
Abstract
Background. A higher Ki-67 labeling index is associated with a poorer prognosis in gastroenteropancreatic neuroendocrine neoplasms. It has also been proposed that the Ki-67 labeling index may increase during disease progression from the primary site to metastatic sites. Although biopsy specimens are used to measure the Ki-67 labeling index, heterogeneity in lesions is thought to affect the assessment of the Ki-67 labeling index. To overcome tumor heterogeneity, we evaluated the variability in the Ki-67 labeling index between primary lesions and hepatic metastases by analyzing only surgically resected specimens. Methods. We conducted a single-center retrospective study to analyze the variability in the Ki-67 labeling index and the change in tumor grade between the primary site and metastatic hepatic sites in 19 patients diagnosed with gastroenteropancreatic neuroendocrine neoplasms at the Cancer Institute Hospital of the Japanese Foundation for Cancer Research from 1998 to 2018. Both the primary site and metastatic hepatic sites were surgically resected. Results. Among the 19 patients with gastroenteropancreatic neuroendocrine neoplasms, 12 patients (63%) showed higher levels of the Ki-67 labeling index at metastatic hepatic sites than at the primary site. The median Ki-67 labeling index levels for the primary lesion and metastatic hepatic lesions were 5% and 10%, respectively. The Ki-67 labeling index levels were significantly elevated in the metastatic hepatic lesions compared to the primary lesion (P = .002). Conclusions. This study addressed the heterogeneity of the Ki-67 labeling index by analyzing only surgically resected specimens. We observed a statistically significant increase in the Ki-67 labeling index in hepatic metastases compared to the primary lesion.
Introduction
Ki-67, a nuclear antigen associated with cell proliferation, has become a useful marker for assessing the malignant potential of neuroendocrine neoplasms (NENs).1–3 The Ki-67 labeling index (Ki-67 LI) is determined by analyzing the cells with the Ki-67 antigen. For gastroenteropancreatic NEN (GEP-NEN), a higher Ki-67 LI is associated with poorer outcomes.4–9 Therefore, a grading system based on Ki-67 LI was proposed by the World Health Organization (WHO) in 2010, which was revised in 2019. 10 According to the WHO 2019 classification, GEP-NEN is divided into four categories on the basis of Ki-67 LI and cell differentiation: NET G1 with a Ki-67 LI <3%; NET G2 with a Ki-67 LI between 3% and 20%; NET G3 with a Ki-67 LI >20% and well-to-moderate cell differentiation; and NET G3 with a Ki-67 LI >20% and poor cell differentiation. The WHO 2019 classification is now a standard system for decision making in the management of GEP-NEN. In recent years, some studies have indicated that Ki-67 LI varies between a primary site and the corresponding synchronous or metachronous metastatic sites,1,2,11 and the reassessment of Ki-67 LI at the metastatic sites or during the disease course may help in predicting prognosis and deciding the management of patients with GEP-NEN. However, not only surgical specimens but also biopsy samples have been used for measuring Ki-67 LI in past studies. However, the use of biopsy samples is problematic due to their heterogeneity, which causes variability in Ki-67 LI measurements.1,2
Therefore, we assessed the variability in Ki-67 LI and the change in tumor grade between the primary site and metastatic hepatic sites by analyzing the surgically resected specimens to address the heterogeneity of Ki-67 LI in GEP-NEN.
Materials and Methods
We conducted a single-center retrospective study at the Cancer Institute Hospital of the Japanese Foundation for Cancer Research. This study included all the patients who were diagnosed with GEP-NEN that had metastasized to only the liver and received radical surgery for primary and metastatic hepatic lesions from 1998 to 2018. Tumor stages were determined by contrast-enhanced computed tomography before surgical resection. We identified 19 patients and analyzed the Ki-67 LI variability and the change in tumor grades (according to the WHO 2017 classification) between the primary and metastatic hepatic sites in these patients. All of them had metastatic synchronous or metachronous hepatic tumors. The primary lesion and synchronous hepatic metastases were resected in the first surgery, and metachronous hepatic metastases were resected in the second surgery. In addition, the 5-year survival rate was defined as the percentage of patients who were alive and followed up 5 years after the first surgery. The cutoff date for the analysis was May 8, 2020. The medical records were retrospectively reviewed to collect the following data: age, sex, primary and metastatic tumor sites, Ki-67 LI, medical therapy including surgical resection, and date of the last follow-up.
This study was approved by the Ethics Committee of the Cancer Institute Hospital of the Japanese Foundation for Cancer Research (No. 2019-1092) and performed in accordance with the Declaration of Helsinki. Since all the data were collected from a medical record system, this study was exempt from the requirement to obtain individual informed consent.
Immunohistochemistry
Serial 5-mm-thick tissue slices were cut from resected specimens fixed with 20% buffered formalin, embedded in paraffin, and 4-μm-thick sections were stained with hematoxylin and eosin. As for specimens of hepatic metastases, the largest tumor was selected among all resected metastatic hepatic lesions for the evaluation of Ki-67 LI. Immunohistochemistry was performed for a representative section of the tumor with a Ki-67 antibody (mouse monoclonal, clone: MIB-1; Dako) and stained with an auto-stainer, Leica Bond-III (Leica Biosystems, Melbourne Pty Ltd).
Pathologists selected a higher Ki-67 labeling area in a low power field (×10 objective lens) first, and they selected the highest Ki-67 labeling area in a middle power field (×20 objective lens) to assess the Ki-67 positivity on the microscopic view. The results were reviewed by two expert pathologists (YT and MT) at our hospital. They were originally reviewed by YT and re-reviewed by MT with visual estimation, except for a case in which the specimen was not available for verification.
Statistical Analysis
Baseline characteristics were expressed as median (range) or number (percentage). Ki-67 LI variability and change in tumor grades between primary and metastatic hepatic lesions or each metastatic hepatic lesion were analyzed using the Wilcoxon signed-rank test, the McNemar test, and the chi-square test. Five-year survival rate was estimated using the Kaplan–Meier method and compared with the log-rank test. A P value < .05 was considered statistically significant. Statistical analysis was carried out using EZR software version 1.40. 12
Results
Patient Characteristics
A total of 19 patients were included in this study. The clinical characteristics of the 19 patients (12 males, 7 females) are shown in Table 1. The median age at diagnosis was 55 years (range: 40-83 years). The primary site was the rectum in 10 patients, the pancreas in 4 patients, the jejunum in 2 patients, and the stomach, bile duct, and papilla of Vater in 1 patient each. As for liver metastases, 8 patients had synchronous metastases. Thirteen patients had metachronous metastases, and 2 of them had both synchronous and metachronous metastases. The median duration between the first and second surgeries was 48.5 months (range: 6.8-175.7 months). Three patients were administered a somatostatin analog and a patient was administered everolimus between the first and the second surgeries. Five patients were administered the somatostatin analog, 5 patients were administered everolimus, and 2 patients were administered peptide receptor radionuclide therapy after the second surgery.
Clinical Characteristics in 19 Patients with NENs.
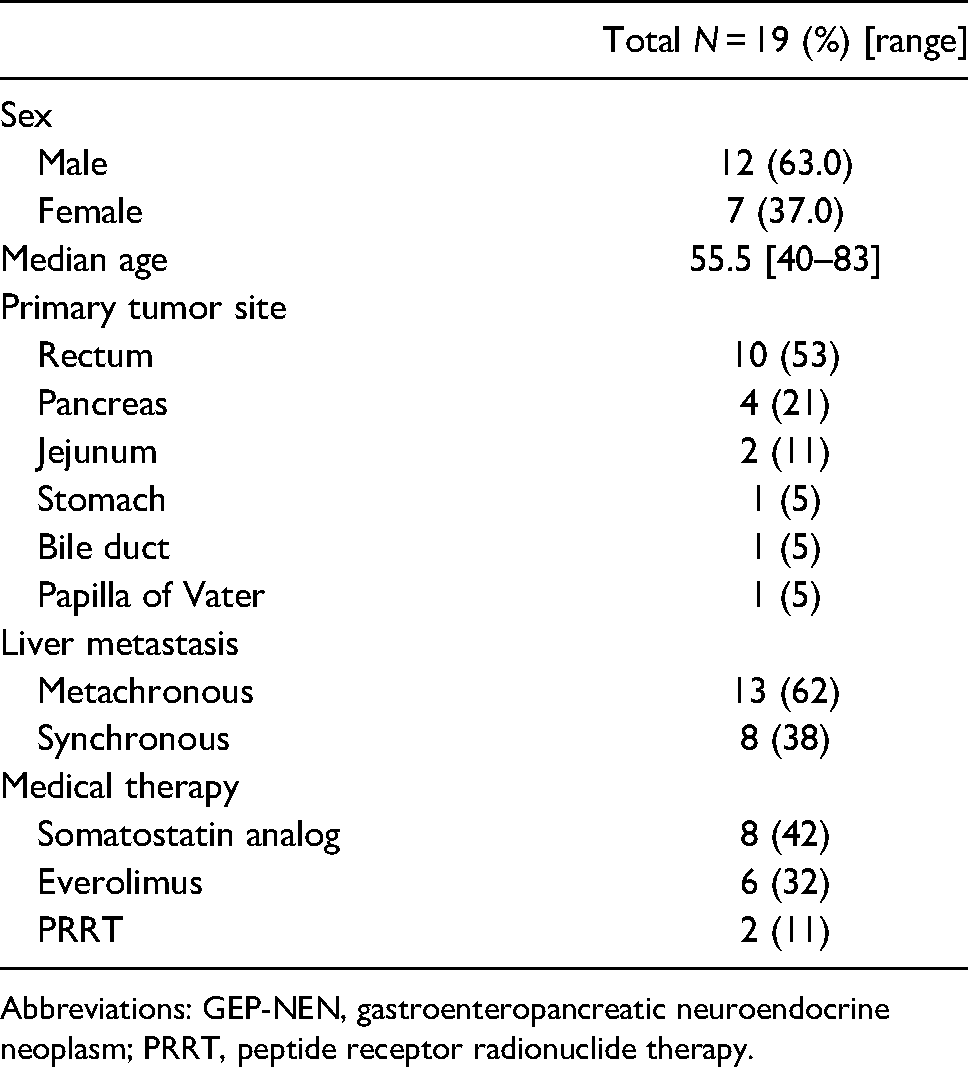
Abbreviations: GEP-NEN, gastroenteropancreatic neuroendocrine neoplasm; PRRT, peptide receptor radionuclide therapy.
Histological Evaluation
Ki-67 LI variability and WHO class change between the primary site and metastatic hepatic sites are summarized in Table 2. A total of 12 patients (63%) showed elevated Ki-67 LI in metastatic hepatic sites compared to that in the primary site. Among them, the rectum was the primary site in 7 patients (Figure 1), the pancreas in 3 patients, and the jejunum and papilla of Vater in 1 patient each. Ten patients had multiple hepatic metastases and 2 patients had a single hepatic metastasis each. Eight patients had metachronous hepatic metastases and 4 patients had synchronous hepatic metastases. Overall, the median Ki-67 LI for primary lesions and metastatic hepatic lesions was 5% and 10%, respectively, and the increase in Ki-67 LI from the primary site to metastatic sites was statistically significant (P = .002) (Figure 2). In addition, in the subset of metachronous hepatic metastases, the median Ki-67 LI for primary lesions and metastatic hepatic lesions was 4% and 10%, respectively, with a statistically significant increase in Ki-67 LI from the primary site to metastatic hepatic sites (P = .014). On the other hand, in the subset of synchronous hepatic metastases, although Ki-67 LI followed an upward trend with median values of 5% and 10% in the primary and metastatic sites, respectively, its elevation was not statistically significant (P = .106).

Parts of histologic images of Case no. 1 in Table 2. The primary rectal NET shows nest or cord-like structure (A), and exhibits low Ki-67 LI (B). The metastatic tumor in the liver shows similar structures of cells with higher nuclear–cytoplasmic ratio and dense chromatin (C), and higher Ki-67 LI (D). Scale bars: 100 µm.
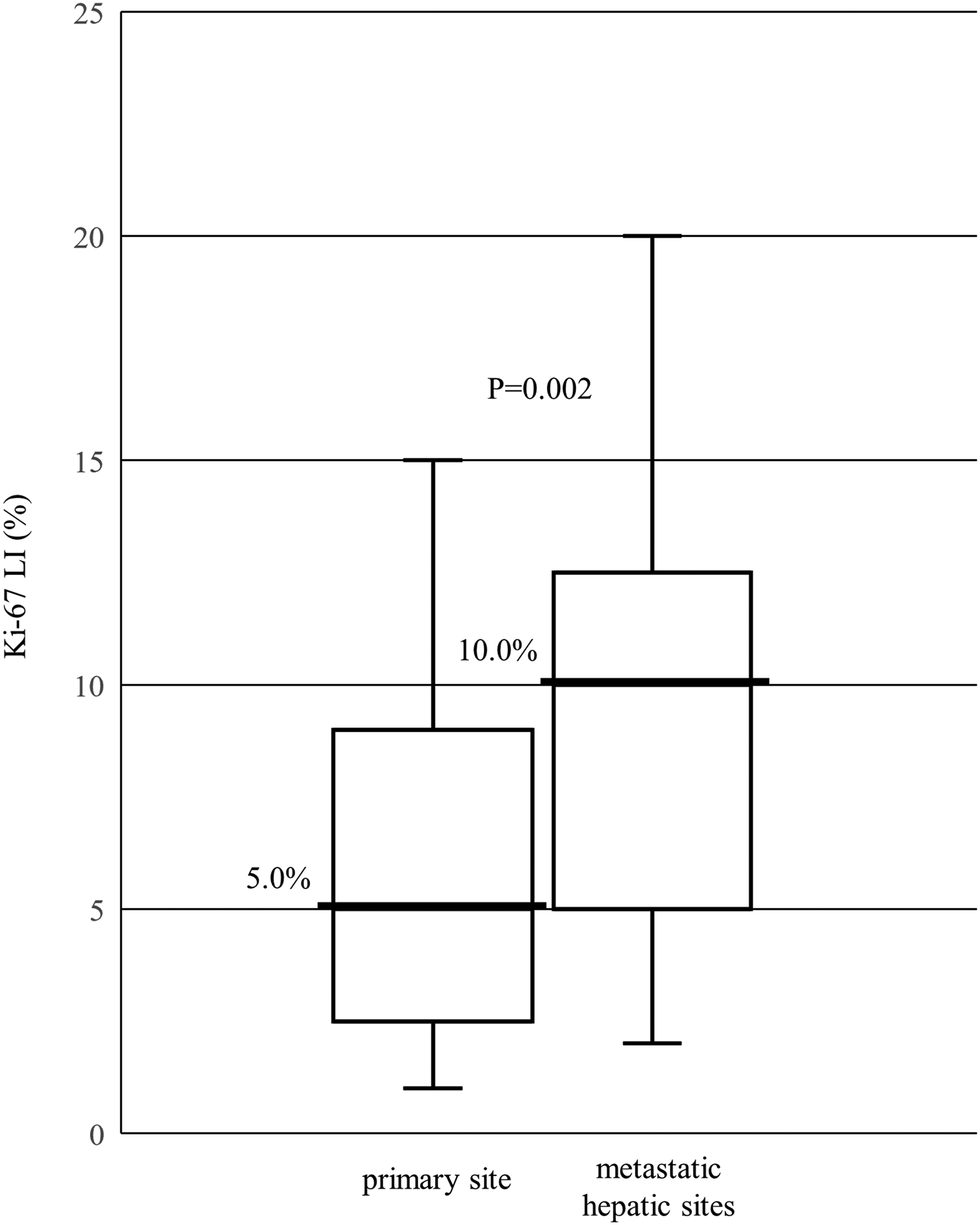
Ki-67 LI change between a primary site and metastatic hepatic sites. Horizontal lines = median values.
Ki-67 LI Variability and WHO Class Change Between the Primary Site and Metastatic Hepatic Sites.
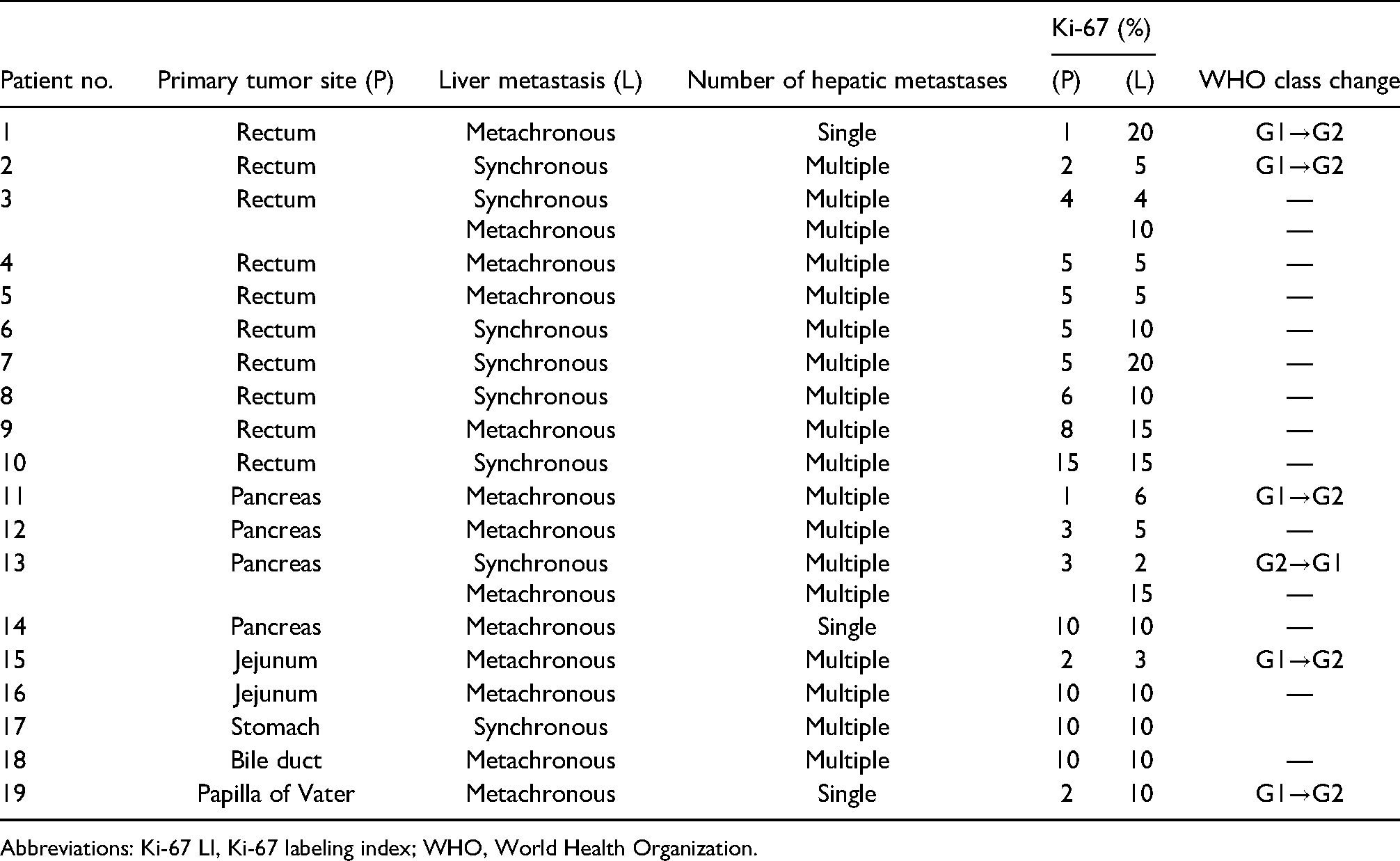
Abbreviations: Ki-67 LI, Ki-67 labeling index; WHO, World Health Organization.
Among the 12 patients who showed increased Ki-67 LI in hepatic metastases, grade increase was observed in 5 patients (42%); however, the difference was not statistically significant (P = .221). In all the 5 patients, the tumor grade changed from G1 to G2, and there was no grade increase from G2 to G3 or G1 to G3. One patient with synchronous hepatic metastases and 4 patients with metachronous hepatic metastases had grade increases. There was no statistically significant difference in grade increase between synchronous and metachronous hepatic metastases (P = .669). As for the primary site in the 5 patients, the rectum was the primary site in 2 patients, while it was the pancreas, jejunum, and papilla of Vater in 1 patient each. In contrast, in 1 patient with the rectum as the primary site, the tumor grade changed from G2 to G1. However, the decrease in Ki-67 LI was only 1%.
Survival Analysis
The 5-year survival rate was 92.3% for all 19 patients, 88.9% for the patients with an increase in Ki-67 LI, and 100% for the patients without an increase in Ki-67 LI. However, the difference between the two groups was not significant (P = .645) (Figure 3).
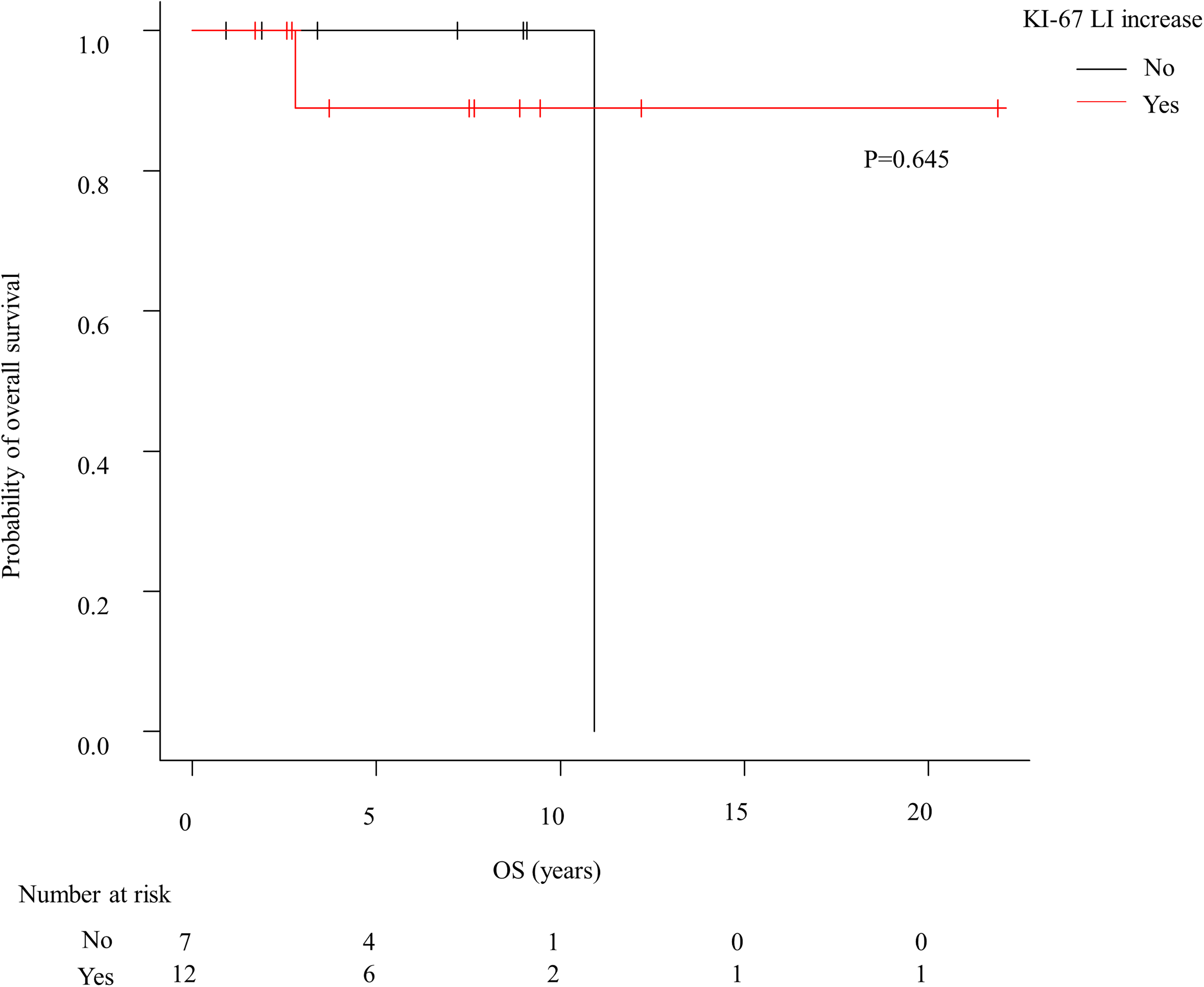
Kaplan–Meier curves of 5-year survival rate in patients with GEP-NEN based on Ki-67 LI variability.
Discussion
It has been proposed in previous reports that Ki-67 LI and the tumor grade may rise from primary to metastatic lesions or during the disease course.13,14 Panzuto et al 15 revealed that an increase in Ki-67 LI occurred in patients with GEP-NEN at the time of progressive disease, and the difference was statistically significant (P < .001). In addition, Grillo et al reported that metastatic lesions in GEP-NEN patients showed an increase in tumor grade compared to a primary lesion. In particular, upgradation occurred more frequently in metachronous metastases than in synchronous metastases. 11 On the other hand, Miller et al 1 reported that Ki-67 LI was higher in metastatic sites than in a primary lesion in only half of the GEP-NEN patients.
Almost all previous studies evaluated Ki-67 LI using biopsy tissue, which is problematic due to the heterogeneity of Ki-67 LI in biopsy specimens; it is not clear whether Ki-67 LI measured in biopsy tissues is truly representative of Ki-67 LI in surgically resected specimens. In this study, we analyzed surgically resected specimens, more than half of which originated from the rectum, to address this problem and to clarify whether Ki-67 LI and tumor grade truly changed between the primary site and metastatic sites. A total of 12 patients (63%) showed a statistically significant increase in Ki-67 LI in metastatic hepatic lesions compared to a primary lesion (P = .002). Specifically, the increases in Ki-67 LI were statistically significant in metachronous hepatic metastases than in primary lesions (P = .014). In contrast, the increases in Ki-67 LI were not statistically significant in synchronous hepatic metastases (P = .106). However, we noted a trend toward an increase in Ki-67 LI in synchronous hepatic metastases, which might reach statistical significance if a larger set of samples were analyzed. Moreover, grade increase was observed in five patients; all of the changes were from G1 to G2. Although the grade increase was not statistically significant, it followed an upward trend (P = .221). Our results support the possibility that Ki-67 and tumor grade may change between a primary lesion and metastatic lesions in patients with GEP-NEN.
On the other hand, there are few reports on the variability in Ki-67 LI among hepatic metastatic lesions. Some differences in Ki-67 LI might exist, not only between primary and hepatic metastatic lesions but also between each hepatic metastatic lesion. However, in clinical practice, it has not been concluded whether we should adopt the average of Ki-67 LI or the highest value of Ki-67 LI among all the hepatic metastases. Therefore, we think that further study would be needed to conclude whether we should assess Ki-67 LI in every metastatic lesion or only in the metastatic lesion that shows the highest Ki-67 LI.
Additionally, in our study, there was a trend toward poorer prognosis in patients with increased Ki-67 LI than in patients without it; the 5-year survival rates were 88.9% and 100%, respectively. Shi et al 13 reported that the variability between primary and metastatic specimens was an independent prognostic factor for survival in patients with GEP-NEN. These results emphasize the importance of reevaluating Ki-67 LI in metastatic lesions or during the disease course to develop a better treatment strategy for GEP-NEN. For patients with disease progression, if tumors show highly increased Ki-67 LI in a reevaluated lesion, systemic chemotherapy and molecular targeted agents will be favored, since further tumor progression can be life threatening. In contrast, if tumors do not show increased Ki-67 LI in a reevaluated lesion, somatostatin analogs or careful surveillance will be selected because these tumors are assumed to be slow growing; if they are small enough to be resected, surgical treatment may be chosen. 16
In clinical settings, it is unrealistic to surgically acquire tissues only for the evaluation of Ki-67 LI in patients with GEP-NEN. However, it is not clear whether Ki-67 LI can be accurately evaluated in biopsy tissues due to its heterogeneity in lesions. Rebours et al 17 reported that Ki-67 LI in metastatic hepatic lesions showed a correlation between bioptic and surgical specimens of pancreatic NEN (PNEN), whereas Ki-67 LI in primary pancreatic lesions did not show a correlation between these specimens. Hasegawa et al 18 revealed that the grading of PNEN with the highest Ki-67 LI in EUS-FNA specimens, which contained adequate cellularity of more than 2000 tumor cells, had a high concordance with grading in surgically resected specimens. It is imperative to recruit a larger number of patients to conclude whether biopsy can truly replace surgical resection to obtain appropriate specimens for the evaluation of Ki-67 LI. In addition, it is necessary to clarify the ideal conditions of biopsy samples for accurate measurement of Ki-67 LI.
There are some limitations that need to be mentioned in our study. This was a retrospective study and a relatively small number of patients were included, which are both common features of studies evaluating rare diseases. Furthermore, we examined only hepatic metastases in this study. Analyses of other metastatic lesions, such as lymph nodes and lungs, to elucidate whether Ki-67 LI and tumor grade vary between the primary site and metastatic sites other than in the liver would improve the study. Finally, our study only dealt with surgically resectable lesions; the median Ki-67 LI in both primary and metastatic lesions was relatively low. Further studies should analyze not only resectable but also unresectable lesions of GEP-NEN to conclude whether the reassessment of Ki-67 LI will improve the clinical management and contribute to better prognosis in patients with GEP-NEN.
Conclusion
In this study, we addressed the heterogeneity of Ki-67 LI in lesions of GEP-NEN by using only surgically resected specimens. In addition, we have revealed that an increase in Ki-67 LI can occur between a primary lesion and metastatic hepatic lesions, especially metachronous hepatic metastases. Based on our results, reassessment of Ki-67 LI may help improve the treatment strategy for GEP-NEN in future clinical practice.
Footnotes
Acknowledgments
We are grateful to Hiroshi Yoko-o, Motoyoshi Iwakoshi, and Sayaka Hirose for their technical assistance.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MO received research grants from Novartis. The other authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The protocol for this research has been approved by a suitably constituted Ethics Committee of the institution and it conforms to the provisions of the Declaration of Helsinki, Committee of Cancer Institute Hospital of Japanese Foundation for Cancer Research, Approval No. 2019-1092.
Informed Consent
Since all data were collected from a medical record system, this study was exempt from the requirement to obtain the individual informed consent.
Trial Registration
Not applicable, because this article does not contain any clinical trials.