
Abstract
Introduction. Primary leiomyosarcoma of bone is rarely described in the literature. In young patients, the clinical and radiological features may mimic relatively common tumours like osteosarcoma. Vertebral and nodal metastasis from osseous leiomyosarcoma is extremely uncommon. Case presentation. A 25-year-old female presented with progressively increasing pain and swelling of the right knee. Clinical and radiological features were suggestive of osteosarcoma. Pre-operative biopsy showed a malignant spindle cell tumour. The surgical resection specimen showed features of leiomyosarcoma of the right proximal tibia. On further evaluation, the patient was found to have an L3-L4 vertebral lesion and histopathological evaluation showed a similar tumour. After 11 months of initial presentation, the patient had axillary lymph node metastasis. Conclusion. Primary osseous leiomyosarcoma should be considered as a differential diagnosis even in young patients presenting with meta-diaphyseal expansile malignant bony lesions. Histology and ancillary studies can confirm the diagnosis.
Introduction
Leiomyosarcoma is a common malignant mesenchymal neoplasm showing smooth muscle differentiation. It commonly arises in the uterus, retroperitoneum and deep soft tissue of extremities. Primary leiomyosarcoma of bone is a rare, however well-recognised entity. 1 The histology, immunohistochemistry (IHC) and molecular features of primary leiomyosarcoma of bone are similar to its soft tissue counterpart. Here we describe a rare case of primary leiomyosarcoma of bone in a young patient with vertebral and nodal metastases. The extreme rarity and pre-operative diagnostic challenge involved in this case make it unique.
Case Presentation
A 25-year-old female presented to the orthopaedics outpatient department with complaints of gradually increasing swelling in the right knee, which was associated with dull aching pain. There was no prior history of trauma or any contributory past medical or family history. A radiograph of the right knee showed an ill-defined lytic lesion with cortical breach and a wide zone of transition in the proximal tibial metaphysis (Figure 1). Magnetic resonance imaging (MRI) scan showed a heterogeneous lesion with few haemorrhagic foci in the right proximal tibial metadiaphysis measuring 7.6 × 4.4 × 2.3 cm with cortical breach and a circumferential exophytic soft tissue component extending into anterior and posterior compartments. The lesion extended proximally up to the subarticular cartilage of the tibial condyles (Figure 2). Based on the clinical and imaging findings, a diagnosis of osteosarcoma was considered. The core needle biopsy showed features of a malignant spindle cell lesion and a possibility of the fibroblastic variant of osteosarcoma was considered. For further staging of the osteosarcoma, whole-body Fluoro-deoxy glucose positron emission tomography (PET) was performed which revealed a metastatic lesion in the L3 vertebral body apart from the primary lesion of the proximal tibia. Based on these findings, a final diagnosis of metastatic osteosarcoma was made. According to our institutional protocol, the patient received three cycles of cisplatin-based neoadjuvant chemotherapy followed by reassessment of local and metastatic disease with repeat MRI and PET scan. The imaging revealed static disease without resolution or progression and no new metastatic lesion. After thorough counselling, the patient opted for a limb salvage surgery of the proximal tibia along with spondylectomy of the L3 vertebral body. The patient underwent a staged procedure of spondylectomy with spine instrumentation followed by limb salvage surgery with wide local resection of the proximal tibia and endoprosthesis implantation. The postoperative course was uneventful. Both the surgical specimens were sent for histopathology evaluation.
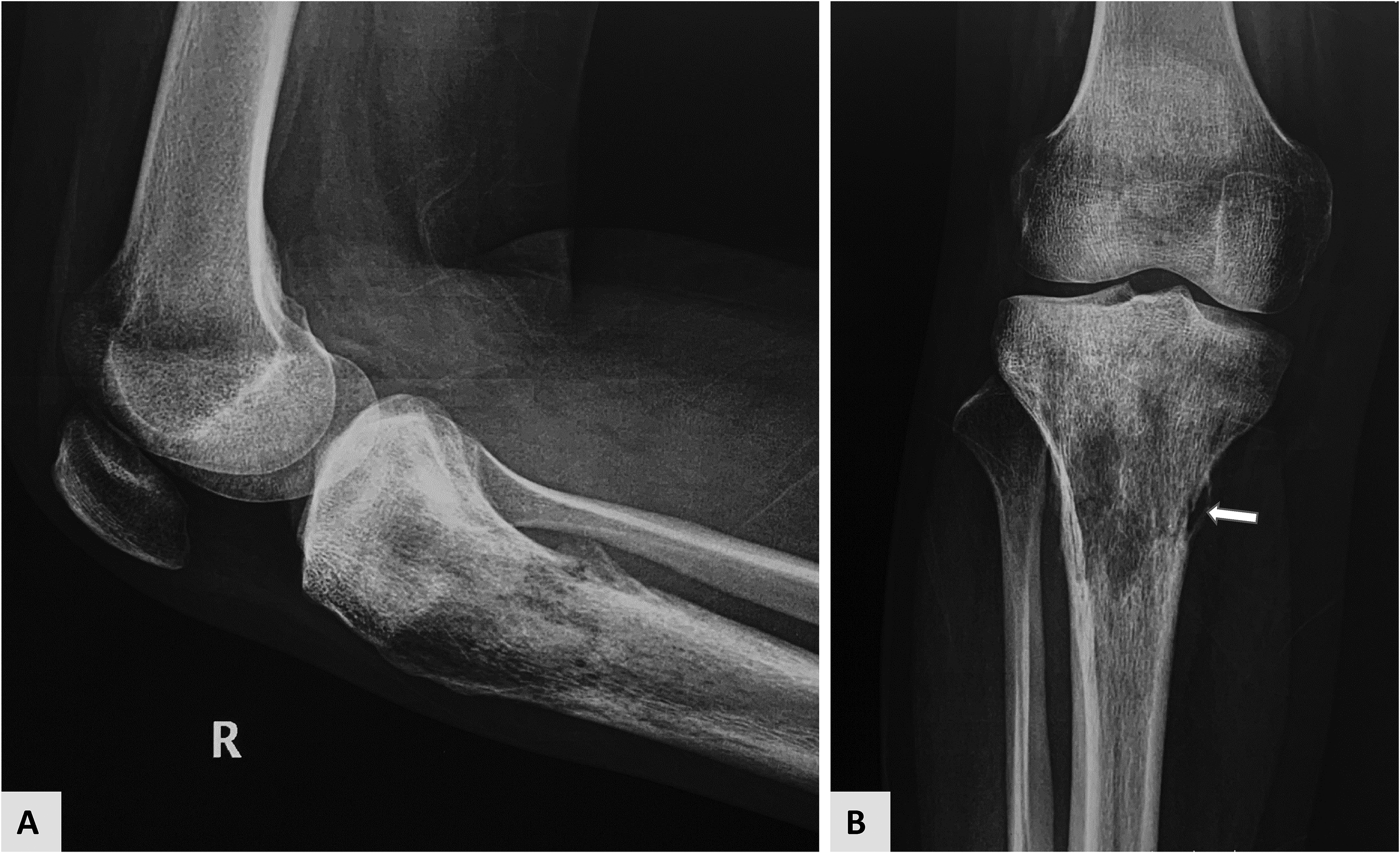
(A, B) Radiograph of the right knee showed a permeative lytic lesion involving proximal metaphysis of the tibia with a wide zone of transition and breach of medial cortex with elevated periosteum (arrow). There is no matrix mineralisation.

(A, B) Coronal T2-weighted fat-saturated MRI (A) and T1 weighted coronal image of the right leg showed an exophytic heterogeneous soft tissue component of the mass arising from the tibia with areas of haemorrhage within (arrow). The lesion extended to involve subarticular marrow (small arrow). The lesion was isointense to muscle on the T1-weighted image (B). Few curvilinear flow voids were seen (curved arrows).
Pathological Findings
On gross examination, the tumour was solid, grey-white homogeneous and fleshy. It involved the meta-diaphysis as well as the epiphysis of the proximal tibia. The tumour was infiltrating the medullary cavity. Less than 10% tumour area showed necrosis. The articular surface was abutted by the tumour, which was also infiltrating the adjacent soft tissue. Foci of haemorrhage were noted (Figure 3).

Gross photograph of the resected specimen. The tumour was solid, grey-brown, fleshy, located in the proximal epi-metaphysis of the tibia and was breaching the cortex and infiltrating into the surrounding soft tissue and articular cartilage.
Microscopic examination of the resected specimen showed a cellular mesenchymal tumour in intersecting fascicle and herring-bone pattern. The tumour was seen infiltrating the marrow spaces (Figure 4A, B). Tumour cells showed moderate to marked nuclear pleomorphism, had hyperchromatic nuclei, and scant spindled cytoplasm. Frequent mitoses were noted [∼14-15/10 high power field]. Only approximately 10% of the tumour area showed features of therapy-related changes in the form of sclerosis and necrosis (Figure 4C, D). Mild lymphoplasmacytic infiltrate was also noted in the surrounding stroma. No malignant osteoid was noted even on extensive sampling.

(A, B, C) [H&E, 10× magnification]. Tumour cells were arranged in sweeping fascicles (A). The tumour cells were seen infiltrating through the marrow spaces (B). A small focus of tumour necrosis. (C and D) Individual tumour cells showed moderate to marked nuclear pleomorphism, had cigar-shaped nuclei with blunt ends, coarse chromatin, occasional conspicuous nucleoli and scant eosinophilic cytoplasm. Mitotic figures were frequent (arrow) [H&E, 40× magnification].
On IHC, these tumour cells were strongly and diffusely positive for vimentin, smooth muscle actin (SMA) and focally for h-caldesmon (Figure 5). IHC for pan-keratin, epithelial membrane antigen, desmin, MYOD1, TLE1, CD34, SATB2, S100 and ALK were negative. There was no loss of nuclear immunostaining for H3K27me3. Epstein Barr virus in-situ hybridization (EBER-ISH) was negative. Based on the morphology and IHC, a final diagnosis of leiomyosarcoma of bone (FNCLCC grade 2) was established.

Using immunohistochemistry, tumour cells show strong, diffuse cytoplasmic positivity for vimentin (A), smooth muscle actin (B) and h-caldesmon (C). Ki-67 labelling index was approx. 10-15% (D).
Sections examined from the excised L3 vertebra showed a similar tumour morphology. The tumour cells stained positive for SMA.
The pre-operative core needle biopsy was also reviewed. The tissue was of limited quantity and showed spindle-shaped tumour cells of similar morphology. There was no neoplastic osteoid tissue in the preoperative biopsy sample. However, IHC could not be performed during preoperative evaluation or during review due to scant material in the biopsy sample.
Follow Up Information
A thorough investigation including clinical examination, MRI and PET scan was done after the diagnosis of leiomyosarcoma of bone was established. No primary lesion was identified anywhere in the genital tract or in the soft tissue. The patient was kept on close follow-up. Eleven months after the surgery, the patient presented with a firm to hard lymph node in the right axilla. The patient underwent a PET scan which confirmed a single site of metastasis. The lymph node was excised. Histologic examination and IHC confirmed metastatic leiomyosarcoma. A follow-up PET scan 2 months later revealed widespread metastasis for which the patient was scheduled for a further course of chemotherapy.
Discussion
The first case of primary leiomyosarcoma of bone in English literature was published by Evans and Sanerkin. 2 primary leiomyosarcoma of bone arising in the extragnathic bone has been described mostly in the form of isolated reports or small case-series. Adelani et al reviewed 107 skeletal leiomyosarcomas that had been previously reported in the English literature. 3 Age of presentation varied from 9- to 87-years with a median age of 47 years, which is younger than its soft tissue counterpart. 4 Males and females were almost equally affected. The commonest site was the distal femur (29%), followed by the proximal tibia (26%). Most of the leiomyosarcomas arising in the long bones involved the metaphysis with or without an extension to the epiphysis, diaphysis, or surrounding soft tissue. Potential risk factors, including radiation, chemotherapy, Pagets disease of the bone, and orthopaedic implant, were identified in 10% of the cases. Immunocompromised patients may develop smooth muscle tumours associated with Epstein Barr virus (EBV) infections in several organs, which are designated as EBV-associated smooth muscle tumours and may rarely involve the bone. 5 Our patient did not have any prior history of radiation, trauma or organ transplantation to suggest immunocompromised status.
In a series by Antonescu et al 1 33 leiomyosarcomas of the bone were classified into 26 high grade and 7 low-grade tumours by an assessment of their histologic parameters, including the degree of cellularity, cellular pleomorphism or anaplasia, mitotic activity, degree of necrosis, and invasive growth.
High-grade leiomyosarcomas show ill-defined, irregular osteolytic lesions with a moth-eaten or permeative pattern of osseous destruction radiographically, and diffuse involvement and destruction of the medullary bone histologically. On the other hand, the low-grade tumours exhibited diffuse involvement of the marrow spaces and had radiographic features, including a geographic pattern of bone destruction and a sclerotic rim. Intraregional calcification is not a typical feature of primary leiomyosarcoma of bone, however, as many as 20% of the patients showed foci of calcification and mimicked osteosarcoma on imaging. 6
Our case showed radiographic and histological features of a high-grade tumour. High-grade primary leiomyosarcoma of bone also shows less disease-free survival and a higher rate of distant metastasis. A review by Adelani et al 3 showed as many as 57% of the cases with distant metastasis, the most common site being the lung. Axial skeletal metastasis is relatively rare. To the best of our knowledge, no case of lymph node metastases from primary leiomyosarcoma of bone has been reported to date.
primary leiomyosarcoma of bone is difficult to diagnose, primarily because of its rarity. A thorough work-up is recommended for possible metastasis from soft tissue or other common locations before labelling a case as primary leiomyosarcoma. The histological differential diagnoses of leiomyosarcoma of the bone may differ according to the tumour grade. The differential diagnoses of high-grade lesions usually include fibrosarcoma, fibroblastic osteosarcoma, malignant fibrous histiocytoma of the bone, synovial sarcoma and metastatic sarcomatoid carcinoma etc The presence of neoplastic osteoid in the tissue confirms the diagnosis of osteosarcoma. However, the neoplastic osteoid is often not adequately sampled in the preoperative biopsy, hence the differentiation of the fibroblastic variant of osteosarcoma becomes difficult. An IHC panel that includes markers like SMA, desmin, h-caldesmon can be added to the panel. Fibrosarcoma would be a diagnosis of exclusion after ruling out the other possible diagnosis.
The histogenetic origin of this neoplasm is not clear. It is hypothesized to arise from intraosseous blood vessels, pluripotent mesenchymal stem cells, stromal cells, or an intermediate or incomplete smooth muscle phenotype, such as myofibroblasts.1, 7, 8 It has been reported that leiomyosarcomas that originate from blood vessels frequently exhibit diffusely positive immunoreaction to h-caldesmon with a potentially limited expression of desmin, although the expression of both desmin and h-caldesmon is usually correlated with the degree of smooth muscle differentiation in leiomyosarcomas of non-vascular type. 9
Data on optimal treatment and prognostic factors for primary leiomyosarcoma of bone are limited because of its low prevalence. Surgical resection, when possible, remains the primary treatment modality. Unlike primary osteosarcoma, which is generally chemosensitive, multiple studies have reported poor response of primary leiomyosarcoma of bone to chemotherapy, as well as minimal impact on overall survival benefit.10, 11
Conclusion
Leiomyosarcoma of bone is a rare but well-recognized primary osseous sarcoma that may arise de novo or in association with radiation. The sarcoma is typically a high-grade tumour with poor survival outcomes and limited treatment options, particularly in metastatic cases. Although the diagnostic differential is broad, awareness of this rare bone tumour phenotype and knowledge of its key morphological and immunohistochemical features allow for accurate diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Informed consent was obtained from the patient. Patient's anonymity was maintained.
Informed Consent
Written informed consent was obtained from the patient to publish the image.
Trial Registration
Not applicable, because this article does not contain any clinical trials.