
Abstract
Appendiceal endometriosis is a rare entity and, when accompanied by intestinal metaplasia, represents a challenging differential diagnosis with low-grade appendiceal mucinous neoplasm (LAMN). We present the case of a 47 years-old woman, with multiple surgical interventions for endometriosis, with persistent symptoms despite chronic hormonal treatment, with imaging showing stage IV endometriosis. Hence, en bloc low rectum resection with total hysterectomy and bilateral adnexectomy was performed, followed by appendectomy. Unexpectedly, despite the gross normal macroscopic appearance of the appendix, microscopy showed multiple endometriosis foci, consisting of endometrial glands embedded in varying amounts of endometrial stroma. As some of these glands were bordered by mucinous-type epithelium containing intestinal cells, Goblet cells, Paneth cells in addition to the presence of mucus-filled microcysts, immunohistochemistry (IHC) was performed in order to differentiate between intestinal-metaplasia and LAMN. IHC showed positivity of the endometrial epithelium for KRT7, estrogen receptor (ER) and progesterone receptor (PR). Both the appendiceal mucosa and the intestinal-type metaplastic epithelium of the glandular structures were positive for KRT20. Additionally, the endometrial stroma enclosing endometrial glands, as well as the stroma surrounding mucinous-type metaplastic epithelium, were positive for CD10, ER and PR. This patient's case draws attention to the rare occurrence of appendiceal endometriosis and the uncommon intestinal metaplasia, which can easily mimic LAMN, emphasizing the paramount importance of the differential diagnosis with this type of neoplasia.
Keywords
Introduction
The presence of ectopic endometrial tissue outside the uterus is known as endometriosis. It has a prevalence of 5-15% between the reproductive aged woman and can cause infertility and chronic pelvic pain. 1 Endometriosis can occur anywhere in the body. The most common sites are the ovaries, followed by broad ligaments, fallopian tubes, sigmoid colon and appendix. 2 The intestinal tract involvement by endometriosis in patients with pelvic disease is outlined in 15-37% of cases. 3 Von Rokitansky was the first to describe the presence of endometrial tissue in the appendix in 1860. 4 Since then, several studies have reported the presence of endometrial glands and stroma in the appendiceal wall with interesting clinical aspects. One familiar situation is when endometriosis of the appendix presents as acute appendicitis.5–7 Other common situations include chronic abdominal and right lower quadrant pain, nausea, vomiting, inflammatory mass formation, intussusception, perforation or may also be an incidental finding in an asymptomatic patient. 3 Despite its rare incidence, appendiceal endometriosis is not known to cause any diagnostic problems for the clinician. However, there are few particular cases with uncommon microscopic findings that can mimic a low-grade appendiceal mucinous neoplasm (LAMN), such as intestinal-type metaplasia or intestinal-type colonization of endometrial glands in the appendiceal wall. 8
We report the case of an interesting patient with appendiceal endometriosis with focal transformation of endometrial type epithelium into mucinous intestinal-type epithelium in a lady with history of uterine, ovarian and rectum endometriosis.
Case Report
A 47-year-old female patient, with extensive surgical past medical history (resection of ovarian endometrioma with 9 years prior to admission to our hospital, followed by hysteroscopic resection of an endometrial polyp one year later and hysteroscopic intervention for uterine synechiae two years later, with a Caesarean section after two years), with chronic hormonal medication for endometriosis, was admitted to our hospital with 6 months history of persistent pelvic pain, accompanied by episodes of metrorrhagia and rectal bleeding, with no change in bowel movement. Clinical examination was unremarkable, except for fresh blood in the stools on digital rectal examination, with no haemorrhoids.
Laboratory tests were unremarkable, except for mild inflammatory syndrome, with fibrinogen 416 mg/dl (normal range 150-400 mg/dl) and C-reactive protein 1.06 mg/dl (normal range 0-0.32 mg/dl). Infection screening was negative, except for positive human papillomavirus (HPV) test for high risk HPV45, but without any intraepithelial lesion or malignancy. Abdominal ultrasound was normal, but transvaginal ultrasound detected a fixed isthmic area of the uterus due to a rectosigmoid endometriotic nodule. In accordance with this, colonoscopy found a mild stenosis (20%) of the superior rectum, with erythema of the anterior wall. Given the endometriotic involvement of the rectum, an abdominopelvic MRI was done. This showed stage IV endometriosis, with heterogenous aspect of the uterus due to adenomyosis and fibromatous lesions, bilateral ovarian endometriomas (right 13 mm and left 24 mm), multiple adhesions to the adjacent organs and submucosal rectal endometriosis, 33 mm length and 13 mm depth, with grossly normal appearance of the appendix (Figure 1, 2).
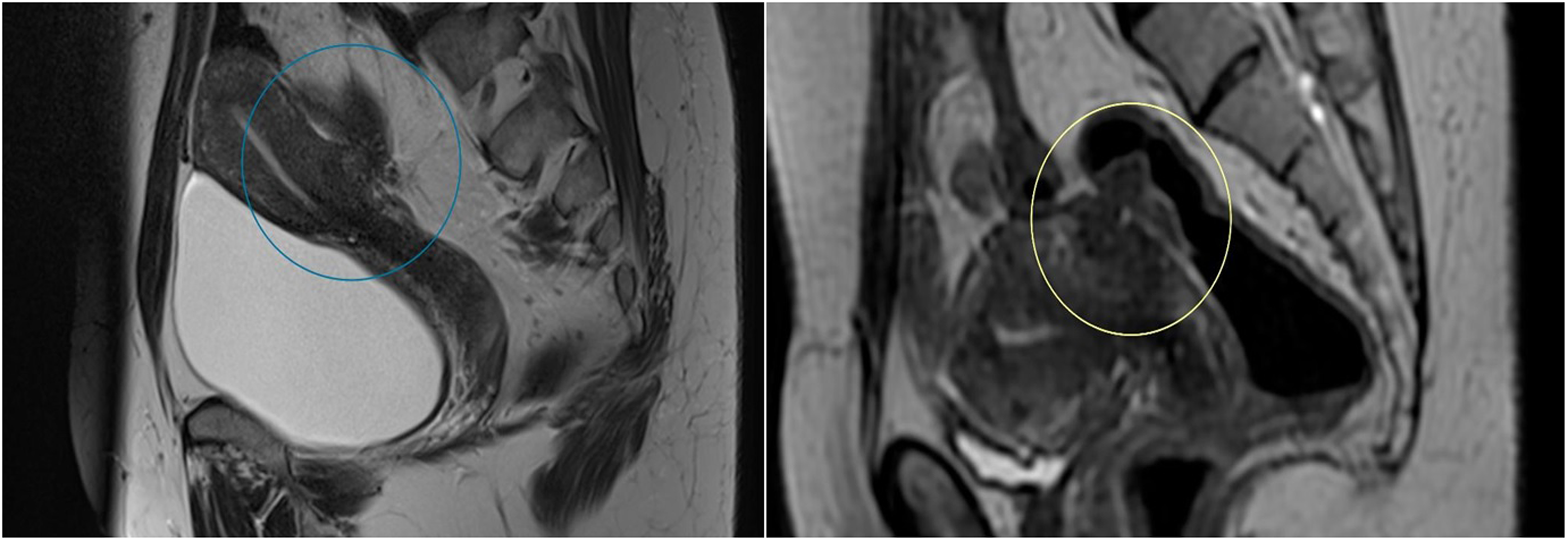
Two MRI saggital plane images showing deep endometriosis, between posterior uterine wall and rectum, involving rectal submucosa.
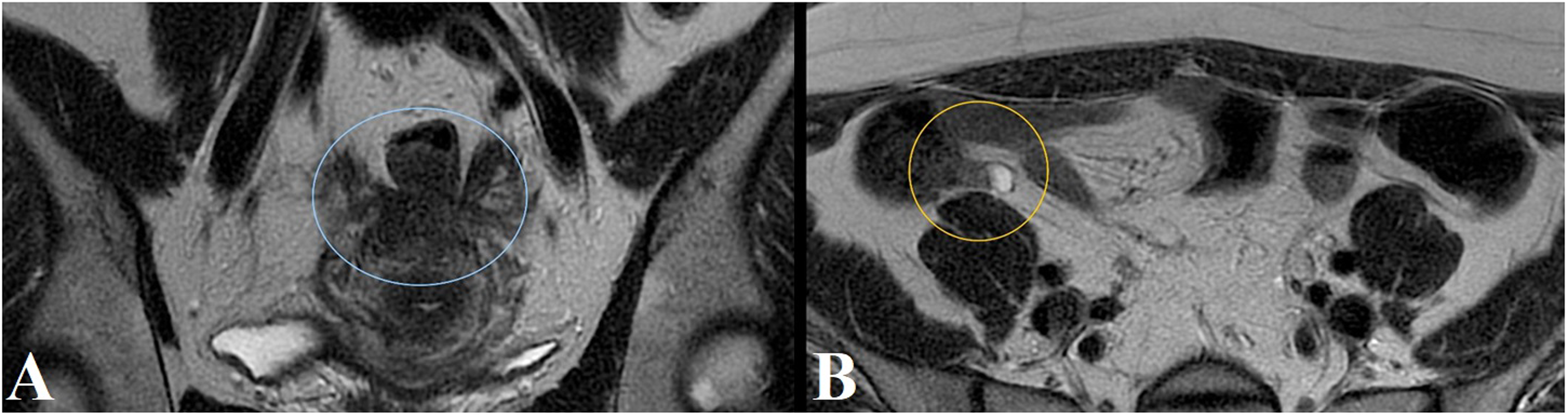
(A) MRI coronal plane showing deep endometriosis, that involves rectum and both ovaries. (B) MRI coronal plane – grossly normal appearance of the appendix.
As a result, on the third day of the admission, laparotomy was performed. As expected, intraoperative, multiple adhesions were observed and thorough adhesiolysis was done. Moreover, en bloc low rectal resection with total hysterectomy and bilateral adnexectomy (Figure 3) was performed due to the presence of bilateral adnexial masses, with posterior wall uterine endometriosis that invaded medium and superior rectum and pelvic peritoneum. The restoration of intestinal continuity was done using a mechanical side-to-end colorectal anastomosis. Appendectomy was also performed.
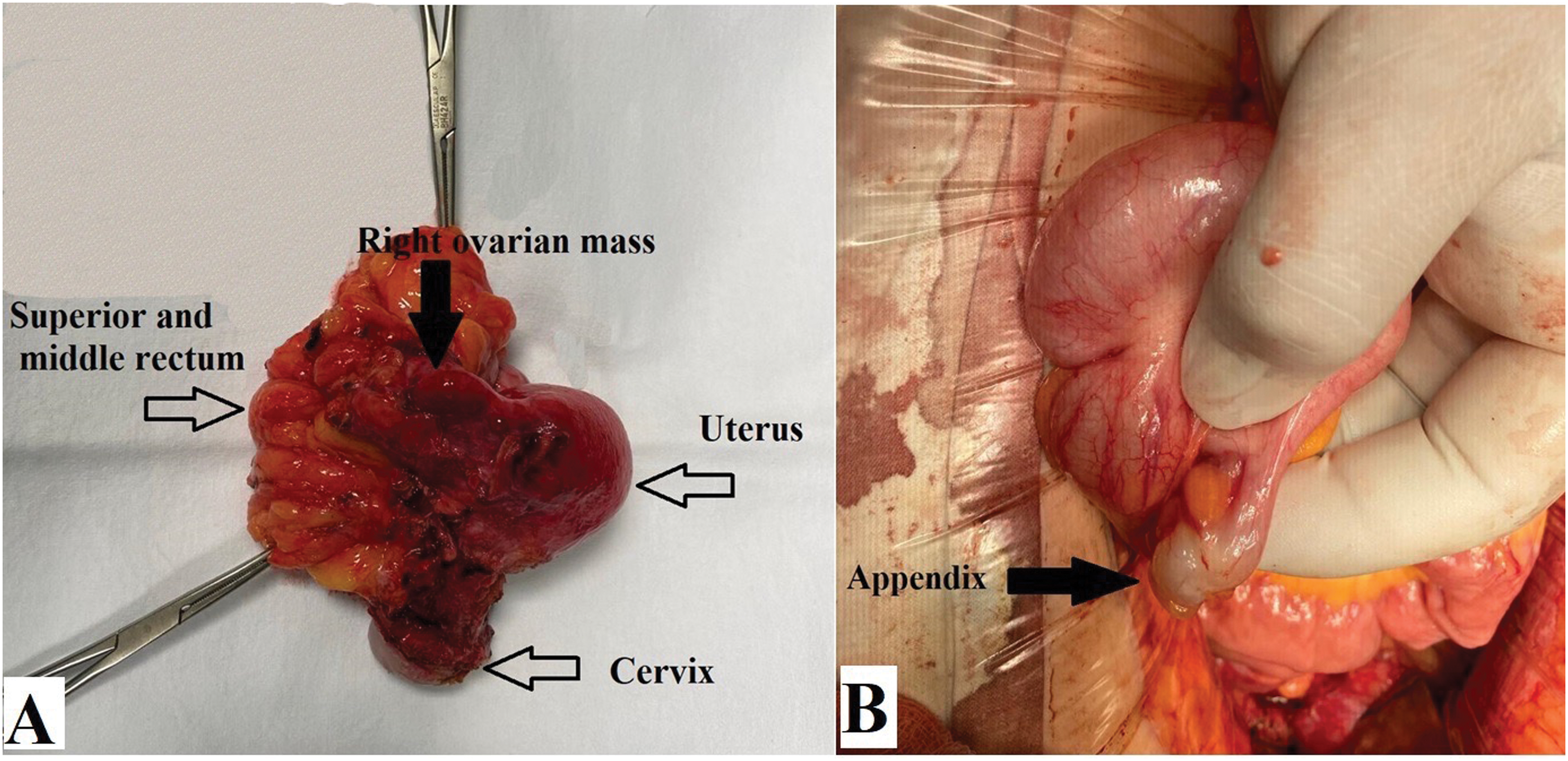
(A) En bloc low rectum resection with total hysterectomy and bilateral adnexectomy. (B) Intraoperative appearance of the appendix.
The radical hysterectomy with bilateral salpingo-oophorectomy specimen, along with the adjacent segment of rectum and appendix, were sent to the laboratory for histological examination. On macroscopic examination, the main surgical specimen showed an area of adhesion between the posterior wall of the uterus and the rectum of 2.5 cm in diameter with cystic spaces on the cut surface. The appendix had a particular aspect measuring only 2 cm in length and 1 cm in diameter, with dilatation of the tip. The lumen was slightly distorted by mucus material, with no evidence of hemorrhage.
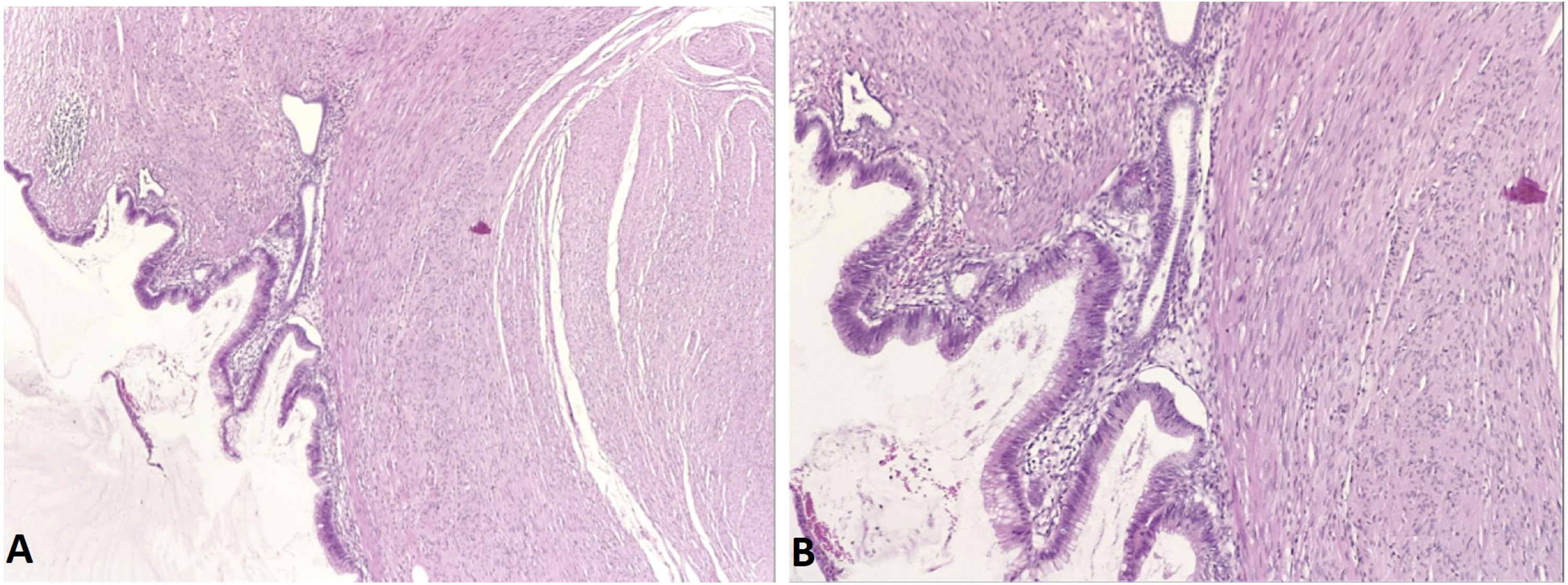
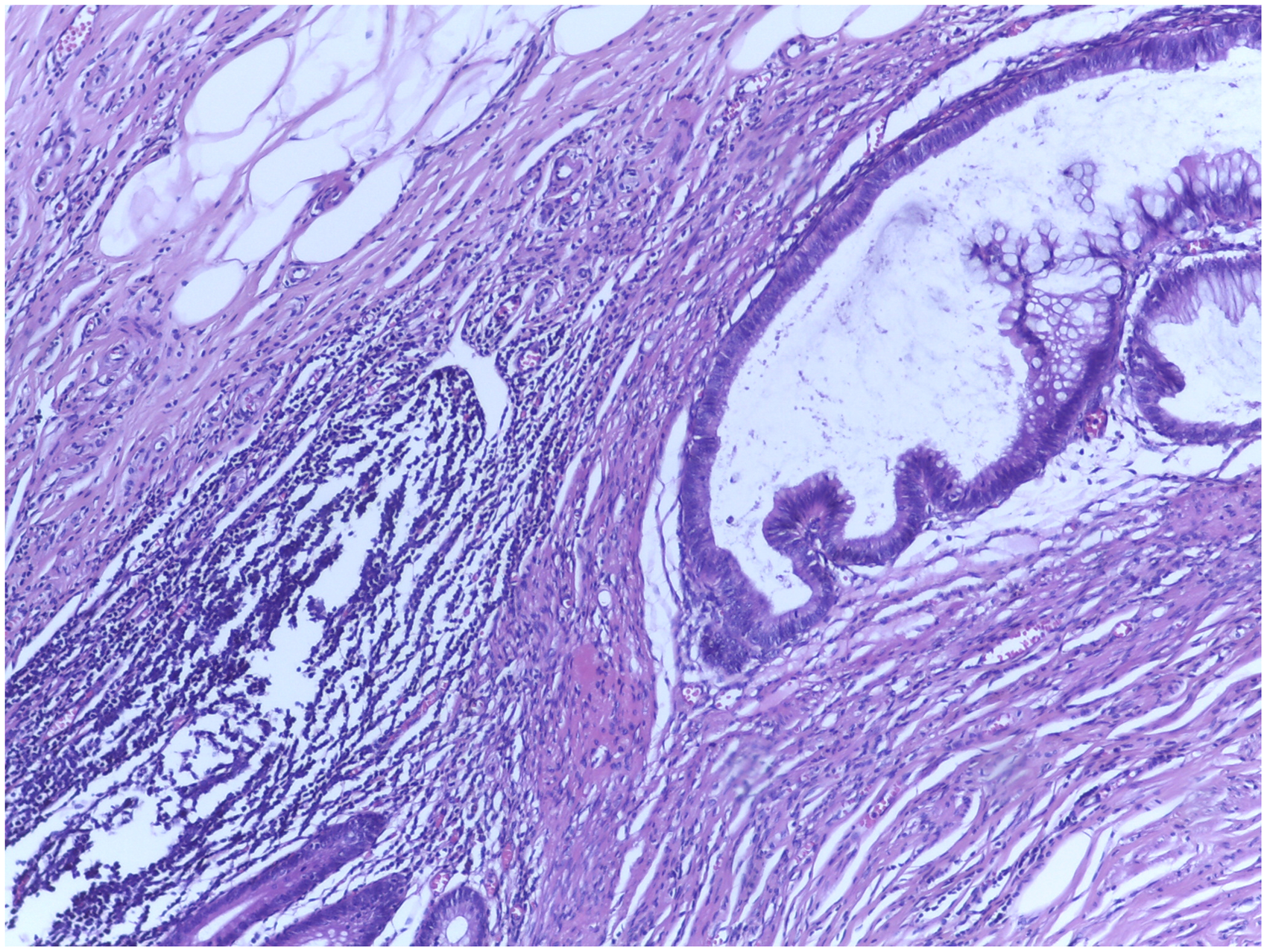
Under light microscopic examination, the rectum showed extensive areas of endometriosis localized from the muscular wall to the serosa and in close continuity with foci of uterine adenomyosis. Areas of endometriosis were also identified in both ovaries. The appendix wall revealed many endometriotic foci, consisting of endometrial glands embedded in varying amounts of endometrial stroma, located at various levels, from the serosal layer to the submucosal layer, in close proximity to the mucosa (Figure 4). Some of the glandular structures embedded in the endometrial stroma were bordered by mucinous-type epithelium containing intestinal cells, Goblet cells, and Paneth cells. These metaplastic endometrial glands were found only in the mucosal and submucosal layers of the appendiceal wall and not involving the serosa. Transition zones between the endometrial-type epithelium and purely mucinous epithelium were identified in the mucosal epithelial lining near the lumen as shown in Figure 5A and 5B. However, mucus-filled microcysts were discovered in the muscular layer (Figure 6). In fact, these structures consist of pools of mucin, only partially delineated by a flat, round, atrophic epithelium and surrounded by CD10 positive endometrial-type stroma. It is important to mention that intestinal metaplasia was not identified in any other organ of this patient in which endometriotic tissue was found. There were no dysplastic changes or other notable alterations in the appendiceal mucosa. The endometriotic origin of the glands and stroma, as well as the metaplastic character of the intestinal-type epithelium observed in some of these foci, were verified by immunohistochemistry (IHC) on the paraffin-embedded appendiceal tissue. KRT7 expression was found in the endometrial epithelium, in contrast with the negative stain in the normal appendix mucosa and in the intestinal-type metaplastic epithelium. Both the normal appendiceal mucosa and the intestinal-type metaplastic epithelium of the glandular structures were positive for KRT20 (Figure 7). KRT20 was not expressed in the endometrial-type epithelium that lined the glands. The endometrial stroma enclosing endometrial glands, as well as the stroma surrounding mucinous-type metaplastic epithelium, were positive for CD10, estrogen receptor (ER), and progesterone receptor (PR) as shown in Figure 8.
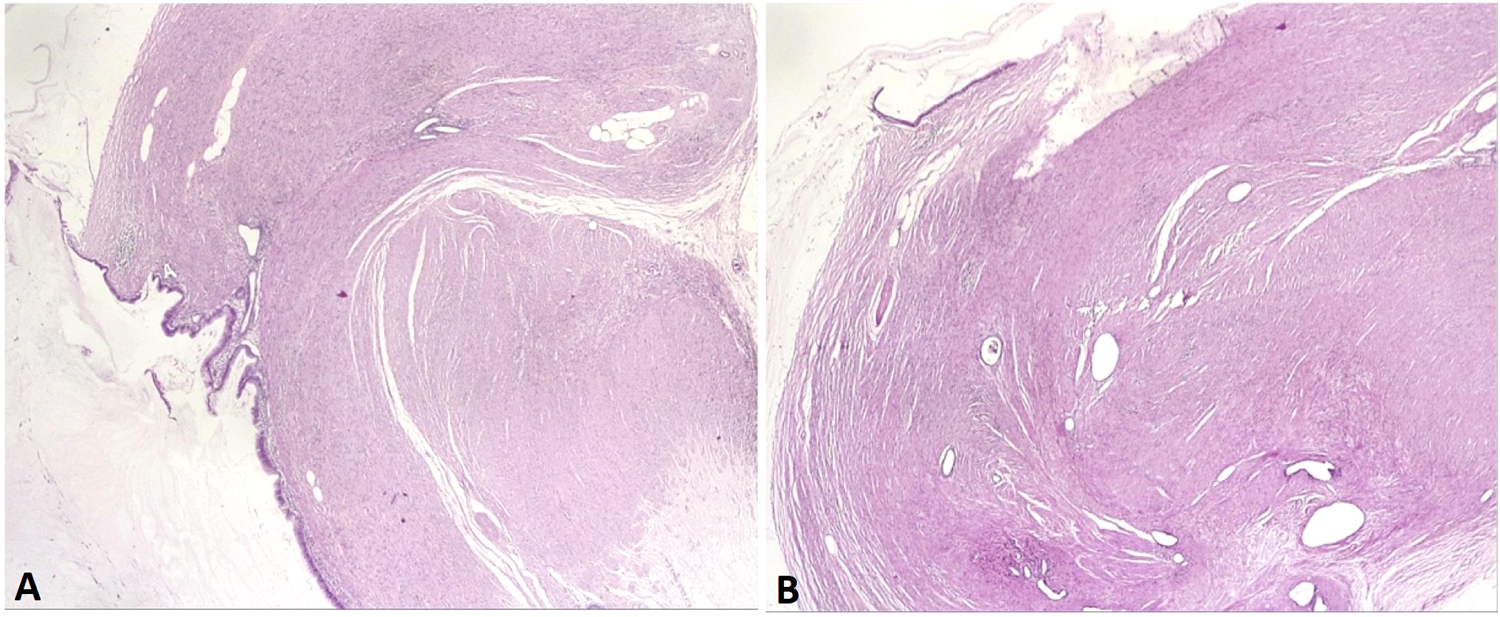
Foci of endometrial glands and stroma scattered throughout the appendix wall, HE staining, low-power field (A) and (B).
Mucosa of the appendix - transitional areas with endometrial type-epithelium admixed with tall columnar mucinous epithelium, HE staining, medium-power field (A) and high-power field (B).
Mucus-filled microcysts (top left) and endometrial gland with focal intestinal metaplasia, HE staining, medium-power field.
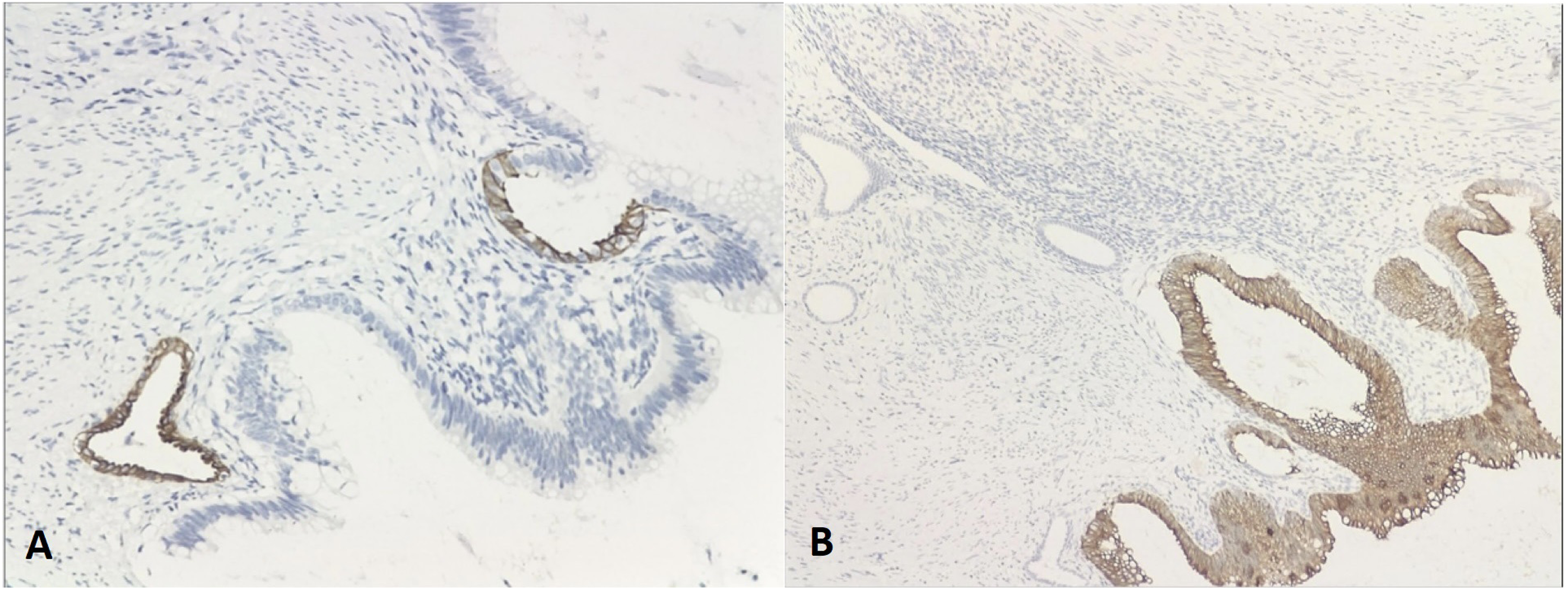
(A) KRT7 positive stain of endometrial-type epithelium in superficial transitional mucosa high-power field; (B) KRT20 positive stain of columnar mucinousepithelium in the same transitional mucosa, high-power field.
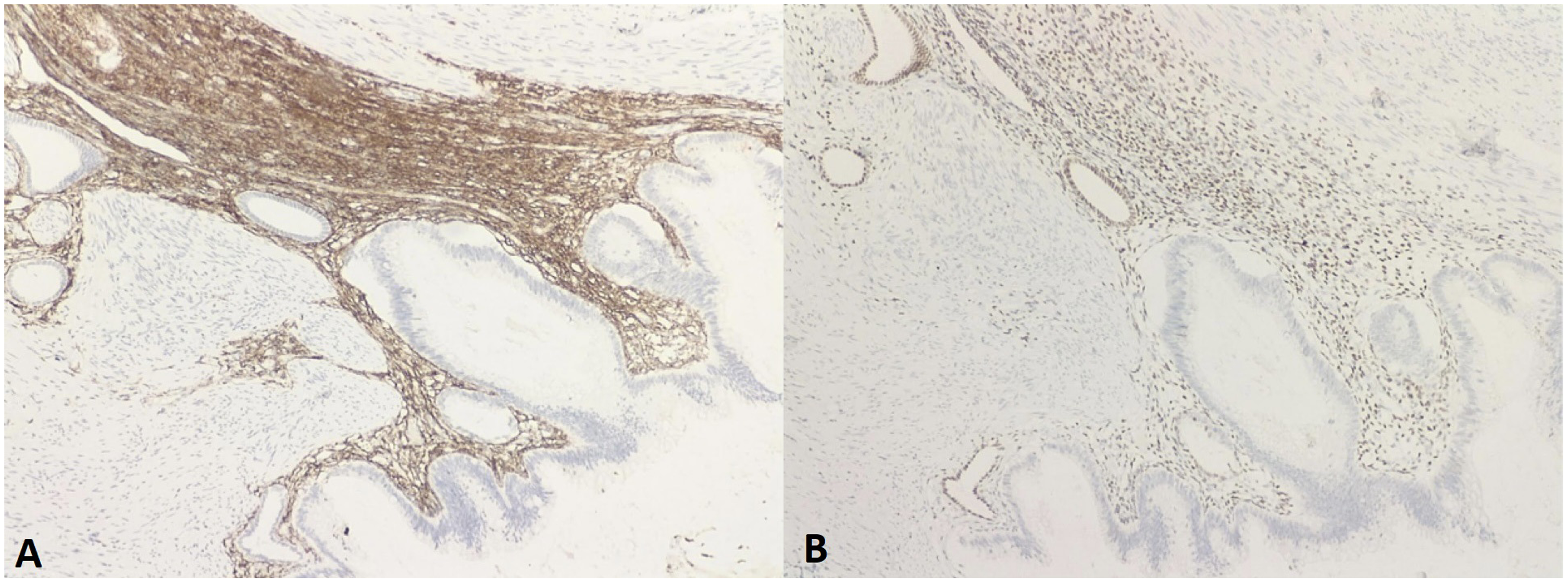
(A) CD10 positive stain in endometrial stroma surrounding glands, high-power field; (B) ER positive stain in endometrial glands and stroma, high-power field.
Discussions
The presence of ectopic endometrial glands and stroma outside of the uterine cavity is defined as endometriosis. Endometriosis in extrauterine sites is thought to be caused by a variety of factors.9,10 The most widely accepted explanation is retrograde menstruation, which states that endometrial tissue is transferred from the uterus through the fallopian tubes backwards. 9 Another viable theory is coelomic metaplasia, which refers to peritoneal cavity stem progenitor cells that can develop into endometrial cells.9,10 Furthermore, the notion of direct transplantation and dissemination could explain endometriosis occurring in extra-pelvic locations. 9
The most common localization for extrauterine endometriosis is represented by the ovary, but it can be also identified in other parts of the human body, including the intestinal tract. 2 Endometriosis localized in the wall of the appendix is rare and was first described by Karl F. Von Rokitansky. 4 It may be asymptomatic or present as acute abdominal pain, with nausea and vomiting, intestinal perforation, intussusception or gastrointestinal bleeding.1,3,5,6,9 Other patients have a long history of chronic pelvic pain. 11
The occurrence of appendiceal endometriosis, as well as significant areas of intestinal metaplasia in several of the endometrium-type glands, defines the case of our patient. This is a very uncommon occurrence, with just a few cases recorded in the literature, and it could be mistaken for a mucinous tumor by a novice eye.8,12–15
It is well known that endometriosis can undergo variable metaplastic changes, with endocervical-type metaplasia being the most commonly described. Other documented types of metaplasia include squamous, ciliated, hobnail, eosinophilic or intestinal-type metaplasia.13,16 Intestinal metaplasia of the endometrial tissue consists of mucinous columnar cells, Goblet cells and Paneth cells partly replacing the endometrial epithelium-lining.
Six examples of endometriosis in the cecum and appendix with foci of intestinal metaplasia that simulated mucinous neoplasms macroscopically and histologically were recently described in a well-researched paper. 8 Epithelial dysplasia was not discovered. There were scattered Paneth cells in one patient who had a history of endometriosis. 8 Furthermore, an incidental observation in a patient with an appendiceal mucinous tumor was endometriosis with focally intestinal metaplasia with Paneth cells. 12 Other two examples13,14 described the coexistence of appendiceal endometriosis with intestinal metaplasia, including Paneth cells and low-grade mucinous epithelial dysplastic alterations. Moreover, a study report of a patient with endometriosis involving the cecum emphasizes the importance of recognition of the intestinal metaplastic epithelium with Paneth cells as it may potentially mimic an invasive mucinous carcinoma. 15
Despite its rarity, endometriosis of the appendix with foci of intestinal metaplasia can sometimes be confused with low grade appendiceal neoplasm (LAMN), especially because both entities can cause extrusion of mucus on the appendiceal serosa. 17 Low-grade appendiceal neoplasm is characterized by its low-grade epithelial features and lack of infiltrative growth. It can perforate the appendix, and disseminate into the peritoneal cavity in the form of pseudomyxoma peritonei. 17
The pathogenesis of intestinal-type transformation of endometriosis is still a subject of debate. Two theories have been proposed: metaplasia and colonization.8,18 These theories have been debated in a comprehensive report by J. Misdraji et al in 2014. 8 In particular cases, some helpful features can establish a correct diagnosis. The absence of an intraluminal mucinous neoplasm is a strong argument against the possibility that mucinous areas of the endometriosis might represent direct colonization of the endometriosis glandular structures by mucinous epithelial cells from a mucin producing tumor. Moreover, no dysplastic changes were found in the appendiceal mucosa. Furthermore, we identified transition zones between the endometrial-type glands and purely mucinous glands with an admixture of endometrial, Goblet, columnar and Paneth cells. In contrast, a sharp demarcation between appendiceal glands and endometrial glands it would be expected in the situation of colonization. Additionally, the presence of endometrial-stroma surrounding the intestinal type glands was illustrated by IHC markers CD10, ER receptor and PR receptor. Estrogen and progesterone receptors showed positivity in mucinous metaplastic cells, although they were negative in the normal mucosa of the appendix. Based on these arguments, our case is more likely to represent a true metaplastic process in areas of appendiceal endometriosis.
Conclusion
In conclusion, we have presented a patient with appendiceal endometriosis accompanied by significant intestinal metaplasia on background of extensive endometriosis in rectum and ovaries. This unusual finding has the potential to mimic more serious conditions, both clinically and histologically and adding another case to the literature will help to raise awareness in order to achieve better recognition of this entity.
Footnotes
Acknowledgements
None.
Author Contributions
Florin Grama, Daniel Cristian, Ileana Popa and Gabriel Becheanu – concept and design of the article. Mirela Chitul, Madalina Chivu and Andrei Chitul – collecting the data and writing the article. Ileana Popa and Gabriel Becheanu – acquisition of pathology images. Florin Grama- review of article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
N/A
Informed Consent
N/A
Trial Registration
N/A