
Abstract
Special AT-rich sequence-binding protein 2 (SATB2) is a novel, diagnostically useful, and highly sensitive immunohistochemical marker for both primary and metastatic colorectal or appendiceal tumors. In the present study, we aimed to assess the impact of neoadjuvant chemotherapy on SATB2 expression in primary colorectal carcinomas and their corresponding liver metastases. Forty-four patients with colorectal carcinomas who received neoadjuvant chemotherapy were included. SATB2 expression in specimens of biopsy, resected primary colorectal carcinomas, and resected metastatic foci were examined by immunohistochemistry and compared to caudal-type homeobox transcription factor 2 (CDX2). Using a modified H-score, expressions were scored semiquantitatively for both staining intensity and tumor cell proportion with nuclear staining. SATB2 was positive in 43/44 cases (98%) in biopsy specimens, 42/44 cases (96%) in resected colorectal carcinomas with neoadjuvant chemotherapy, and 9/9 cases (100%) with liver metastases. However, these expressions were variably decreased, and the H-score was lower in resected colorectal carcinomas (158 ± 69) than in biopsy specimens (174 ± 60) (p < 0.01). The proportion of SATB2-positive area of colorectal carcinoma was 93% in metastatic foci, while the CDX2-positive area was 78%. When categorized by histopathological tumor regression, the most effective tumors of chemotherapy showed the lowest H-score in resected colorectal carcinomas among the three groups (p < 0.01). SATB2 is a useful marker for both primary colorectal carcinoma and corresponding liver metastases, even with neoadjuvant chemotherapy. However, caution should be exercised when performing needle biopsy for metastatic foci with neoadjuvant therapy because expressions could be decreased, especially in chemotherapy-effective cases, and show immunohistochemically negative results.
Introduction
The special AT-rich sequence binding protein (SATB2) is a member of the AT-rich matrix attachment region-binding transcription factor family involved in transcription regulation and chromatin remodeling. 1 SATB2 was originally characterized as a gene involved in isolated cleft palate defects and subsequently shown to have a role in central nervous system development and osteoblast differentiation.2–4 Recent studies have identified SATB2 as a novel immunohistochemical marker with more than 93% of the tumors positively stained for both primary and metastatic colorectal carcinomas or appendiceal tumors.5–12
For the diagnosis of these tumors, caudal-type homeobox transcriptional factor 2 (CDX2) has been exploited, which is observed in approximately 90%–95% of colorectal adenocarcinomas, and it is considered to be a highly sensitive and specific marker for adenocarcinomas of intestinal differentiation.13–17 CDX2 is expressed within the nuclei of intestinal epithelial cells from the proximal duodenum to the distal rectum, and it regulates gut epithelial development and maturation.18–22 Some reports stated that SATB2 is superior to CDX2 in distinguishing adenocarcinomas of the lower gastrointestinal tract and upper gastrointestinal tract origin.23–25 However, these studies did not include patients who received chemotherapy, and it remains unclear whether this superiority of SATB2 holds true for carcinomas that received chemotherapy.
Chemotherapy plays an important role in the treatment of colorectal carcinomas. Patients with unresectable colorectal carcinomas benefit from chemotherapy, which has been shown to shift the clinical stage toward a technically resectable condition. 26 Patients with stage III and high-risk stage II colorectal carcinomas also benefit from adjuvant chemotherapy, as shown by the decreased risk of recurrence. 27 However, the impact of chemotherapy on SATB2 expression status remains poorly understood, although the expression of several gene products was previously shown to be affected by chemotherapy. 28
These previous studies did not mention the percentage of cases with neoadjuvant therapy that shows the loss of SATB2 expression, nor did they assess the extent of expression loss. We hypothesized that specimens from tissues that received chemotherapy would show variably decreased expression and might be decreased to influence diagnosis even if they were classified as positive in previous studies. In the present study, we aimed to assess the impact of chemotherapy on SATB2 and CDX2 expressions in primary colorectal carcinomas and their corresponding liver metastases.
Materials and Methods
Ethical Approval
This study was performed in accordance with the tenets of the Declaration of Helsinki. Study approval was obtained from the institutional ethical committee, including members from outside the institution (Institutional Approval Number 20-96).
Patients Selection
We retrospectively identified 58 consecutive patients with colorectal carcinomas from the surgical pathology archives of our hospital between January 2010 and March 2020. The inclusion criteria for the study were: (1) a diagnosis of adenocarcinoma of the colon, rectosigmoid junction, or rectum; (2) use of chemotherapy before surgical resection of the primary tumor; (3) adequate residual viable tumor in the resection specimen for immunohistochemical studies; and (4) available pretreatment biopsy material. The exclusion criteria were as follows: (1) colorectal carcinomas that were not treated with chemotherapy and (2) colorectal carcinomas that showed complete therapeutic response and no viable tumor. Forty-four patients with resection of colorectal carcinomas met these criteria and were included in the study group. The original glass slides of these cases were reviewed, the diagnosis was confirmed, and the “best tumor block” was identified. The preoperative biopsy material corresponding to the resected tumors and metastases were all examined with hematoxylin and eosin staining and immunohistochemistry for any given patients. Subtypes were classified based on the World Health Organization (WHO) Classification of Tumours, fifth edition. 29 Histopathological tumor regression of resected specimens was evaluated following the established system of the American Joint Committee on Cancer (AJCC) 2017. 30 In summary, tumor regression was scored as follows: 0, no viable cancer cells; 1, single cells or rare small groups of cancer cells; 2, residual cancer with evident tumor regression, but more than single cells or rare small groups of cancer cells; and 3, extensive residual cancer with no evident tumor regression. In the current study, patients with a score of 0 were excluded because they indicated no viable cancer cells. Patients with score 1 were called as Group1, those with score 2 were classified as Group 2, and those with score 3 were classified as Group 3. Clinical information regarding patients’ age, sex, and tumor site was retrieved from the patients’ medical records and pathology reports.
Immunohistochemistry and Interpretation
One representative formalin-fixed paraffin-embedded carcinoma block in each case was chosen for immunohistochemical analysis. Immunohistochemistry was performed using antibodies against SATB2 (clone EP281, 1:200; Cell Marque, Rocklin, CA, USA), CDX2 (clone EPR2764Y, 1:3000; Genetex, Irvine, CA), and MSH6 (clone 44, 1:100; BD Biosciences, San Diego, CA) on 3-μm-thick unstained whole tissue sections using Ventana BenchMark ULTRA, an automated immunohistochemical staining system, according to the manufacturer‘s recommendations (Ventana Medical System, Tucson, AZ, USA). Microscopic review of immunohistochemistry was performed by two pathologists (Y. A. and H. H.), and discrepancies were resolved by consensus review.
SATB2- and CDX2-positive tumors were defined as nuclear staining in tumor cells, regardless of either staining intensity or tumor cell proportion with nuclear staining. SATB2 and CDX2 were scored semiquantitatively for both staining intensity and tumor cell proportion with nuclear staining. Staining intensity was scored as follows: 0, absent; 1 + , weak nuclear staining visible with 10 × or greater objective magnification; 2 + , strong nuclear staining visible at 2 × or 4 × objective magnification.
The percentage of tumor cells with nuclear staining was estimated by visual inspection, which was the proportion of tumor cells with nuclear staining to the whole tumor cells. This percentage is named “positive area” in the current study. Examples of the subclassified specimens are shown in Figure 1. A modified H-score for SATB2 and CDX2 was calculated using the following formula: H-score = (intensity score) × (positive area). A modified H-score between 0–200 was obtained, where the maximum score of 200 was equal to 100% of the tumor cells stained strongly (2 + ) as calculated.

A–C, examples of the classification according to the response to chemotherapy (hematoxylin and eosin stain); D–E, nuclear intensity score (comprising one component of the histologic score) of SATB2 in colorectal carcinomas. A, Group 1: single cells or rare small groups of cancer cells. B, Group 2: residual cancer with evident tumor regression, but more than single cell or rare small groups of cancer cells. C, Group 3: extensive residual cancer with no evident tumor regression. D, 0 intensity. E, 1 + intensity. F, 2 + intensity.
For mutS homolog 6 (MSH6), preserved expression was defined as nuclear staining within tumor cells, using normal stroma and mucosa as internal positive controls. Loss of protein expression for MSH6 was the regional absence of nuclear staining regardless of focal or diffuse area within tumor cells with concurrent positive labeling in internal non-neoplastic cells.
Prior to the assessment, we confirmed that immunohistochemical staining was equally positive in normal epithelial tissues of both biopsy and resected primary colorectal carcinomas, which would make it valid to compare the immunohistochemical expression between these and assess the impact of chemotherapy on immunohistochemical expression.
Statistical Analysis
All statistical analyses were conducted using R (version 3.1.3; The R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p < 0.05. Student‘s t-test and Mann–Whitney U test were used for two-group comparisons of numerical values. The Mann–Whitney U test with Bonferroni correction of p-values was applied in three-group comparisons.
Results
The demographic and clinicopathological characteristics of all patients with colorectal carcinomas are summarized in Table 1. The study group included 27 male and 17 female patients with a mean age of 64 years (range, 28-79 years). Thirty-nine (89%) primary colorectal carcinomas were diagnosed with adenocarcinoma NOS, with four adenoma-like adenocarcinomas (9%) and one serrated adenocarcinoma (2%) by histological assessment. A total of 38 (86%) patients had left-sided colorectal carcinomas. Thirteen patients had liver metastases, and 12 of them underwent metastasectomy. Viable cancer cells were detected in nine patients, and no viable cancer cells remained in the three. All 44 patients in this study received neoadjuvant chemotherapy but not radiation therapy.
Clinical and Histological Patient Characteristics.
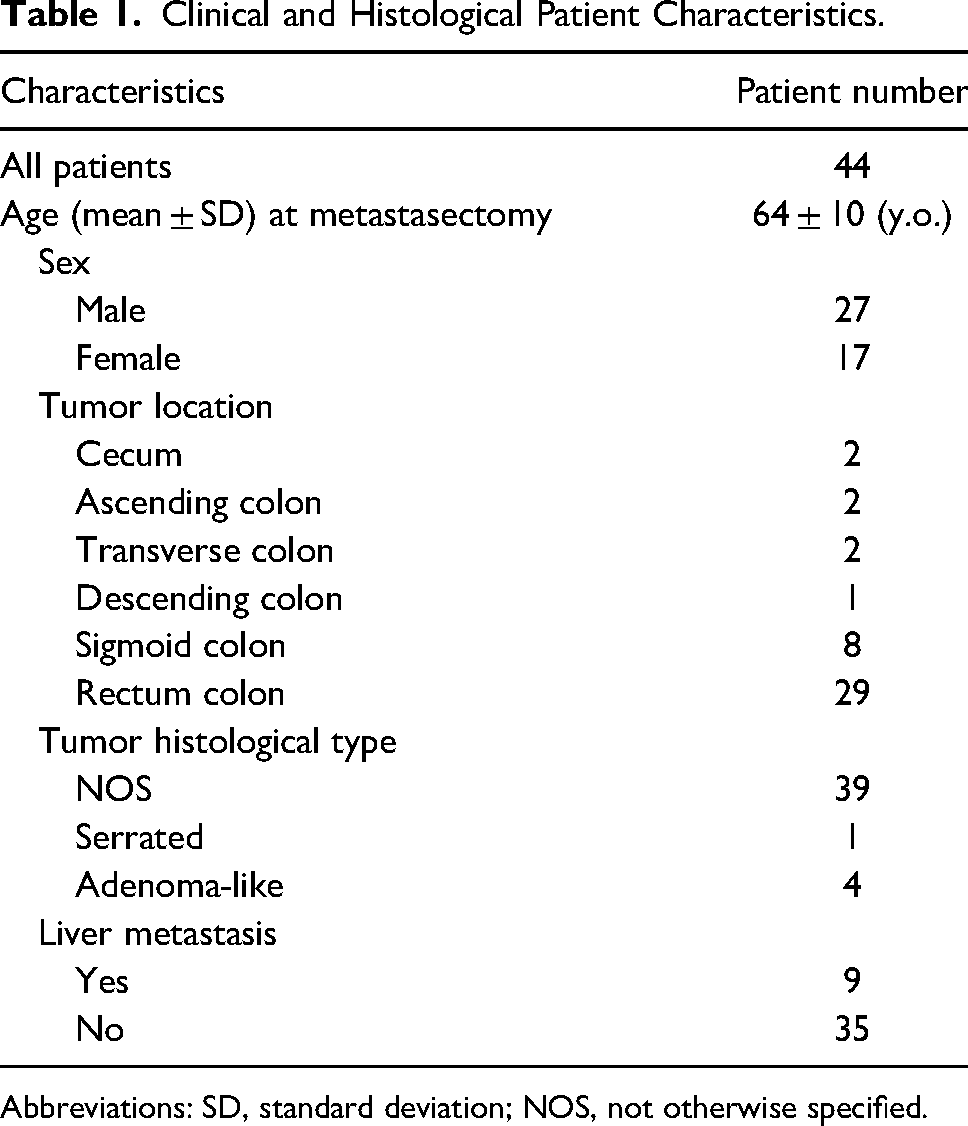
Abbreviations: SD, standard deviation; NOS, not otherwise specified.
SATB2 expression was positive in 43/44 cases (98%) in biopsy, 42/44 (96%) in resected colorectal carcinomas with neoadjuvant chemotherapy, and 9/9 (100%) of the corresponding liver metastases (Table 2). In contrast, CDX2 expression was positive in 43/44 cases (98%) in biopsy, 41/44 (93%) in colorectal carcinomas with neoadjuvant chemotherapy, and 9/9 (100%) in corresponding liver metastases. The SATB2 H-score on biopsy was 174 ± 60 (mean ± SD) and 159 ± 70 in colorectal carcinomas with neoadjuvant chemotherapy. There was also a significant difference in the SATB2 H-score between biopsy and colorectal carcinomas with neoadjuvant chemotherapy (p < 0.01). The CDX2 H-scores in biopsy were 180 ± 51 and 151 ± 71 in colorectal carcinomas with neoadjuvant chemotherapy, and there was a significant difference in the CDX2 H-score between biopsy and colorectal carcinomas with neoadjuvant chemotherapy (p < 0.01). There was no significant difference between SATB2 and CDX2 in either biopsy or colorectal carcinomas with neoadjuvant chemotherapy (p = 0.62 and p = 0.63, respectively). Among the nine patients who had viable cancer cells in liver metastasis, the SATB2 H-score in biopsy was 171 ± 59 and 187 ± 28 in metastatic foci, while the CDX2 H-score in biopsy was 142 ± 70 and 147 ± 57 in metastatic foci (Table 2). Neither SATB2 nor CDX2 showed any significant difference in H-score between colorectal carcinomas with neoadjuvant chemotherapy and corresponding metastases (p = 0.11 and p = 0.13, respectively). Furthermore, the proportion of areas where tumor cells showed nuclear staining was 93% in SATB2% and 78% in CDX2, which was not statistically significantly different (p = 0.13). However, there was a significant difference between SAB2 and CDX2 H-scores in metastasis (p = 0.04). Example images of SATB2 and CDX2 expression in a case of colorectal carcinoma and its corresponding liver metastasis are shown in Figure 2.

Example images of marker expressions in one patient with colorectal carcinoma and the corresponding liver metastasis. A, SATB2, resected colorectal carcinoma with neoadjuvant chemotherapy. B, CDX2, resected colorectal carcinoma with neoadjuvant chemotherapy. C, SATB2, metastasis. D, CDX2, metastasis. SATB2 was strongly positive in resected colorectal carcinoma with neoadjuvant chemotherapy (A) and the corresponding metastasis (C). However, CDX2 was weakly positive in resected colorectal carcinoma with neoadjuvant chemotherapy (B) and its corresponding metastasis (D), although these specimens were obtained from the same patient.
SATB2, CDX2 and MSH6 Immunohistochemical Results Stratified by Primary and Metastatic Colorectal Carcinoma.
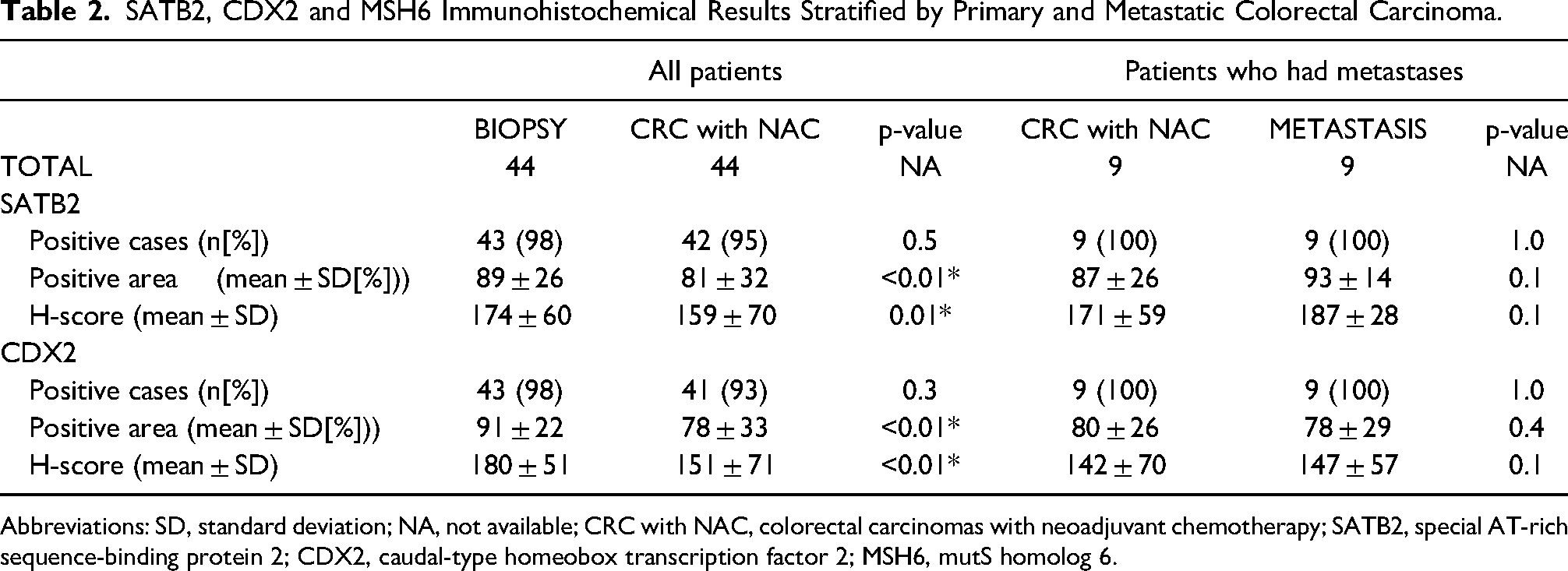
Abbreviations: SD, standard deviation; NA, not available; CRC with NAC, colorectal carcinomas with neoadjuvant chemotherapy; SATB2, special AT-rich sequence-binding protein 2; CDX2, caudal-type homeobox transcription factor 2; MSH6, mutS homolog 6.
Among all 44 cases, 43 (98%) showed positive expression of MSH6 in biopsy, but only 33 (75%) were positive for primary colorectal carcinomas; 4/9 cases (44%) were positive for metastases. There was no significant difference in the SATB2 or CDX2 H-scores in primary colorectal carcinomas between the MSH6 positive and negative groups (p = 0.78 and p = 0.29, respectively) (Table 3).
SATB2, CDX2 Immunohistochemistry Results Stratified by MSH6 Expression.
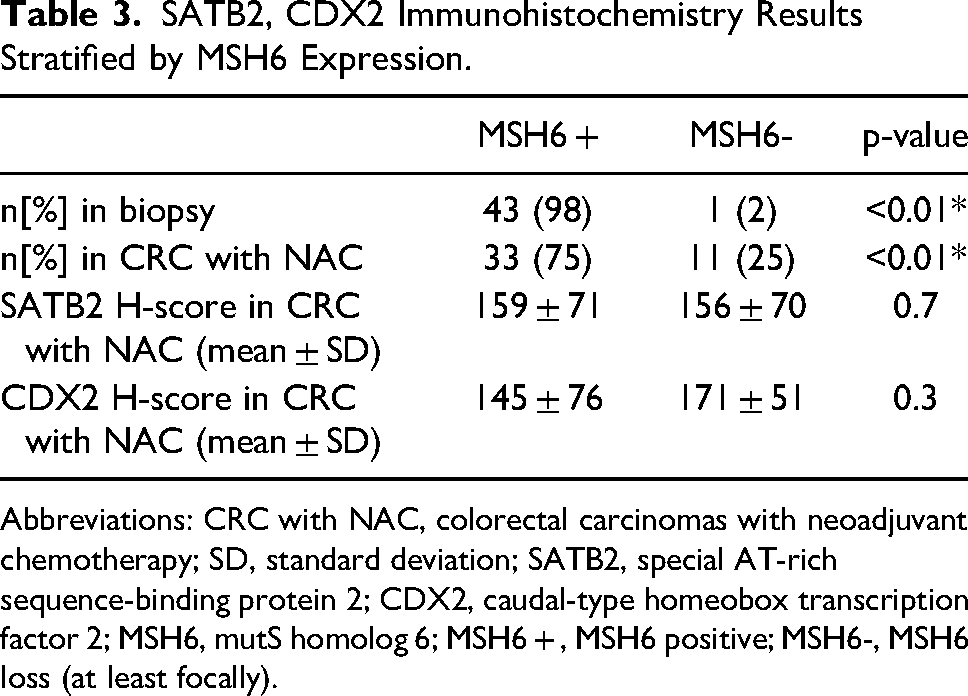
Abbreviations: CRC with NAC, colorectal carcinomas with neoadjuvant chemotherapy; SD, standard deviation; SATB2, special AT-rich sequence-binding protein 2; CDX2, caudal-type homeobox transcription factor 2; MSH6, mutS homolog 6; MSH6 + , MSH6 positive; MSH6-, MSH6 loss (at least focally).
When all 44 patients were categorized by histopathological tumor regression of resected specimens following the AJCC 2017, 6 were classified as Group 1, 20 as Group 2, and 18 as Group 3. There was no significant difference in the SATB2 H-score between any of these groups in biopsy, while the CDX2 H-score was significantly the lowest in the biopsy of Group 1 (p < 0.05). On the other hand, both SATB2 and CDX2 H-scores in primary colorectal carcinomas showed significant differences between Groups 1 and 2 (p = 0.01 and p < 0.001, respectively) and Groups 1 and 3 (p = 0.01 and p < 0.001, respectively) (Figure 3). Examples of different SATB2 and CDX2 expression levels according to the response to chemotherapy are shown in Figure 4.
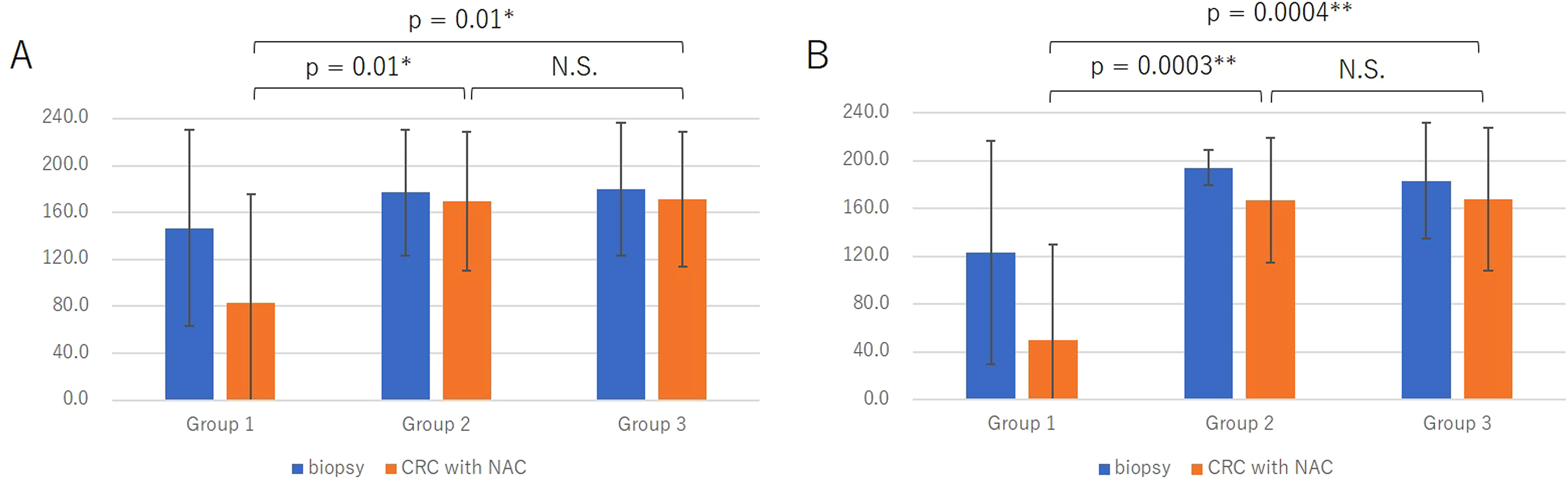
H-score of SATB2 and CDX2 in specimens of biopsy and resected colorectal carcinomas of all patients. A, SATB2. B, CDX2. A significant difference was observed in the H-score of SATB2 between Groups 1 and 2 and Groups 1 and 3, while no significant difference was observed between Groups 2 and 3. A significant difference was also observed in the H-score of CDX2 between Groups 1 and 2 and Groups 1 and 3, while no significant difference was observed between Groups 2 and 3.

Example images of marker expressions in two cases with colorectal carcinomas stratified by the classification of response to chemotherapy. A, SATB2, biopsy, Group 1. B, SATB2, colorectal carcinoma with neoadjuvant chemotherapy, Group 1. C, SATB2, biopsy, Group 3. D, SATB2, colorectal carcinoma with neoadjuvant chemotherapy, Group 3. E, CDX2, biopsy, Group 1. F, CDX2, colorectal carcinoma with neoadjuvant chemotherapy, Group 1. G, CDX2, biopsy; Group 3. H, CDX2, colorectal carcinoma with neoadjuvant chemotherapy, Group 3. Strong expression of SATB2 was observed in the biopsy specimen (A), while the expression was conspicuously decreased, although it remained positive in colorectal carcinoma with neoadjuvant chemotherapy specimen that was classified as Group 1 (B). On the other hand, strong expression of SATB2 was observed in the biopsy specimen (C) and was as strong in colorectal carcinoma with neoadjuvant chemotherapy specimen (D), which was classified as Group 3 because it showed a poor response to chemotherapy. A similar pattern was observed for CDX2 (E–H).
Discussion
In this study, we found that both SATB2 and CDX2 showed variably decreased expression in colorectal carcinomas with neoadjuvant chemotherapy, with more decreased expression in chemotherapy-effective tumors, although most of these expressions were regarded as SATB2- or CDX2-positive. To our knowledge, there have been few studies on SATB2 expression in colorectal carcinomas treated with neoadjuvant chemotherapy. Our study is unique because we included only patients with colorectal carcinomas who underwent the following procedure: biopsy, preoperative chemotherapy (neoadjuvant chemotherapy), and resection of primary colorectal carcinomas, with or without metastasectomy, which allowed us to precisely assess SATB2 and CDX2 expression after chemotherapy.
In our study, both SATB2 and CDX2 expressions were positive in 98% of the biopsy specimens, and 96% and 93%, respectively, in colorectal carcinomas with neoadjuvant chemotherapy. This rate of positivity is concordant with previous studies that included cases with or without chemotherapy5,7,31,32 and shows that SATB2 and CDX2 are useful immunohistochemical stains for cases with neoadjuvant chemotherapy. However, among the colorectal carcinomas with neoadjuvant chemotherapy and metastases with positive SATB2 or CDX2 expression, the intensity and immunohistochemically stained areas were variably decreased. In addition, there was no significant difference in H-scores between primary colorectal carcinomas and metastases in our study, which would indicate that the impact of chemotherapy on SATB2 and CDX2 was irrelevant to primary colorectal carcinoma or metastasis, and metastatic specimens would show equally decreased positive expression as the primary colorectal carcinomas. We think this result is clinically important because if one detects metastasis and performs needle biopsy on it in patients with colorectal carcinomas that were treated with neoadjuvant therapy, the needle biopsy specimens could show negative expression of SATB2 or CDX2 when the biopsied tissue is the area where SATB2 or CDX2 expression is lost due to chemotherapy. Thus, caution should be exercised when interpreting immunohistochemical stains for SATB2 and CDX2 in the neoadjuvant setting and consider evaluating SATB2 and CDX2 immunoexpression in pretreatment tumor samples in the diagnosis of primary colorectal carcinomas.
Interestingly, although significant differences were not observed between SATB2- and CDX2-positive area of metastatic specimens in the current study, SATB2 showed a larger area of positivity than CDX2 (93% and 78%, respectively). Moreover, SATB2 showed a significantly higher H-score in metastatic specimens than in CDX2, suggesting that SATB2 is more useful than CDX2 in the diagnosis based on the biopsy of metastasis, especially because the larger negative area or weaker positive expression in metastasis makes it more likely for the diagnosis of the needle-biopsied specimen to regard it as immunohistochemically negative. Indeed, a previous study by Yasuyuki et al reported that although 96.3% of colorectal carcinomas that received chemotherapy showed CDX2 positivity, 22.2% of their study cohort showed heterogeneous CDX2 expression. 31
Among the groups classified according to the response to chemotherapy, Group 1, which showed the best response to neoadjuvant chemotherapy in primary colorectal carcinomas, had the lowest H-score of SATB2 and CDX2 among the three groups. This result supports our hypothesis that immunohistochemical expression can be decreased by chemotherapy in patients with colorectal carcinomas. We also hypothesized that immunohistochemical expression in biopsy specimens might correlate with the response to chemotherapy because the H-score of biopsy specimens in Group 1, which showed better response to neoadjuvant chemotherapy, was smaller than that in Groups 2 and 3, which showed less response to neoadjuvant chemotherapy. Indeed, the biopsy specimens of Group 1 showed the lowest H-score in CDX2. However, there was no significant difference in the SATB2 H-score of biopsy specimens among the three groups in the current study. This statistically insignificant difference might be due to the small number of patients in Group 1 compared to the other groups. Furthermore, there have been a few reports on SATB2 expression and response to chemotherapy. A recent prospective cohort study reported that patients with metastatic colorectal carcinomas expressing high levels of SATB2 had better prognosis and response to chemotherapy than those with low SATB2 expression, and patients with both low SATB2 expression and mutated BRAF had a particularly poor prognosis. 32
In our study, Group 1, which showed the best response to neoadjuvant chemotherapy, showed significantly lower H-score of SATB2 than other groups. Apparently, this might seem contradictory to the previous reports that lower expression of SATB2 is related to poor prognosis and response to chemotherapy. 32 However, the previous study employed non-resectable colorectal carcinomas without chemotherapy for SATB2 staining, which later received palliative chemotherapy, and studied the relationship between SATB2 expression and response to chemotherapy. 32 Therefore, the condition of primary colorectal carcinoma specimens when they were used for SATB2 staining is different from our study, which included only those with neoadjuvant chemotherapy. Another report showed that high SATB2 expression is an independent marker of good prognosis in colon cancer and may modulate sensitivity to chemotherapy and radiation. 33 This previous study included both colorectal carcinomas with and without neoadjuvant chemotherapy, and overall SATB2 high expression was related to better prognosis. 33 However, they also mentioned that significant difference was not found between high and low SATB2 expression in stage III–IV rectal cancers with neoadjuvant chemotherapy subgroup Cox proportional hazards analysis. Again, our study did not study prognosis and simply found that colorectal carcinomas with good response to neoadjuvant chemotherapy were likely to show decreased SATB2 expression, which led us to believe that chemotherapy could impact SATB2 expression.
Regarding the relationship between MSH6 and SATB2 expression in colorectal carcinomas with neoadjuvant therapy, one report showed that the extensive loss of MSH6 staining with microsatellite stability was observed in 19% of colorectal carcinomas with neoadjuvant chemotherapy. 34 In our study, 22% of all cases showed at least regional focal loss of MSH6 immunohistochemical expression in colorectal carcinomas with neoadjuvant chemotherapy, although they showed positive expression in biopsy specimens. This result is concordant with a previous report. 34 We speculated that if chemotherapy-effective tumors show decreased expression of CDX2 or SATB2, these tumors might be more likely to show the loss of MSH6 expression than chemotherapy-resistant tumors. However, no significant difference in the H-score was found between MSH6-positive and -negative tumors. We conjectured that neoadjuvant chemotherapy caused the loss of MSH6 independently in both SATB2-positive and -negative groups, which made the difference between these groups statistically insignificant. The mechanism by which neoadjuvant chemotherapy induces loss of MSH6 immunohistochemical expression is unknown, although it may result from therapy-induced mutations, epigenetic changes such as DNA methylation, or dysregulation of cell cycling in mismatch repair proficient tissues. 34
Some heterogeneity of nuclear markers with fixation in resected tissues could be a limitation. However, all tumors were formalin-fixed under similar conditions and examined using statistical analyses. In addition, equally positive immunohistochemical staining in normal epithelial tissues was confirmed in all biopsy and resected colorectal carcinoma specimens before analyses. Therefore, we believe our methodology is adequate.
Other limitations include its retrospective nature and the size of the study cohort. It is possible that the relatively small size of the study cohort may have influenced the results. For example, the number of patients with SATB2-negative colorectal carcinomas is small, and the results might not be sufficiently powered to detect a difference between the MSH6-positive and -negative groups. The number of patients in Group 1, the best chemotherapy-effective cohort, was also small compared to that of the other two groups. Further large-scale prospective studies with detailed genetic analyses are warranted to elucidate the impact of chemotherapy or tumor progression in SATB2-negative colorectal carcinomas and validate our findings.
Conclusion
SATB2 and CDX2 expression status in colorectal carcinomas was highly concordant between biopsy specimens, resected primary colorectal carcinomas with neoadjuvant therapy and their corresponding liver metastases. Although SATB2 positivity was variably decreased after chemotherapy, especially in chemotherapy-effective tumors, SATB2-positive areas were larger than that of CDX2 in metastatic foci. These facts indicated diagnostical usefulness of SATB2 in colorectal carcinomas even with chemotherapy or metastasis.
Footnotes
Acknowledgments
Author Contributions
Y.A. and H.H. designed the study and collected data as well as drafted the main manuscript. Y.A., H.H. and T.M. were responsible for the pathological diagnosis. T.N. was responsible for surgical specimens. Y.A., H.H., M.A., T.N. and T.M. reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI (grant number JP18K15103).
Ethical Approval
Ethics committee of NTT Medical Center Tokyo; Approval number: 20-96.
Informed Consent
We provided means for patients to opt-out of the study on the hospital homepage.
Trial Registration
Not applicable, because this article does not contain any clinical trials.