
Abstract

To the Editor,
The recent online publication of the article entitled “A histopathologic approach to uterine niche: What to expect and to report in hysteroscopy-resected isthmocele specimens” in the “International Journal of Surgical Pathology”, has shown some absent or scarce histopathologic features in hysteroscopy-resected isthmocele specimens compared to previously reported cases of isthmoceles in hysterectomy specimens.1–5 We became interested in the histopathologic features in isthmoceles that can be identified in hysterectomy specimens which might have been absent or obscured in hysteroscopy-resected isthmoceles. Our aim this time is to compare and contrast the clinicopathologic features of isthmoceles procured from hysterectomy and isthmoplasty specimens.
We retrieved hysterectomy specimens from our pathology archive file that included isthmoceles by performing a retrospective review over a 10-year period. We have collected relevant clinical data for each patient such as age, clinical presentation, number of Caesarean sections, and reason for hysterectomy. We retrieved the hematoxylin and eosin slides of the sampled isthmoceles from each hysterectomy case. We looked for the types of the lining mucosa, luminal contents and the edge wall stroma, as well as the underlying residual myometrial tissue, the scar area, and fibrofatty tissue separating the base of the pouch from the resected uterine margin. We looked for the presence and pattern of hemorrhage, cysts, fibroblastic stroma, metaplasia, epithelial atypia, inflammation and foreign body giant cell reaction. We searched for histopathologic findings which were present in hysterectomy-isthmoceles, but either were not identified or masked in our previous cases of hysteroscopy-isthmoceles. We also recorded accompanying uterine lesions.
We found 32 cases of isthmoceles procured from hysterectomy specimens. On average, the patients in our current hysterectomy group were older than our previous hysteroscopy group (Table 1). The patients complained of menorrhagia, dysmenorrhea and postmenopausal bleeding because they had adenomyosis, leiomyomas, endometrial polyps and endometriosis which were more prevalent in the hysterectomy group. In contrast to hysteroscopy group, brownish mucoid vaginal discharge and intermenstrual (postmenstrual) spotting and bleeding were not reported. The patients had on average similar number of previous Caesarean sections, but of a longer duration since the last Caesarean section. These patients had the choice of hysterectomy for symptomatic relief because they have completed their families. Three patients did not have radiologic investigations, nine cases of the isthmoceles were identified during radiologic investigations, and the remaining isthmoceles were identified during gross pathologic examination of the hysterectomy specimens.
Comparison Between Hysteroscopy-Isthmoceles and Hysterectomy-Isthmoceles.
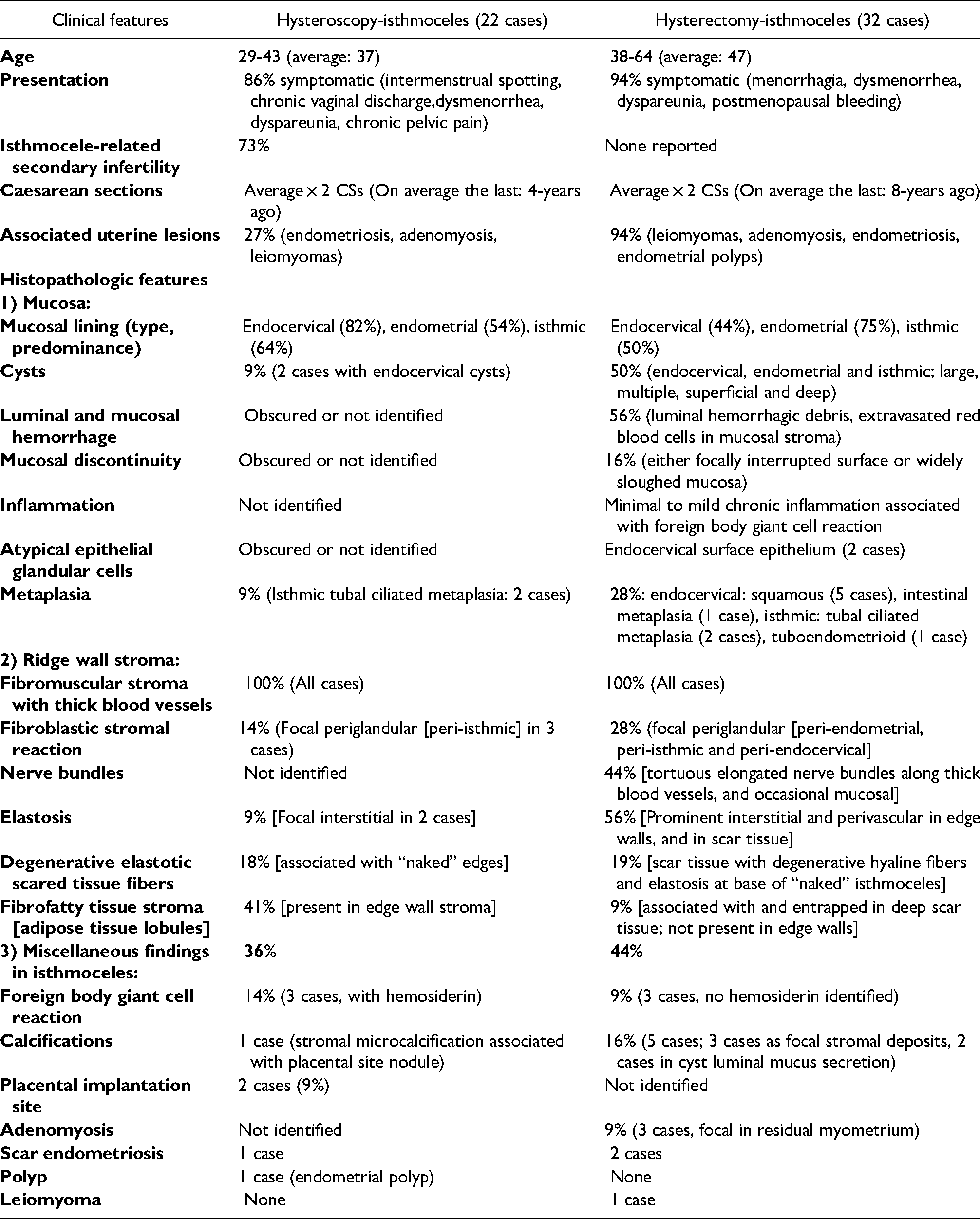
Histologically, similar to our previous series of isthmoplasty specimens, the hysterectomy-isthmoceles showed endocervical, endometrial and isthmic lining mucosa either isolated or combined. However, endometrial lining and isthmoendometrial lining were more prominent in hysterectomy-isthmoceles (Table 1). In contrast to hysteroscopy-isthmoceles, the hysterectomy-isthmoceles showed luminal hemorrhage with cellular degenerate debris material and subepithelial hemorrhagic mucosal stroma and congested capillaries (Figure 1A to C). The mucosal lining showed foci of spontaneous surface sloughing and discontinuity particularly at the base (Figure 1A and C). Similar to hysteroscopy-isthmoceles, endocervical cysts were present, but endometrial and isthmic cysts were also present, were intact, larger, multiple, clustered and distributed superficially and deeply in hysterectomy-isthmoceles (Figure 1E and F). Some were mucosal and edge-based while others were deep in the stroma even some approaching the scar base and underlying adipose tissue (Figure 1E). Some cysts showed calcified secretions (Figure 2E). Endocervical surface epithelium showed occasional foci of atypical epithelial glandular cells (Figure 1D). Similar to hysteroscopy-isthmoceles, ciliated tubal metaplasia was observed in hysterectomy-isthmoceles, which also showed other forms of metaplasia noticeably squamous metaplasia (Figure 2A to D). Similar to hysteroscopy-isthmoceles, the hysterectomy-isthmoceles showed thick fibromuscular stroma with characteristic thick tortuous blood vessels. In addition, hysterectomy-isthmoceles showed prominent tortuous nerve bundles accompanying the edge stromal blood vessels and even some reached the mucosa (Figure 3A). The fibromuscular stromal edge walls in hysterectomy-isthmoceles showed prominent perivascular and interstitial degenerative elastosis (Figure 3B). The base showed degenerative scar tissue with thickened hyaline fibers and elastotic tissue. Some cases showed transepithelial-like elimination of the scare fibers through the mucosa-free base of the isthmoceles (Figure 3C to E). Some cases showed foci of mild chronic inflammation and foreign body giant cell reaction in the stroma (Figure 3F). A few cases showed adenomyosis of the residual and adjacent myometrium, and endometriosis of the basal scar and adipose tissue (Figure 2F). In contrast to hysteroscopy-isthmoceles, hysterectomy-isthmoceles showed smaller amount and distribution of adipose tissue which was occasionally present in the deep scar area, but not in the edge stromal tissue (Figures 1E and 2F).

(.

(.

(.
Both specimen types showed consistent features of fibromuscular stromal edges with thick blood vessels. The miscellaneous findings were comparable between the two specimens (Table 1).
However, hysterectomy-isthmoceles showed some additional histopathologic features that were not identified in our previous study of hysteroscopy-resected isthmoceles. They included luminal and mucosal stromal hemorrhage, congested subepithelial capillaries, mucosal discontinuity, surface epithelial atypia, squamous metaplasia and tortuous nerve bundles. Similar to previous studies of uterine niches examined in hysterectomy specimens, we also found mild fibrosis, scar tissue, adenomyosis, periglandular fibroblastic stroma (Figure 2B and C), and epithelial atypia.2–6 Similar to our series, Karpathiou et al mentioned neural fibers in three cases, and calcified secretions in two cases. 4 However, we did not identify chronic inflammation of the endocervical mucosa which was mentioned in Gubbini et al, Raimondo et al and Karpathiou et al reports.2–4 Other findings were present in hysterectomy-isthmoceles but probably obscured in hysteroscopy-isthmoceles. They included glandular cysts, periglandular fibroblastic stromal reaction, elastosis, mucosal inflammation, degenerative scar tissue and stromal adipose tissue. The reasons for these differences might include several iatrogenic and idiosyncratic factors. One obvious and important reason is the marked cauterization artifacts associated with hysteroscopic specimens. Another reason is that microscopic examination of hysteroscopic samples is limited to resected isthmocele ridges in contrast to the whole intact isthmocele pouch and its surrounding tissues in hysterectomy. A possible reason might include that the fragmented nature of the samples procured from hysteroscopy-isthmoceles result in disorientated and tangentially-cut fragments. On the other hand, patient-related factors, for example small versus large isthmoceles, their histologic components, level relative to the cervix, and characteristics of underlying scar tissue may explain some of the different clinicopathologic features between the cases of hysterectomy-isthmoceles and hysteroscopy-isthmoceles. 6 The patterns of scar changes may give a clue to Caesarean section-related factors and isthmoceles properties. 6 Some of the clinicopathologic differences might indicate two groups of patients with Caesarean section-related isthmoceles depending on their levels, sizes, shapes, contents, and histologic properties of their mucosa, edge wall, surrounding tissue, residual myometrial and scar tissues.1,6 Some findings may have potential pathologic and clinical implications. For example, the surface epithelial atypia and sloughed degenerate epithelial cells might have interpretation pitfalls when examining cervical smears and biopsies. Of note is that endocervicosis in the form of irregularly arranged often cystically dilated endocervical glands has been suggested to be an important factor in the pathogenesis of isthmoceles. 4 This may explain the cystically dilated glands in the endocervical and isthmoendocervical ridge walls in many cases with low-situated isthmoceles in our current and previous case series. This may imply that a rather high incision at a safe distance from the internal os maybe considered by obstetricians during Caesarean sections. 4
In conclusion, for several reasons histopathologic examination of isthmoceles in hysterectomy specimens reveal some additional findings that were either masked or absent in hysteroscopy isthmoplasty specimens. This should be considered and correlated when examining isthmocele specimens.
Footnotes
Author Contributions
BA and RF have retrieved and reviewed the cases, prepared and approved the manuscript, SA has provided the clinical data, reviewed and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.