignant cells and genomic instability.
Our patient presented at a slightly younger age than the average age reported by other investigators (63 years vs 73 years). 13 This is in contrast to primary extragonadal YSTs, which typically present in young adults, 32 although few cases have been described in elderly patients.33-36 Increased serum AFP levels may be noted in patients with tumors containing YST elements. AFP levels were unknown in our case; however, are not routinely measured in patients with bladder carcinoma. Serum AFP determinations should be considered in the postoperative settings for early detection of metastases or the presence of recurrent disease. 37
Because of the limited number of reported cases, there is no consensus on standard treatment. In the prior case reported by Espejo-Herrera and Condom-Mundó, 3 the patient presented with thoracic mass at presentation, after surgery received chemotherapy cycles with poor response, and developed pulmonary and brain metastasis 9 months following cystectomy. The patient died 11 months after diagnosis. In the present case, the patient remains alive and disease-free 7 months after surgery. Follow-up imaging studies have yet to be performed. Consideration for adjuvant therapy, including platinum-based chemotherapy or adjuvant nivolumab, is being considered and largely dependent on the patient's performance status.
The differential diagnosis includes metastasis or secondary extension from adjacent organs to the bladder, and carcinoma arising within the urothelium displaying enteroblastic differentiation. Given the presence of urothelial carcinoma with areas of glandular differentiation, the diagnoses of metastatic YST and primary extragonadal YST were considered less likely. Carcinoma with enteroblastic differentiation has been primarily reported in the gastrointestinal tract, while hepatoid differentiation most commonly has been found in the stomach but may occur in a variety of other organs, including the gastrointestinal tract, ovary, and bladder.13,38 These tumors show similar histopathological and immunohistochemical features as those identified in our case. This phenomenon could also be regarded as a form of neometaplasia, aberrant differentiation, or retrodifferentiation or considered part of the same spectrum of what some authors have termed “somatically derived YST.” 27 Differential diagnoses with morphologic and immunohistochemical profiles are summarized in Table 2.
Immunohistochemical Markers for Distinguishing YST From and Other Malignancies.
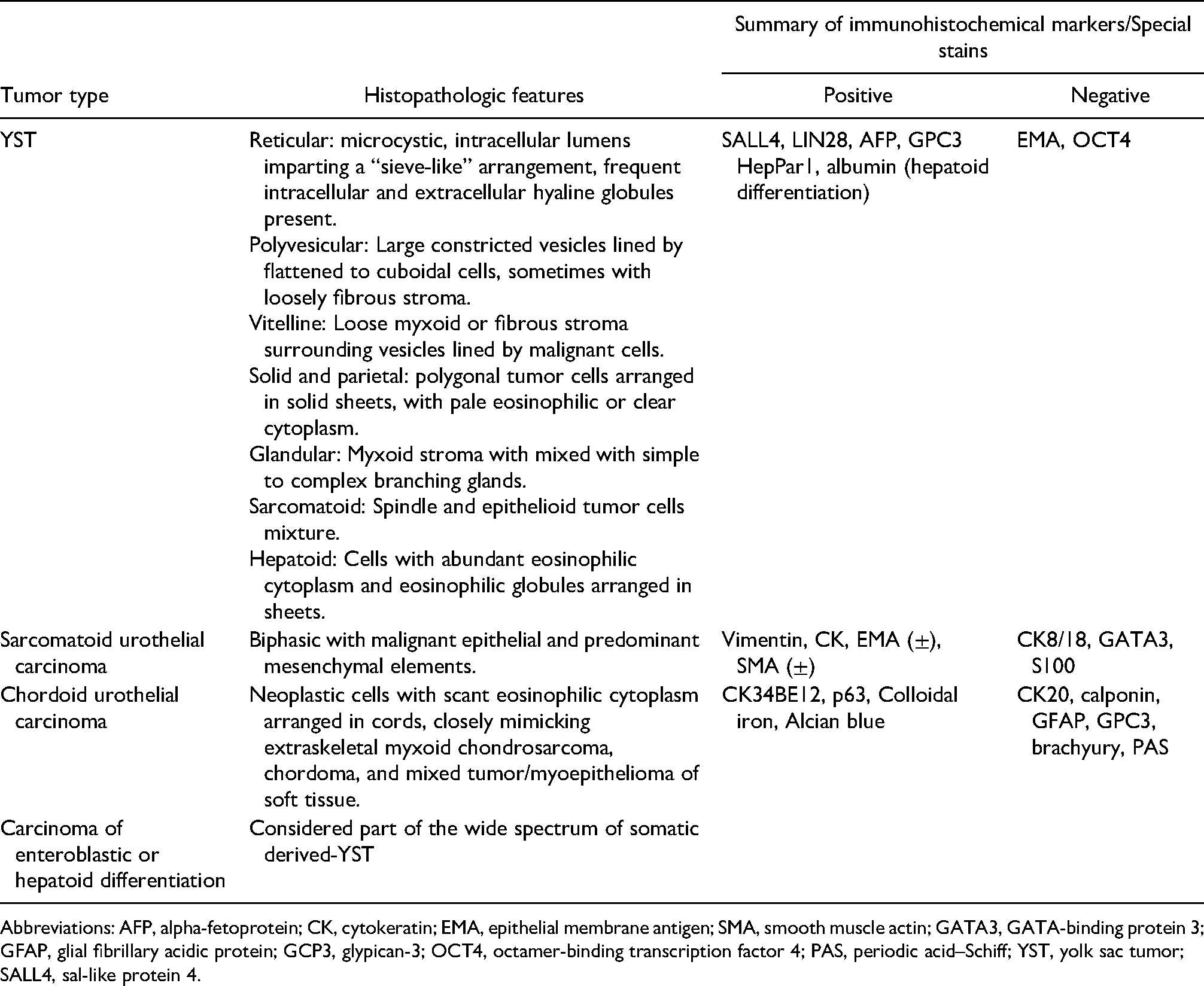
Abbreviations: AFP, alpha-fetoprotein; CK, cytokeratin; EMA, epithelial membrane antigen; SMA, smooth muscle actin; GATA3, GATA-binding protein 3; GFAP, glial fibrillary acidic protein; GCP3, glypican-3; OCT4, octamer-binding transcription factor 4; PAS, periodic acid–Schiff; YST, yolk sac tumor; SALL4, sal-like protein 4.
Conclusion
In summary, this is an exceptionally rare case of urothelial carcinoma with predominant YST differentiation and represents a rare example of a somatically derived germ cell tumor. YST differentiation should be considered in adult patients with urothelial tumors showing glandular and hepatoid histological patterns. It is hypothesized that the occurrence of germ cell type malignancy can arise within a somatic neoplasm by neometaplasia or retrodifferentiation or transformation of totipotent malignant cells coupled with genomic instability of tumor cells. Immunohistochemistry is necessary to confirm the diagnosis and exclude other differentials. Other confirmatory tests, including FISH studies for chromosome 12p abnormalities may be helpful.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.