
Abstract
A subset of clear cell chondrosarcomas may contain focal areas of low-grade conventional chondrosarcoma; however, it is rare to find foci resembling clear cell chondrosarcoma admixed with areas otherwise typical conventional chondrosarcoma. We report two patients with conventional chondrosarcoma with clear cell features occurring in the rib, one in the setting of multiple hereditary exostoses (MHE) and the other without MHE. Both patients were found to have a destructive rib mass with a soft tissue component and underwent en bloc resection. Histologic examination revealed predominantly grade 2 conventional chondrosarcomas; however, multiple foci containing large cells with pale eosinophilic to clear cytoplasm, distinct cell borders, centrally located nuclei, and conspicuous nucleoli, resembling clear cell chondrosarcoma were identified throughout the specimen. The significance of clear cell features in an otherwise typical conventional chondrosarcoma, to our knowledge, is unknown and deserves recognition. Finally, these tumors highlight the need for careful histologic examination and proper classification as unexpected findings may impact management.
Keywords
Introduction
Clear cell chondrosarcoma is a rare, low-grade chondrosarcoma subtype typically occurring in the epiphysis of long bones in older adults in their third to fifth decades of life. The tumor consists of lobules or sheets of neoplastic cells with abundant clear, pale to eosinophilic cytoplasm, distinct cell borders, large round central nuclei, and conspicuous nucleoli. Evenly distributed woven bone formation with admixed osteoclast-like giant cells is often observed. Foci of conventional chondrosarcoma may be seen in clear cell chondrosarcoma in about half of the tumors1,2; however, it is very unusual to find areas morphologically resembling clear cell chondrosarcoma in an otherwise classic conventional chondrosarcoma. To date, there have been only two reports including six patients with conventional chondrosarcoma with a clear cell component.3,4 Herein, we present two patients – one with a known diagnosis of multiple hereditary exostoses (MHE) and the other without MHE.
Case Reports
Case 1
A 61-year-old man with a known diagnosis of MHE presented with a new pain over his left ribcage. He had multiple osteochondromas, including those in the right iliac wing, right forearm, left ankle, and bilateral knees. Radiographs demonstrated a subtle expansile deformity of his left ninth rib. A subsequent chest CT showed an exophytic mass along the left lateral ninth rib with an associated soft tissue mass (6 × 5.5 cm) suspicious for transformation to chondrosarcoma given an irregular amorphous internal calcified matrix along with a soft tissue component (Figure 1A). Multiple exostoses in the ribs were also noted. There was no prior CT for comparison, but given that the mass was not previously palpable, it was likely that it had grown over the prior few months. Tc-99m MDP whole body scan demonstrated focal radiotracer activity within the lateral aspect of the left ninth rib. Given the patient's history of MHE and the high likelihood of chondrosarcoma, the patient underwent a wide excision of his rib mass.
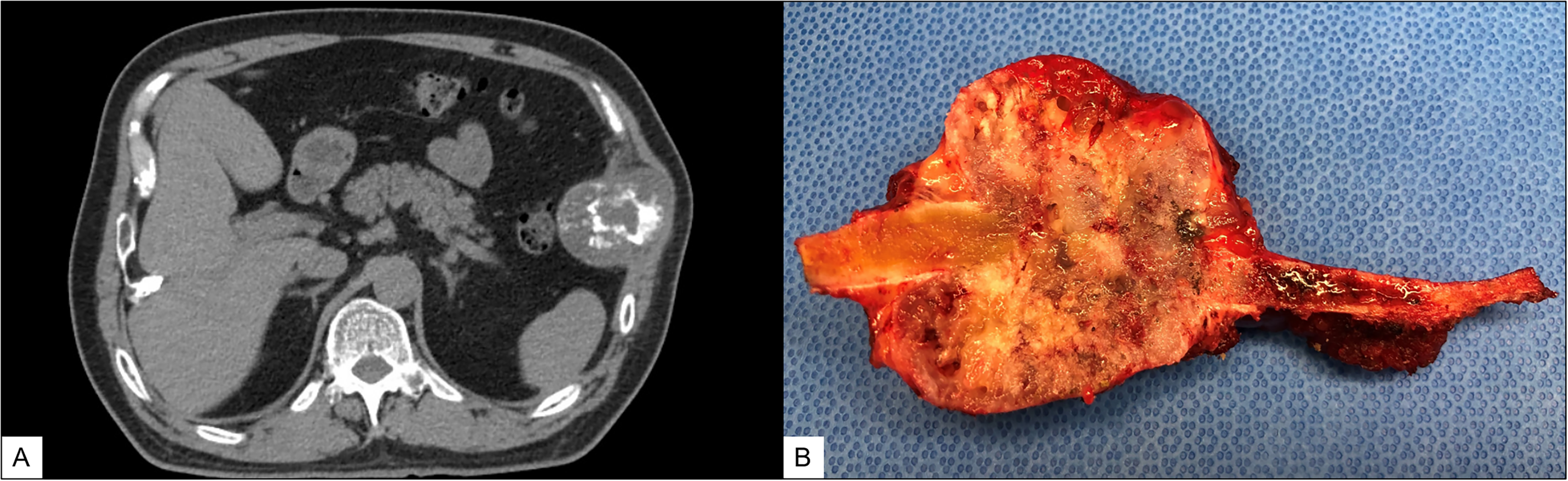
(Case 1): Axial computed tomography (CT) shows a mass along the ninth left lateral rib with associated soft tissue mass (A). An irregular amorphous internal calcified matrix along with a soft tissue component are suspicious for the transformation of osteochondroma to chondrosarcoma. Gross evaluation reveals a destructive 6.4 cm mass encasing a portion of the rib. The section reveals a white-tan heterogeneous cartilaginous cut surface with bone involvement (B). The osteochondroma stalk is not definitively identified.
Gross examination showed a 6.4 × 5.0 × 4.3 cm mass encasing a portion of the rib, with a smooth capsule around the lesion. The specimen is serially sectioned to reveal a white-tan heterogeneous cartilaginous cut surface destroying the native bone without an underlying osteochondroma stalk (Figure 1B). Microscopic examination revealed predominantly grade 2 conventional chondrosarcoma showing hypercellularity, permeative growth, and myxoid stroma (Figure 2A). The tumor cells were plump and demonstrated nuclear atypia with enlarged nuclei, open chromatin, and conspicuous nucleoli (Figure 2B). However, multiple scattered foci of clear cell features were also identified throughout, accounting for 20% of the overall tumor (Figure 2C). In these areas, the tumor cells demonstrated pale eosinophilic to somewhat clear cytoplasm with central nuclei and prominent cell borders (Figure 2D). Both components showed gradual merging with no abrupt transition. Based on these findings, the diagnosis of grade 2 conventional chondrosarcoma with foci of clear cell features was made. At a 14-month follow-up, the patient did well with no signs of clinical or radiological recurrence.

(Case 1): At low power, the tumor shows permeative growth pattern and consists of conventional chondrosarcoma with admixed clear cell change (A). The conventional component demonstrates increased cellularity, myxoid changes, and cytologic atypia, consistent with grade 2 chondrosarcoma (B). Both components show gradual merging with the clear cell component having woven bone formation (C). At high power, the clear cell component contains tumor cells that have abundant pale eosinophilic to clear cytoplasm with central nuclei and prominent cell borders (D).
Case 2
A 41-year-old man with an insignificant past medical history presented with an asymptomatic lytic lesion in the anterior portion of the left second rib incidentally discovered on a chest X-ray during his annual examination. A follow-up chest CT confirmed an intramedullary lytic lesion in the left second rib. The lesion was expansile, had scattered mineralized rings and arcs, and breached the cortex with a soft tissue component abutting the pleural surface, concerning for chondrosarcoma (Figure 3A). The patient underwent an en bloc resection of this second rib mass with disarticulation of the costosternal joint.
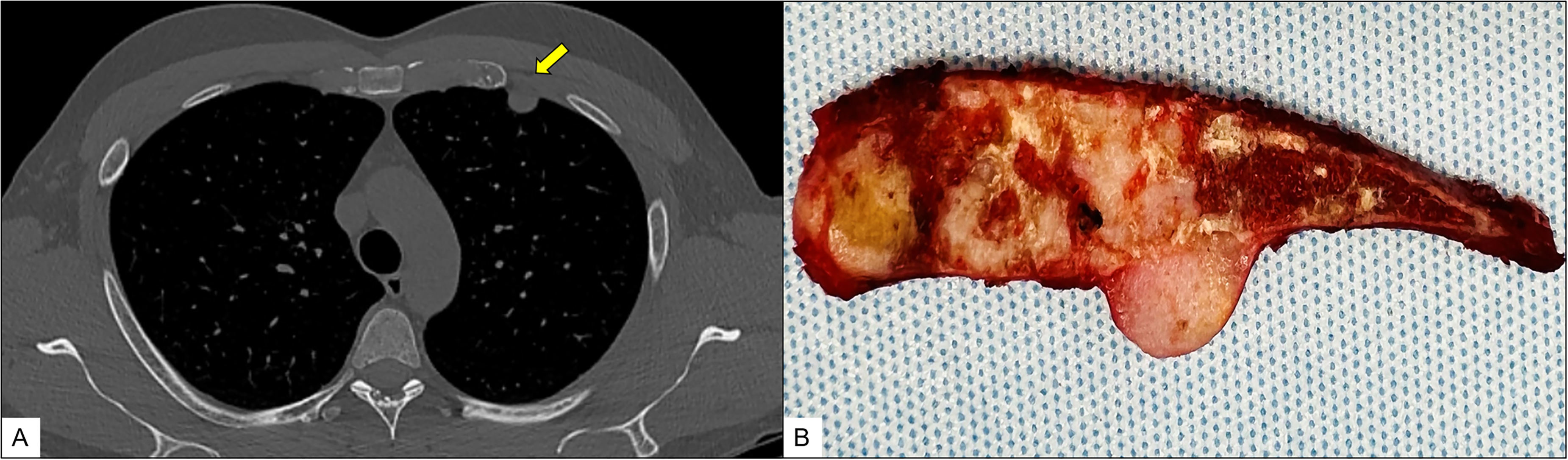
(Case 2): Axial computed tomography (CT) shows a mass arising in the second rib with a soft tissue component (A). Gross evaluation reveals a 3.8 cm left second rib mass showing both intramedullary and extraosseous exophytic components and consisting of glistening tan-white cartilaginous tissue (B).
Gross examination showed a mass protruding from the rib and partially covered by the intact pleura. Sectioning revealed a gray-tan, glistening, lobulated, cartilaginous lesion (3.8 × 2.1 × 1.7 cm) that filled the medullary cavity, broke the cortex, and formed an exophytic mass (Figure 3B). Histologic sections showed a hyaline cartilage neoplasm with mild to moderate hypercellularity and infiltrative growth. The tumor replaced the marrow and encased the pre-existing trabecular bone in a permeative and aggressive pattern (Figure 4A) of conventional chondrosarcoma grade 2 with scattered mitotic activity, increased cellularity, and cytologic atypia (Figure 4B). In addition, scattered foci, best seen in the extraosseous component of the tumor, composed of larger polygonal cells with lightly eosinophilic to pale cytoplasm, central nuclei, dot-like nucleoli, and prominent cell borders reminiscent of clear cell chondrosarcoma were also identified (Figure 4C-D). This clear cell change was mainly in the extra-osseous component, accounted for approximately 10% of the overall tumor mass, and gradually merged to the conventional component. Finally, woven bone admixed within the clear cell change was identified, a common finding in clear cell chondrosarcoma (Figure 4C). Therefore, the diagnosis of grade 2 conventional chondrosarcoma with focal clear cell features was rendered.

(Case 2): low-power microscopy reveals a predominantly low to intermediate grade conventional chondrosarcoma showing permeative growth throughout the intramedullary space of the rib as well as an exophytic soft tissue component. The pale areas, best appreciated in the extraosseous component, correspond to the clear cell change (A). The conventional component shows cytologic atypia; the nuclei vary in size and shape with open chromatin. Scattered mitotic activity is present (arrow) (B). Intermediate power shows an admixture of both conventional chondrosarcoma (left) and chondrosarcoma showing clear cell change, including woven bone formation (C). High-power microscopy shows the polygonal tumor cells with lightly eosinophilic cytoplasm and prominent cell borders, characteristics of clear cell chondrosarcoma. In this tumor, the clear cell change is a minor component (D).
Discussion
In this study, we present the clinical, radiographic, and histologic characteristics of two additional tumors, in which we have recognized clear cell chondrosarcomatous areas admixed as a minor component of a conventional chondrosarcoma both occurring in the ribs of patients (one with MHE and one without MHE). To our knowledge, conventional chondrosarcoma with focal areas of clear cell features has been rarely reported in other sites but has never been reported in the rib. Both of our tumors occurred in adult males in the rib. The largest series to date consists of five patients with two arising in the femur, and one each in the tibia, iliac bone, and nasal septum, respectively. 3 Interestingly, one tumor in our series occurred in the setting of multiple hereditary exostoses (MHE), which, to our knowledge, has also never been documented in the literature.
Clear cell chondrosarcoma is a rare, low-grade subtype of chondrosarcoma with a predilection for the epiphysis of long bones, most commonly seen in the proximal femur. It is slow-growing and has an excellent prognosis with a 10-year overall survival rate of 89%. 5 Clear cell chondrosarcomas are not known to harbor IDH1/2 mutations, unlike primary conventional chondrosarcomas. 6 Microscopically, the tumor has a lobular architecture with the center of the lobule, usually showing woven bone formation. The tumor cells have abundant pale eosinophilic to clear cytoplasm, centrally located nuclei, and distinct cell borders. Mitotic figures are rare.
Unni et al first described clear cell chondrosarcoma in 1976. They noted that these tumors may contain areas of conventional low-grade chondrosarcoma either as large lobules of tumor cartilage surrounded by clear cells or as small inconspicuous foci among the clear cells. 1 However, the opposite phenomenon of smaller areas of clear cell chondrosarcoma within conventional chondrosarcoma has not been well described.
Recently, Lam et al reported five patients with conventional chondrosarcoma with clear cell chondrosarcomatous components accounting for 5-20% of the tumors. 3 Similar to our tumors, they observed gradual merging of the two components. Molecular analysis showed IDH1 mutations in three tumors with the same mutation identified in both conventional and clear cell components; one of the three harbored TP53 mutation in both components. The other two tumors did not have an IDH mutation, so molecular analysis was not performed in the clear cell component. It should be noted that IDH1/2 mutation studies would not be helpful in the tumor arising in the setting of our patient with MHE as secondary peripheral chondrosarcomas in these patients arise from cells with at least one functional copy of EXT gene and acquire mutation(s) not related to EXTs, frequently TP53 and CDKN2A mutations but not IDH1/2 mutations as would be expected in primary/de novo chondrosarcoma.7–10 Lam et al suggested that these neoplasms be considered conventional chondrosarcoma with clear cell change rather than a collision tumor or clear cell chondrosarcoma with extensive conventional components. It is also our opinion that our two tumors should be considered conventional chondrosarcoma with clear cell features/change.
Prior to the series by Lam, Dallas et al reported an example of a 32-year-old man with a pelvic secondary peripheral chondrosarcoma, grade 1, arising within an osteochondroma that contained a minor component of clear cell chondrosarcoma at the origin of the osteochondroma stalk within the medullary cavity of the underlying ilium bone. Interestingly, only the clear cell chondrosarcoma component metastasized widely to the patient's skull and lungs without any admixture of the low-grade conventional chondrosarcoma component emphasizing the importance of accurate histologic recognition at the time of the original diagnosis. 4
The clinicopathologic findings of all eight tumors (including this present series) are summarized in Table 1. Overall, the clinical data were similar to those of conventional chondrosarcoma: most tumors developed in older adults (median 53.5 years; range 15-79 years), affected men more than women (M:F = 3:1), and arose in flat bones and metaphysis or diaphysis of long bones. The tumors ranged from 3.5 to 15 cm in size (mean 8.7 cm). All except one tumor (case 2) had extraosseous extension, and none of the tumors showed radiologic findings suggestive of clear cell chondrosarcoma. Half of the tumors showed a grade 2 conventional chondrosarcoma component. The amount of clear cell change was minor and ranged from 5% to 20%. In addition, the two components gradually merged rather than grew as an abrupt transition in all tumors except case 1. In terms of follow-up (mean 29 months, range 1-120 months), three patients died of disease: two were with grade 3 and one grade 2. One patient with grade 1 was alive with metastatic disease (all clear cell chondrosarcoma) and the other patient with grade 1 had no evidence of disease. The prognosis of chondrosarcoma is directly based on the grade of the conventional chondrosarcoma component in a three-tiered system (Grade 1-3); however, it is unknown if the behavior of tumors with clear cell features is driven by the grade of the conventional component or the clear cell component as only a limited number of tumors have been reported in the literature and more long-term data with clinical follow-up are needed.
Summary of Conventional Chondrosarcoma with Clear Cell Features in the Literature.
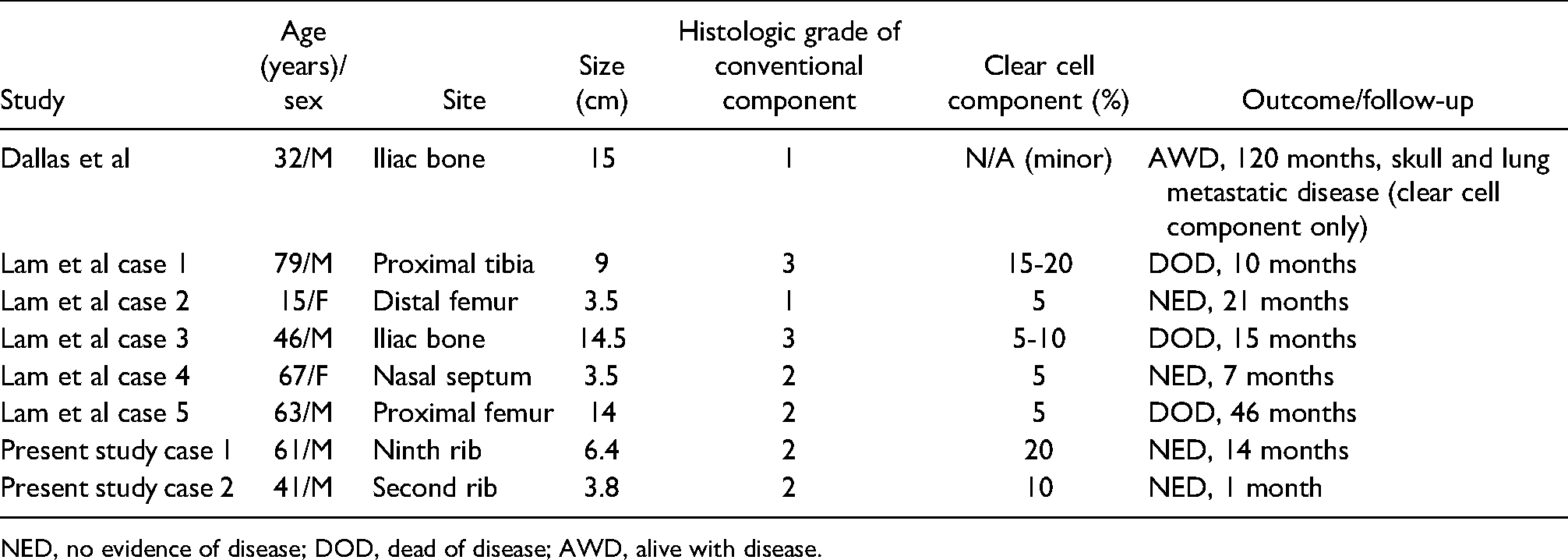
NED, no evidence of disease; DOD, dead of disease; AWD, alive with disease.
In summary, we report two additional patients with conventional chondrosarcoma with clear cell features. The significance of clear cell features in an otherwise typical conventional chondrosarcoma, to our knowledge, remains unknown and deserves recognition. Nonetheless, one should not confuse this unusual phenomenon with a primary clear cell chondrosarcoma as we believe these are conventional chondrosarcomas with clear cell features. Until more long-term data regarding their behavior can be analyzed, we want to emphasize that these tumors should continue to be graded in the conventional three-tiered system but hopefully this series will bring awareness of this phenomenon and more cases can be identified. Finally, these additional cases highlight the need for careful histologic examination, adequate specimen sampling at the time of grossing, and proper classification as unexpected findings may impact management.
Footnotes
Author Contributions
SW, HJ: conception, acquisition of data, analysis and interpretation of data, drafting the manuscript, final approval of the manuscript; AWJ, EFM, CDM, JMG: conception, acquisition of data, analysis and interpretation of data, revising the manuscript, final approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Johns Hopkins Medicine Institutional Review Board (JHM IRB). A case report does not have to be reviewed to by the JHM IRB.
Informed Consent
Not applicable, because this article does not contain any clinical trials.
Trial Registration
Not applicable, because this article does not contain any clinical trials.