
Abstract
Background. Synovial sarcoma (SS) is a rare soft tissue sarcoma. Available data regarding survival outcomes of patients with SS still remains limited. In this study, a single center retrospective analysis was performed to investigate the clinical characteristics, pathology and survival outcomes in patients with SS in China. Methods. Patient data were systematically reviewed at the National Cancer Center from January 2015 to December 2020. The general information and treatment condition of patients were collected. Overall survival (OS) was evaluated using the Kaplan-Meier and Cox regression method. Results. A total of 237 consecutive patients were included in this study (follow-up cut-off date: December, 2020). The median age of patients involved was 35 years (ranging from 5 to 83 years) and the mean tumor diameter was 5.3 cm (ranging from .2 to 26.0 cm). The main findings of the immunohistochemical staining analyses were EMA (111/156) (71%), keratin 7 (32/64) (50.0%), keratin 8/18 (12/20) (60%), keratin 19 (42/70) (60%), S-100 (18/160) (11%), BCL2 (128/134) (96%), CD99 (137/148) (93%) and TLE1 (23/26) (88%). It was found that 109 patients (66%) were presented with monophasic subtype and 55 (34%) with biphasic subtype. A total of 137 patients were tested by FISH method and 119 patients (87%) demonstrated SS18 rearrangement, whereas 18 patients (13%) did not show SS18 rearrangement. Generally, it was found that the 3-year OS rate was 86% and the 3-year DFS was 55%. Results of univariate analysis revealed that age, tumor size, tumor site, radiotherapy and targeted therapy were significantly correlated with the overall survival (P < .05). Further, multivariate Cox regression analysis revealed that age, tumor size and radiotherapy were significantly associated with OS (P < .05). Conclusions. In conclusion, this study shows that the outcomes of patients with SS significantly decrease with age and tumor size. It was evident that radiotherapy is an independent and positive prognostic factor for patients with SS. In addition, it was shown that the prognosis of SS varies with tumor location. For instance, primary tumors in lower extremities have a higher prognosis, whereas tumors located in thorax have a lower prognosis.
Introduction
Synovial sarcoma (SS) is a clinically malignant soft tissue sarcoma, representing between 8% and 10% of all soft tissue sarcomas. It has an estimated incidence of 2.75 per 100 000 general population.1,2 Despite its name, this rare subtype of mesenchymal neoplasm has no direct relationship with synovium. It may originate from any part of the body, generally near the joint regions of the extremities with a predilection of the lower limb.3,4 Synovial sarcoma can also occur at other body locations, such as the lung, kidney and heart. It usually affects adolescents and young adults. The median age of SS diagnosis is typically 35 years, though the ages can range from 5 to 85 years. 5
Generally, SS is divided histologically into three subtypes: monophasic, biphasic and poorly differentiated. More than 90% of SS are characterized by a well-established chromosomal translocation t(X; 18) (p11.2, q11.2). This involves the SS18 gene (formerly SYT gene) on chromosome 18 and one of the several synovial sarcoma X genes (SSX gene) on chromosome X (commonly SSX1, SSX2 or SSX4). 6 It hence results in a classical formation of SS18-SSX fusion oncogene. Fluorescence in-situ hybridization (FISH) or reverse transcription polymerase chain reaction (RT-PCR) methods are used to test the chromosome anomaly which causes SS. Currently, the standardized treatment of SS includes surgery and radiotherapy, with SS showing some sensitivity to routine chemotherapeutic agents like adriamycin and ifosfamide (AI chemotherapy regimen). Further, SS is generally considered a high-grade tumor with poor prognosis.
Previous studies have described the biological and clinical features of SS. However, clinical and pathological data as well as information on survival outcomes of patients with SS in China still remains limited. Therefore, the current study performed a single center retrospective study from the Chinese National Cancer Center to investigate the clinicopathological characteristics and survival outcomes of SS to guide future management of the disease.
Patients and Methods
Patient Identification and Data Abstraction
Patients with SS were recruited from the National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences, and Peking Union Medical College, including consultation patients from outside the hospital, between January 2015 and December 2020. The inclusion criteria of this study were: (1) pathologically confirmed patients with SS using the World Health Organization (WHO) classification system; (2) patients without synchronous primary tumors. To avoid the diagnosis deviation, the clinicopathological characteristics of the patients were independently determined by two experienced pathologists (Susheng Shi and Hongtu Zhang). A total of 237 patients met the criteria and were hence included in this study. Demographic and clinical data were collected for each patient. These data included gender, age, tumor size, tumor site, histologic subtype, immunohistochemical stains, molecular results and treatment condition. The influence of each predictive factor on survival outcomes was analyzed. Follow-up data were obtained by reviewing the records in the outpatient, letters to the patients or through telephone calls.
Immunohistochemistry
For immunohistochemistry staining, 3-μm-thick sections were mounted on the poly-L-lysine-coated slides, deparaffinized and hydrated through the graded alcohols to water. After endogenous peroxidase activity inhibition, performed by dipping sections in 3% hydrogen peroxide for 10 min. Immunohistochemical tests were performed for EMA (E29; IR62961; Dako; Denmark), keratin 7 (OV-TL12/30; ZM0071; Zhongshan; China), keratin 8/18 (DC10; ZM-0073; Zhongshan; China), keratin 19 (A53-B/A2.26; ZM0074; Zhongshan; China), S-100 (Z031129; Dako; Denmark), BCL2 (124; IR61461; Dako; Denmark) and CD99 (O13; MAB-0059; Maixin, China).
Fluorescence In Situ Hybridization
The Vysis SS18, Break Apart Rearrangement Probe consists of a mixture of 2 FISH DNA probes. The first probe, an 650 kb probe extends distally from the SS18 gene. The second probe lies 3’ or proximal to the SS18 gene and is 1044 kb in length. The cut-off level for an aberrant SS18 FISH was ≥15% of cells with a break-apart signal. An SS18 FISH split signal rate of <15% was interpreted as negative.
Ethical Approval
The present study was approved by the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences, Beijing, China (approval number 21/136-2807). Further, this study was conducted in accordance with the Declaration of Helsinki. The information involved in this study was retrospectively collected from the National Cancer Center electronic recording system and did not contain any personal information or privacy. Therefore, the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences determined that the patients consent to review their medical records was not required. Furthermore, all the data from the patients were anonymized or maintained with confidentiality.
Statistical analysis
Overall survival (OS) was calculated from the time of SS diagnosis to the time of death from any cause. Disease-free survival (DFS) was defined as the interval from diagnosis to recurrence or metastasis. Statistical package for the social sciences (SPSS) version 21.0 software (IBM, Armonk, NY, USA) was used for data analysis in this study. Statistics continuous variables were expressed as means ± SD or medians and range. However, categorical variables were expressed as proportions with percentages. Univariate survival analysis was performed using Kaplan–Meier curves and log-rank test. On the other hand, multivariate survival analysis was performed using the Cox proportional hazards regression model. All tests were two-sided, and statistically significant difference was set at a P < .05.
Results
Patient demographics and clinical characteristics
The demographical and clinical characteristics of all patients were summarized as presented in Table 1. A total of 237 patients were enrolled in this study which included 116 males (49%) and 121 females (51%). The median age was 35 years, ranging between 5 and 83 years. Thirty patients involved in this study (13%) were less than 18 years of age, 86 patients (36%) were between 18 and 34 years, 112 patients (47%) were between 35 and 64 years and nine patients (4%) were over 65 years. The mean tumor diameter was 5.3 cm (ranging from .2 to 26.0 cm). However, the tumor diameter was less than 5.0 cm in 132 patients (57%), between 5.0 and 10.0 cm in 77 patients (33%) and more than 10.0 cm in 24 patients (10%). Nevertheless, data on tumor size for four patients were not available.
Patient Characteristics.
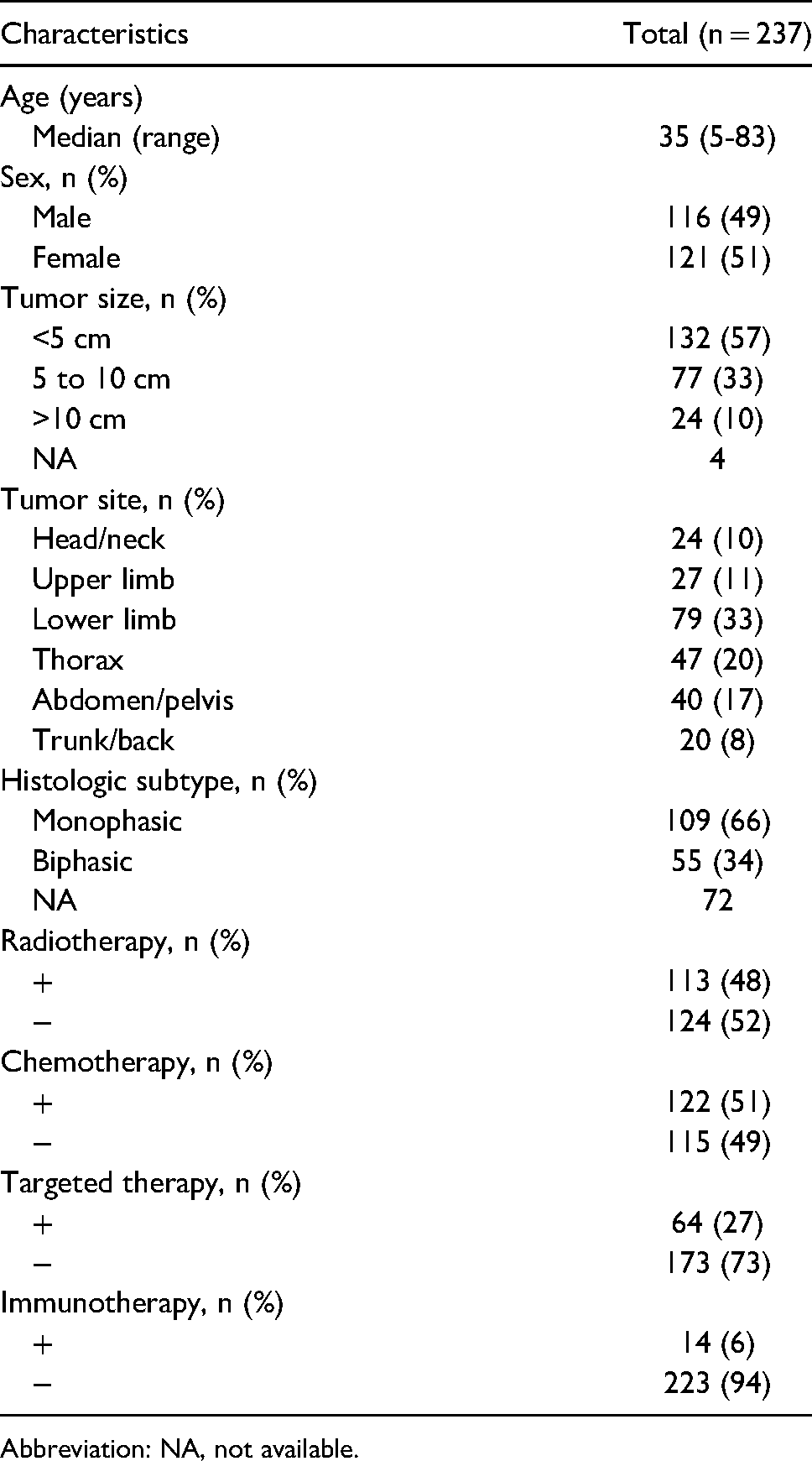
Abbreviation: NA, not available.
The main findings of the immunohistochemical staining analyses were EMA (111/156) (71%), keratin 7 (32/64) (50%), keratin 8/18 (12/20) (60%), keratin 19 (42/70) (60%), S-100 (18/160) (11%), BCL2 (128/134) (96%), CD99 (137/148) (93%) and TLE1 (23/26) (88%). Out of 164 patients, 109 of them (66%) were presented with monophasic subtype and 55 (34%) with biphasic subtype (Figures 1 and 2). It was noted that 73 patients had incomplete information about histological subtype. Further, patients with tumors in head/neck were 24 (10%), 27 patients (11%) had tumors in the upper limb (12 on the left and 15 on the right), 79 patients (33%) in the lower limb (36 on the left and 43 on the right), 47 patients (20%) in thorax (22 in lung, 6 in mediastinum, 3 in pleura and 3 in pericardium), 40 patients (17%) in abdomen/pelvis and 20 patients (8%) in trunk/back. A total of 137 patients were tested through FISH method and it was found that 119 patients (87%) demonstrated SS18 rearrangement, whereas 18 patients (13%) did not. And no patients tested with RT-PCR method.

Hematoxylin and eosin–stained (HE) and immunohistochemical stain (IHC) showing monophasic subtype SS (A) HE × 100. (B) HE × 200. (C) EMA × 200. (D) keratin × 200. (E) BCL2 × 200. (F) CD99 × 200.

HE and IHC showing biphasic subtype SS (A) HE × 100. (B) HE × 200. (C) EMA × 200. (D) keratin × 200. (E) BCL2 × 200. (F) CD99 × 200.
The patients who received chemotherapy were 122 (51%), out of whom 71 patients used AI chemotherapy regimen, 7 patients used MAID chemotherapeutic regimen (mesna + adriamycin + ifosfamide + dacarbazine) and 115 patients (49%) did not use chemotherapy. However, the exact chemotherapy regimens of 44 patients were not provided. The patients treated with immunotherapy (camrelizumab) were 14 (6%), whereas 113 patients (48%) received radiotherapy. A total of 64 patients (27%) were previously treated with tyrosine kinase inhibitors (TKIs), which included anlotinib alone in 32 patients, apatinib alone in 12 patients, pazopanib alone in 2 patients and multiple TKIs in 16 patients.
Survival Analysis
The median follow-up time was 35.0 months (from 1 to 348 months). As of December 2020, follow-up data were available for all 237 patients (100.0%). Among the studied patients, 169 of them (71.3%) were alive and 75 (31.6%) had local recurrence or distant metastasis. It was found that a total of 68 patients (28.7%) died during the study period. Of these, one patient died of lung squamous cell carcinoma, one died of intracerebral bleeding and one of car accident. The overall 3-year OS rate was found to be 85.7%, whereas the median survival for all patients was 185.0 months (95% CI, 97.7 to 272.3 months) (Figure 3).
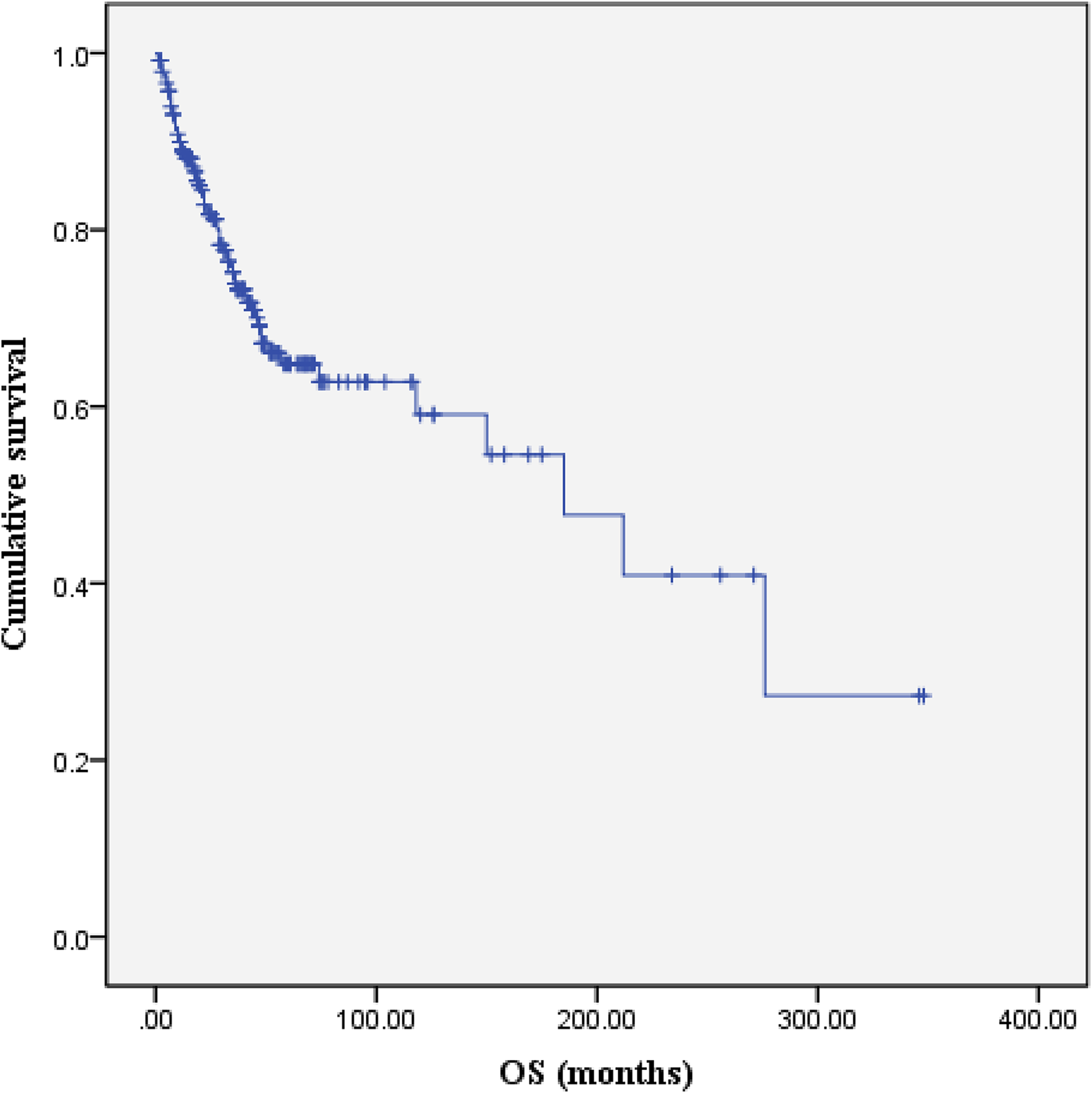
Kaplan-Meier overall survival (OS) curve of 237 SS patients.
Univariate analysis showed that age, tumor size, tumor site, radiotherapy and targeted therapy were significantly correlated with overall survival (P < .05; Figures 4 and 5). However, univariate analysis identified that sex, histologic subtype, immunohistochemical stains, molecular results, chemotherapy and immunotherapy were not significantly associated with survival (P > .05).
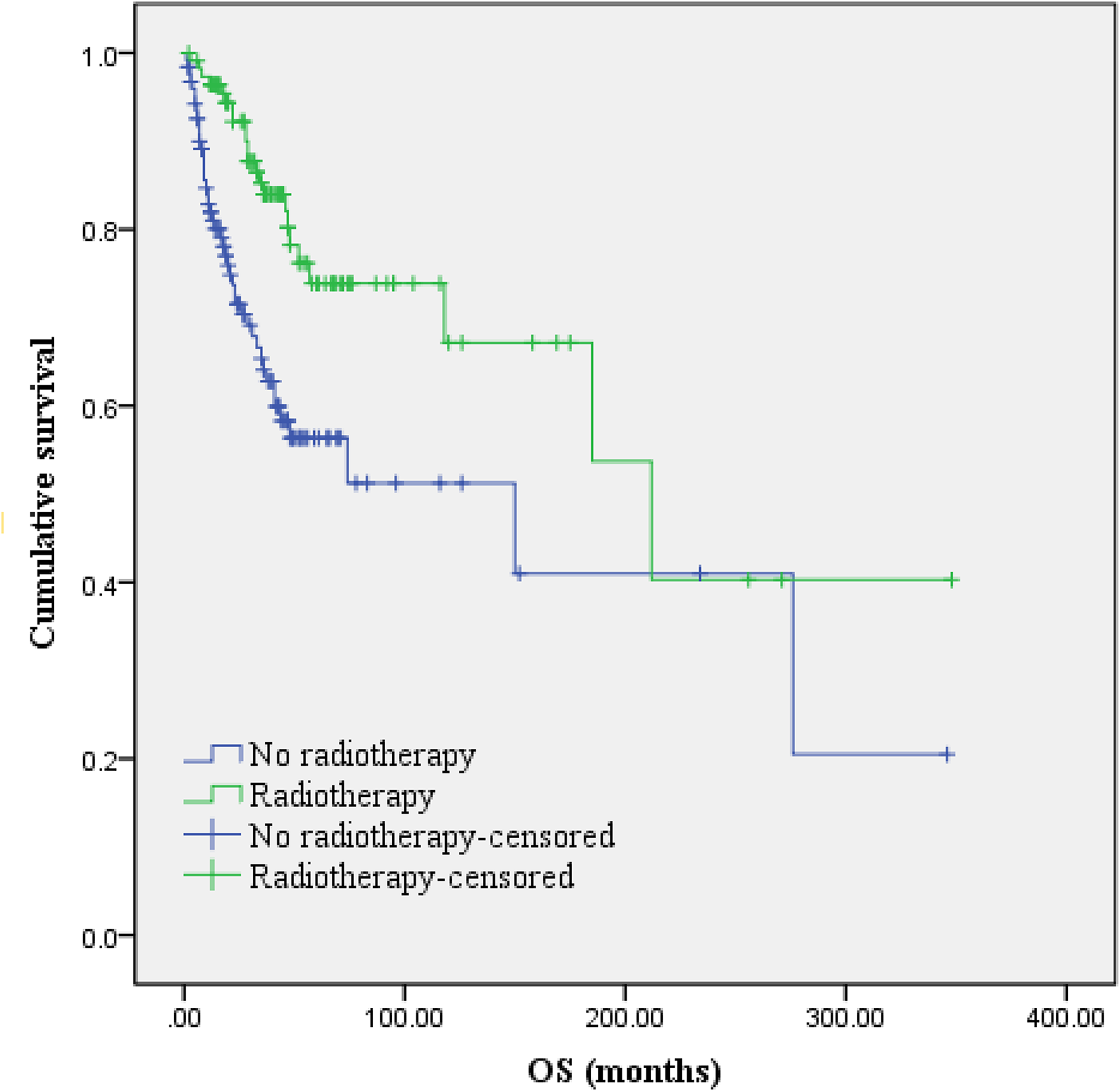
The Kaplan–Meier curve of overall survival for radiotherapy.
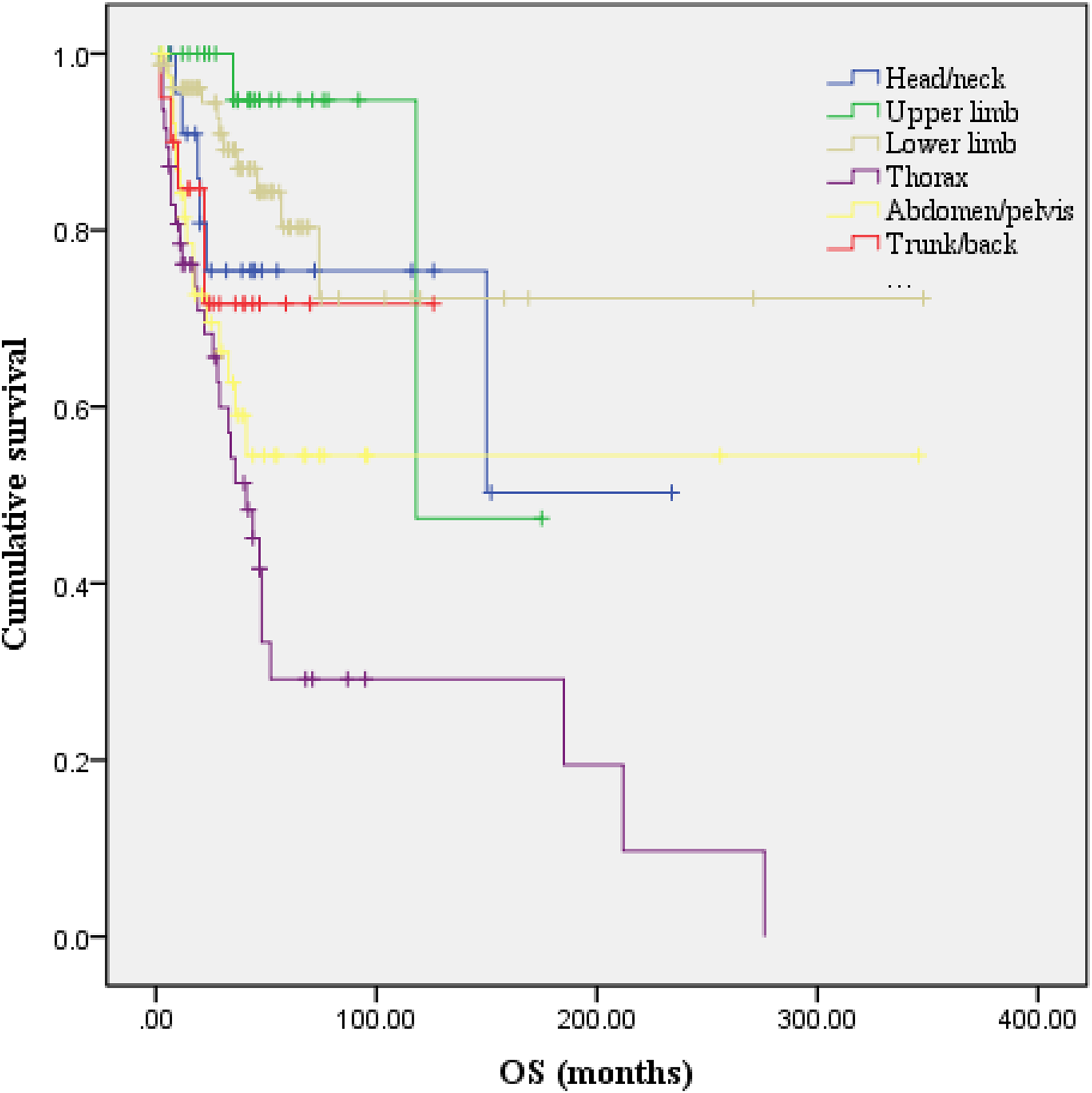
The Kaplan–Meier curve of overall survival for tumor site.
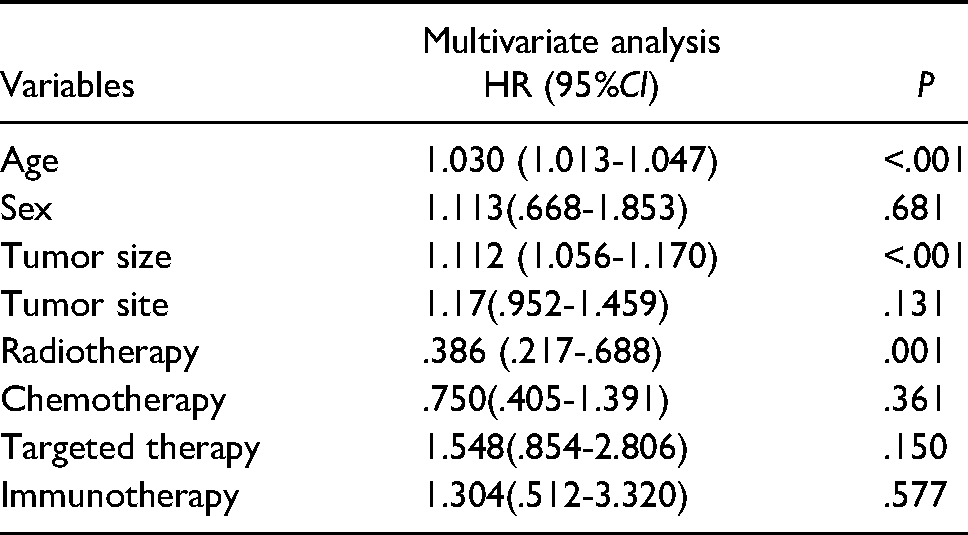
Multivariate Cox regression analysis revealed that age, tumor size and radiotherapy were significantly associated with OS (P < .05) (Table 2). Furthermore, it was noted that the survival group patients were younger than death group patients with a median age of 33.0 years and 42.5 years, respectively. Therefore, it was evident that prognosis decreased with increase in age of patients. The mean and median tumor size were 4.5 cm and 4.0 cm in the survival group, 7.3 cm and 5.4 cm in the death group, respectively. It was hence evident that larger tumor size was correlated with poor prognostic outcomes in patients with SS.
Multivariate Analysis of the Overall Survival of Patients.
Discussion
In this observational study, clinical characteristics and outcome of 237 patients with SS in China was reported. Synovial sarcoma is a highly aggressive disease with a dismal long-term prognosis. It has been reported that the 5-year and 10-year survival rates of patients with SS are approximately 60% and 50%, respectively. 7 In the present study, a 3-year overall survival of 85.7% was observed and there is likely survivor bias as most of the survivors with severe outcomes may have died.
Synovial sarcoma is characterized by a relatively high rate of local recurrence and distant metastasis. It has been shown that lung is the most common site of metastasis, followed by bone and lymph nodes. Previous studies have reported that approximately 50% of patients with SS will develop metastases, which is more common in adults.8,9 In the current study, it was found that 75 patients (31.6%) had local recurrence or distant metastasis. 3-year DFS of patients with SS was 55%. Further, 7 patients (9.3%) were less than 18 years and 68 patients (90.7%) were over 18 years. Local recurrence or distant metastasis occurred within 3 year in 53 cases (70.7%). The longest local recurrence or distant metastasis time in patients with SS was 268 months. Therefore, periodic reexamination was required to prevent local recurrence or distant metastasis, especially within 3 years after surgery.
Age is a known prognostic factor for the outcomes in patients with SS. Brennan et al reported that patients aged from 1 to 19 years have the best prognosis, whereas those over 70 years have a high mortality rates. 10 Elsewhere, in a comparative study between SS in children and adults, Sultan et al revealed that adult patients with SS have a worse prognosis. 11 Vlenterie et al reported that the outcomes of patients with SS significantly decrease with age, regardless of tumor size, primary tumor size and treatment. 12 In a separate study, Aytekin et al divided the SS patients into two groups (patients ≥35 years and patients <35 years) and it was noted that patients ≥35 years were associated with a less prognosis that patients <35 years. 13 In the current study, the univariate and multivariate Cox regression analysis revealed that age was significantly associated with OS (P < .05). This result showed that the older patient was, the worse the patient outcome would be, which was consistent with the previous reports in literature.
Previous studies have reported that male sex is associated with poor prognosis in patients with SS. 13 Further, several studies have shown that increase in size of tumor is significantly associated with low survival and this has consistently emerged as an important predictive factor of poor prognosis across studies.14–16 The present study found no correlation between sex and prognosis (P = .159). This is probably because of the small sample size used in this study. However, the univariate and multivariate analysis revealed that tumor size was an independent predictive factor of patients with SS (P < .001); larger tumor size was correlated with worse outcome.
Previously, it has been shown that SS18 gene break-apart probe is a reliable diagnostic tool to identify SYT disruption in SS disease. The Vysis LSI SS18 (18q11.2) Dual Color, Break Apart Rearrangement Probe identified 86% of positive cases in a study using 134 paraffin-embedded tumors, in which SS was the favored diagnosis. In the present research, a total of 137 patients were tested through FISH method and 119 patients (86.9%) demonstrated SS18 rearrangement. This was in consistence with the findings of other previously reported research studies. In addition, it is worth mentioning that the results of FISH are affected by variable pre-analytical handing of the specimen, including delay in fixation, inappropriate fixation time, inappropriate fixation solution and issues regarding paraffin embedding. Among the 137 patients tested by FISH method, 93 were consultation cases from other hospital. The specimen processing differences and storage conditions deserve further consideration.
Synovial sarcoma often arises in the extremities, particularly the lower extremities, usually in the middle or proximal portions (commonly around the knee) but can also occur in different body parts. 17 The second most common location is reported as the head and neck area. 18 The present study showed that the lower limb is the most frequent place of SS (33.3%), which was in agreement with other previous studies. However, in this study, thorax was the second most common site for SS (19.8%). This might be that our department of thoracic surgery is one of the largest and top ranked departments in China, with a naturally high proportion of patients with thoracic SS. It is reported that SS located in other areas are associated with a worse prognosis than SS located in body extremities. 11 Previous studies have also reported that distal rather than proximal site in the extremities reveals a more favorable outcome in patients with SS. This might be attributed to location on a distal extremity region allowing for earlier diagnosis of SS at a smaller tumor size and subsequent initiation of earlier treatment under more favorable conditions. In the present study, a univariate analysis demonstrated that tumor site was also associated with prognosis (P < .001). It was found that the primary tumors originating from lower extremities have a better prognosis, while the tumors originating from thorax have a poor prognosis. The results may be ascribed to the following reasons. First, thoracic tumors cannot removed easily by surgery compared with the primary tumor located in other body parts, due to its unusual site with a narrow space. Second, thoracic tumors are adjacent to vital structures and its thoracic involvement can cause respiratory failure and is associated with poor prognosis.
Management of SS involves multiple-modality therapy with surgery, radiotherapy, chemotherapy and targeted therapy. Because the tumor has the tendency for late recurrence and metastasis, more than 10 years follow-up is indicated. 19 We will continue the follow-up of these patients with SS in a further study. Wide surgical resection is the primary treatment for SS and often in combination with adjuvant or neoadjuvant radiotherapy. It has been reported that the most important factors that influence local recurrence-free survival are negative surgical margins and adjuvant radiotherapy. 20
The National Comprehensive Cancer Network (NCCN) Guidelines recommend radiotherapy after surgery for patients with SS. 21 Song et al reported that adjuvant radiotherapy might lengthen the DFS period in SS patients. 22 Elsewhere, Naing et al observed that radiotherapy was associated with a statistically significant improvement in oncologic outcome for patients with SS based on database of the surveillance, epidemiology and end results (SEER). 23 In the current study, both univariate and multivariate analyses revealed that radiotherapy was an independent predictor factor for survival.
The present study had some limitation. First, this study was retrospective and had a relatively small number of patients. In addition, some of the clinical data (histological types and immunohistochemical expression) in the hospital electronic recording system was incomplete. It is suggested that the future versions of the electronic medical recording system should integrate with the existing information so as to efficiently provide a single source of patient data. Second, survival information of this study was limited as the follow-up time was not long enough to determine 5-year and 10-year survival rates. Building on the obtained results, continuous accumulation of related information will be carried out to expand this work in the future. Therefore, we were able to more accurately describe the clinicopathological characteristics of SS for a more precise prediction of the SS outcomes. Third, because the department of thoracic surgery is one of the largest and top ranked departments in China, there might have been more patients from different regions of the country to the hospital than in other hospitals with a naturally high proportion of patients with thoracic SS. This might contribute sample bias in the present study and hence needs to be taken into consideration during results interpretation.
Conclusion
In summary, this study evidently revealed that age, tumor size and radiotherapy are the potential prognostic risk factors in patients with SS. Older the age, larger the diameter, the worse the prognosis. Furthermore, it was found that the prognosis of SS varies with tumor location. The primary tumors in lower extremities have a better prognosis, while in thorax have a worse prognosis.
Abbreviations
SS, Synovial sarcoma; OS, Overall survival; DFS, disease free survival; STS, Soft tissue sarcomas; FISH, Fluorescence in-situ hybridization; RT-PCR, Reverse transcription polymerase chain reaction; AI, adriamycin + ifosfamide; MAID, Mesna + Adriamycin + Ifosfamide + Dacarbazine; TKIs, Tyrosine kinase inhibitors; NCCN, The national comprehensive cancer network; SEER, The surveillance, epidemiology, and end results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The present study was approved by the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences, Beijing, China (approval number 21/136-2807). Further, this study was conducted in accordance with the Declaration of Helsinki. The information involved in this study was retrospectively collected from the National Cancer Center electronic recording system and did not contain any personal information or privacy. Therefore, the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences determined that the patients consent to review their medical records was not required. Furthermore, all the data from the patients were anonymized or maintained with confidentiality.
Informed Consent
Not applicable, because this article does not contain any studies with human participants or animals.
Trial Registration
Not applicable, because this article does not contain any clinical trials.