
Abstract
Background. Frozen sections (FS) are common in neurosurgery to address varied clinical concerns. Artifacts in central nervous system (CNS) FS can be severe and affect or hinder interpretation. We performed a case-control study using a semiquantitative scale: the Histologic Preservation Score (HPS), and a quantitative scale: the Ice Crystal Vacuolization Score (ICVS), to compare the histologic quality yielded by snap- versus cryostat freezing techniques. Material and Methods. All specimens were sectioned in 2 halves, one half was used for FS and the other for permanent evaluation. HPS assigns a distortion score to the FS sample using the non-frozen half as the comparator: 1 = minimal, 2 = slight, 3 = moderate, 4 & 5 = severe. The ICVS is the average size in µm of the 5 largest vacuoles/0.05 mm2, evaluated on digitized slides. Results. 86 CNS-FS were collected: 22 snap- and 64 cryostat-FS. Significant differences in HPS: 2.28 versus 2.84 (p <0.05) and ICVS 7.47 versus 14.56 (p < 0.001) were obtained for snap- versus cryostat-FS, respectively. HPS and ICVS showed a strong correlation: R2 = 0.63, p < 0.0001. Histologic distortion was worse for neuroglial than mesenchymal tissue by both methods; however, a significant difference was only observed in cryostat-FS: HPS: 3.23 versus 2.33, p < 0.001; ICVS: 16.86 μm versus 10.26 μm, p < 0.001. Conclusion. Snap-FS yields better histologic quality than cryostat-FS for CNS-FS, and the difference is more pronounced in neuroglial samples. HPS and ICVS correlate strongly, indicating that the histologic quality is inversely proportional to water-crystallization. These results may apply to other areas of surgical pathology.
Introduction
Frozen sections are one of the most important, difficult, and stressful tasks surgical pathologists perform. 1 Interpretation of central nervous system (CNS) frozen sections is particularly challenging because most samples are minute and almost always distorted by edema, hemorrhage, and/or necrosis, which amplify the morphologic distortion inherent to freezing techniques. 2 The correct interpretation of CNS frozen sections determines if sampling is adequate for definitive diagnosis and classification of diseases, and whether there is indication for specific triage of the specimen (eg cultures, lymphoma work-up), or if additional resection is needed during the ongoing surgical act. Despite the critical relevance of this high-risk procedure, there is lack of evidence-based data about the optimal freezing technique for neurosurgical samples.3–5 We conducted a case-control study of CNS-frozen sections using two of the most common freezing techniques: cryostat-freezing and snap-freezing. A qualitative analysis was performed using two semiquantitative scales created or modified for this study: the Histologic Preservation Score (HPS) and an Ice Crystal Vacuolization Score (ICVS) to determine if significant differences exist between these two freezing techniques. We also performed a chart review to assess if the quality of the FS impacted the surgical management of these patients.
Material and Methods
After obtaining institutional IRB approval for the study (IRB#2101304482), CNS-frozen sections were assigned to either cryostat- or snap-freezing by the FS-pathology assistants using a randomization table; however, in cases staffed by neuropathologists not participating in the study, the method was deferred to their preferences. Before initiation of the study, both methods were regularly used at our institution. Prior to intraoperative consultation, the patient's imaging findings and clinical history were reviewed by the attending neuropathologist on service. Only biopsies from suspected neoplastic disease were included in the study because these represent the most common sample type in our institution. Prior to freezing, biopsies were split into even-sized halves along their longest axis. One half was used for frozen sectioning and the other half was placed in 10% buffered formalin for permanent processing per institutional protocol. For both freezing techniques, the tissue was placed on a cryostat chuck previously covered with a thin layer of frozen optimal cutting temperature compound (OCT). Then, an additional layer of liquid OCT was applied to cover the tissue and the frozen OCT base. The samples assigned to cryostat-freezing were placed on the freezing shelf within the cryostat at temperatures ranging from −18 to −21 °C and covered with an aluminum heat extractor (weight) to accelerate the freezing process and to create a flat plane for cutting. The samples assigned to snap-freezing were submerged using a metallic dipper in a container with isopentane (methylbutane) chilled in dry ice in a Styrofoam cooler to a temperature of −78 °C. After the second layer of OCT visually changed from transparent to white, the samples were placed on the cryostat microtome and sectioned at a thickness of 3 μm, the tissue ribbons were mounted on charged glass slides, fixed briefly in 95% ethanol, and stained with hematoxylin and eosin (H&E) following our department's standard procedure.
Morphologic Analysis
Histological Preservation Score (HPS)
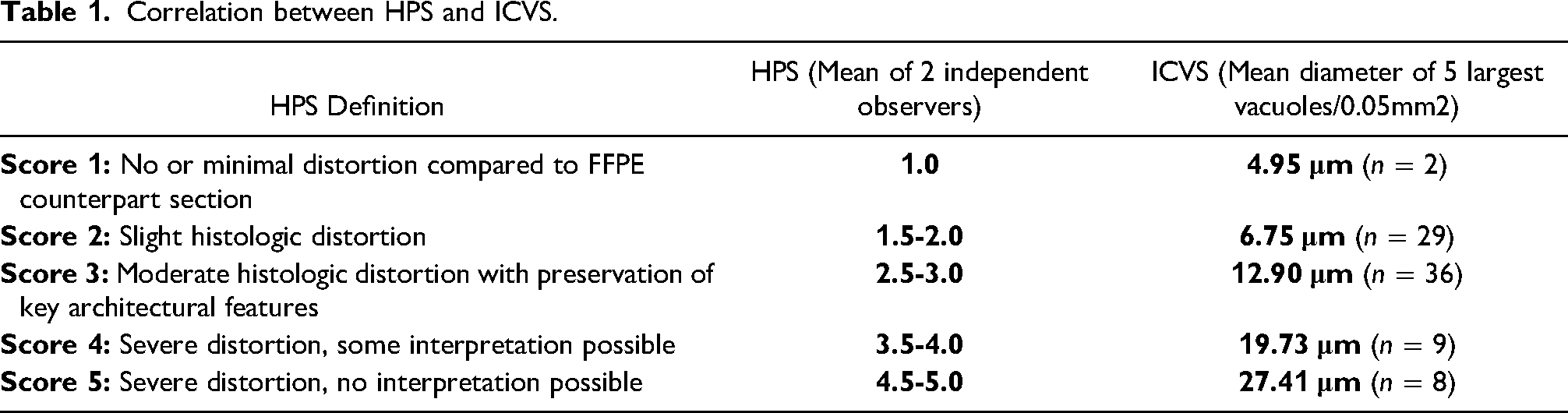
In all cases, the tissue was equally represented in both the frozen sections and the formalin-fixed paraffin-embedded sample. Two experienced neuropathologists (DSP and AOV) blindly reviewed each pair of frozen section and formalin-fixed paraffin-embedded glass slides and assigned a histological preservation score (HPS) designed for this study (Table 1): Score 1: optimal, little or no difference between frozen section and formalin-fixed paraffin-embedded sample; Score 2: slight but noticeable differences between frozen section and formalin-fixed paraffin-embedded sample not affecting interpretation; Score 3: moderate distortion but interpretation not compromised; Score 4: severe distortion, interpretation possible but compromised; Score 5: severe distortion, interpretation not possible. The individual scores from each neuropathologist were averaged to determine the final HPS.
Correlation between HPS and ICVS.
Ice Crystal Vacuolization Score (ICVS)
All body tissues have a high content of water and formation of water crystals normally occurs during freezing, resulting in artifactual vacuolization of FS.2, 6 H&E-stained FS slides were scanned using a Philips digital pathology slide scanner (software version 3.1.1.2) for image analysis. From an intermediate power (200X) the area with the best-preserved histology was marked with a 0.5 mm2–diameter circle. The circled area was then reviewed at a higher magnification (400X) and the area with the best-preserved histology was marked with a new 0.05 mm2–diameter circle. The diameters (in μm) of the five largest vacuoles within the smaller circle were recorded, and their average was designated as the Ice Crystal Vacuolization Score (ICVS) for that given FS. For oval shaped vacuoles, the largest and smallest diameters were averaged.
Clinical Impact
Pathology reports and neurosurgical operative notes were reviewed to determine if the FS diagnosis affected the patient's surgical management and if this correlated with our qualitative analysis.
Statistical Analysis
The clinical and experimental data were collected with Microsoft Excel 2016. The statistical analysis was performed with Graph-Pad Prism software version 7. Values were expressed as mean ± SD. Student t-test was used for statistical comparison of continuous variables and chi-square test for categorical values. The level of statistical significance was set at a p-value < 0.05.
Results
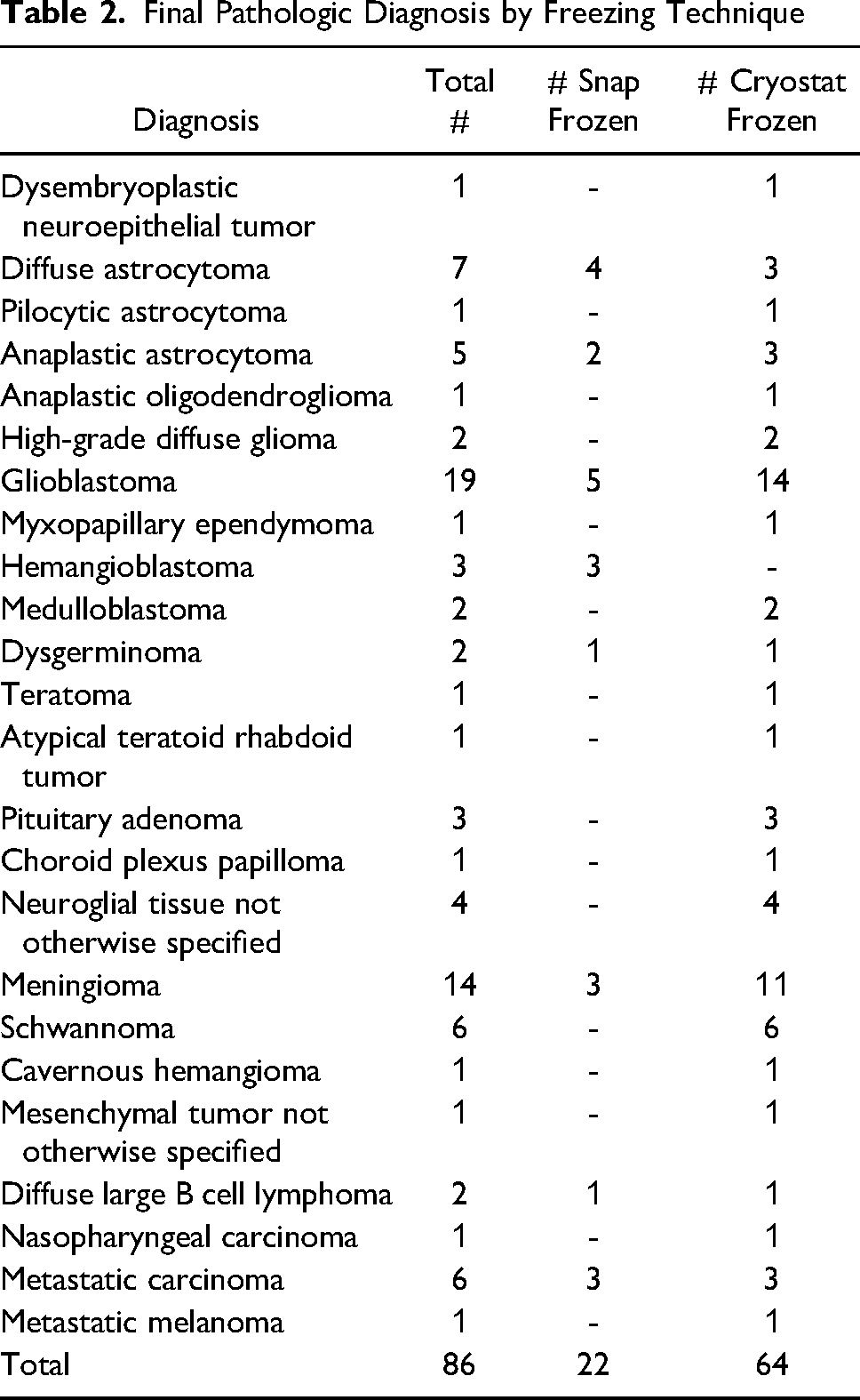
A total of 86 frozen sections were collected: 22 snap- and 64 cryostat-frozen sections. Forty-four frozen sections (51%) consisted of neuroglial tissue, 26 (30%) were intracranial mesenchymal lesions (eg schwannoma, meningioma), 8 (9%) were metastases or contiguous spread of head and neck malignancies, and 8 (9%) were designated as miscellaneous lesions, including germ cell tumors, lymphomas, and pituitary adenomas. Table 2 shows the final pathologic diagnosis of all cases by freezing method.
Final Pathologic Diagnosis by Freezing Technique
Comparison of Cryostat- versus Snap-Frozen FS
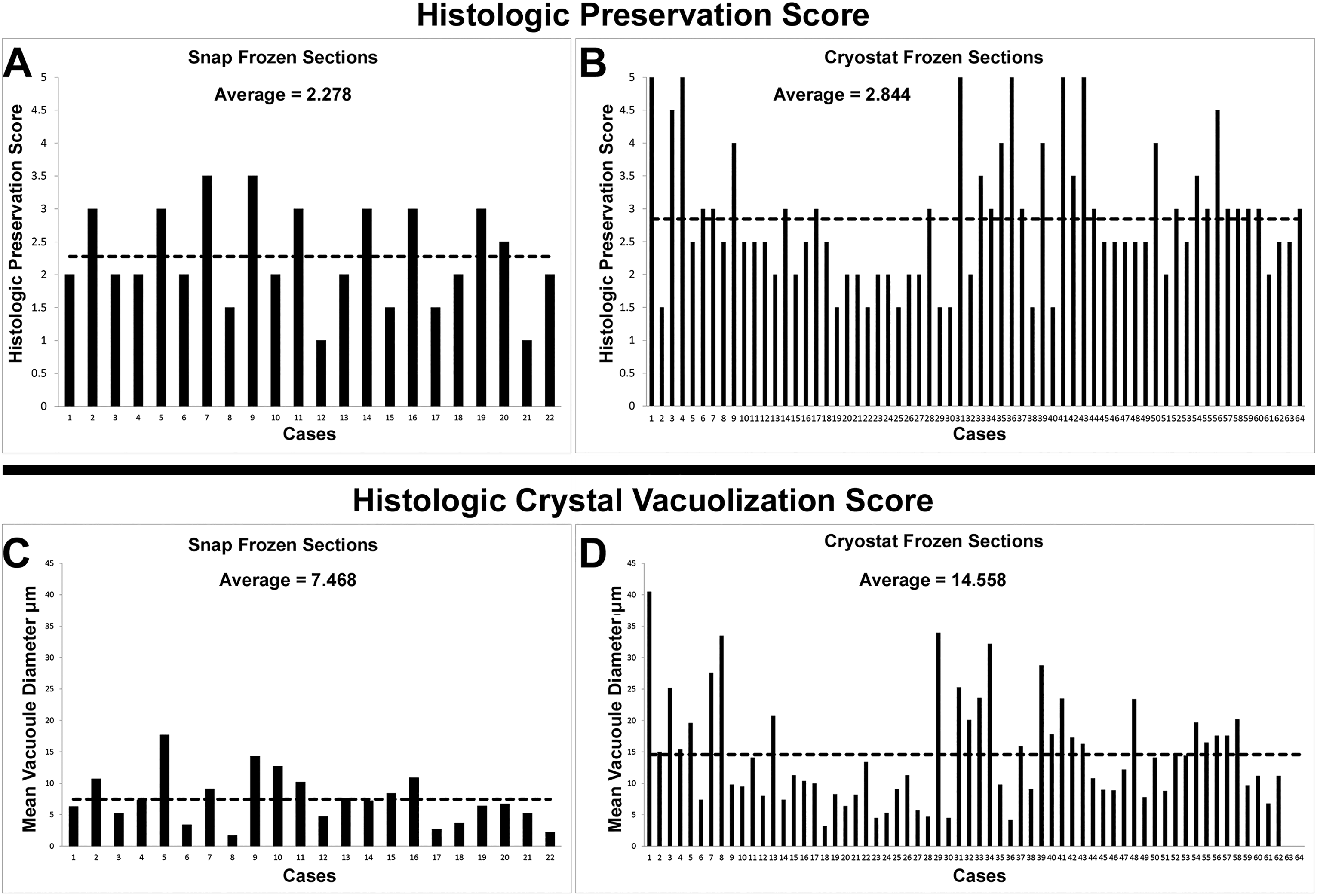
The mean and standard deviation (SD) for the HPS for all tissue types was 2.28 ± 0.80 versus 2.84 ± 1.08 for snap-frozen sections versus cryostat-frozen sections, respectively. This difference was statistically significant: p-value = 0.0175. The mean ± SD ICVS for all tissue types was 7.47 ± 4.07 versus 14.56 ± 8.31 for snap-frozen sections versus cryostat-frozen sections. This difference was statistically significant: p-value <0.001 (Figure 1). Additionally, small vacuoles (ICVS < 10 μm) were more common in snap-frozen sections versus cryostat-frozen sections: 72.7% versus 40.3% (p-value = 0.12), while large vacuoles (ICVS > 20 μm) were more common in cryostat-frozen sections versus snap-frozen sections: 22.6% versus 0 (p-value = 0.08), although these differences did not reach statistical significance.
Comparison of Snap- and Cryostat-Frozen Sections by Tissue Type: Neuroglial versus Mesenchymal
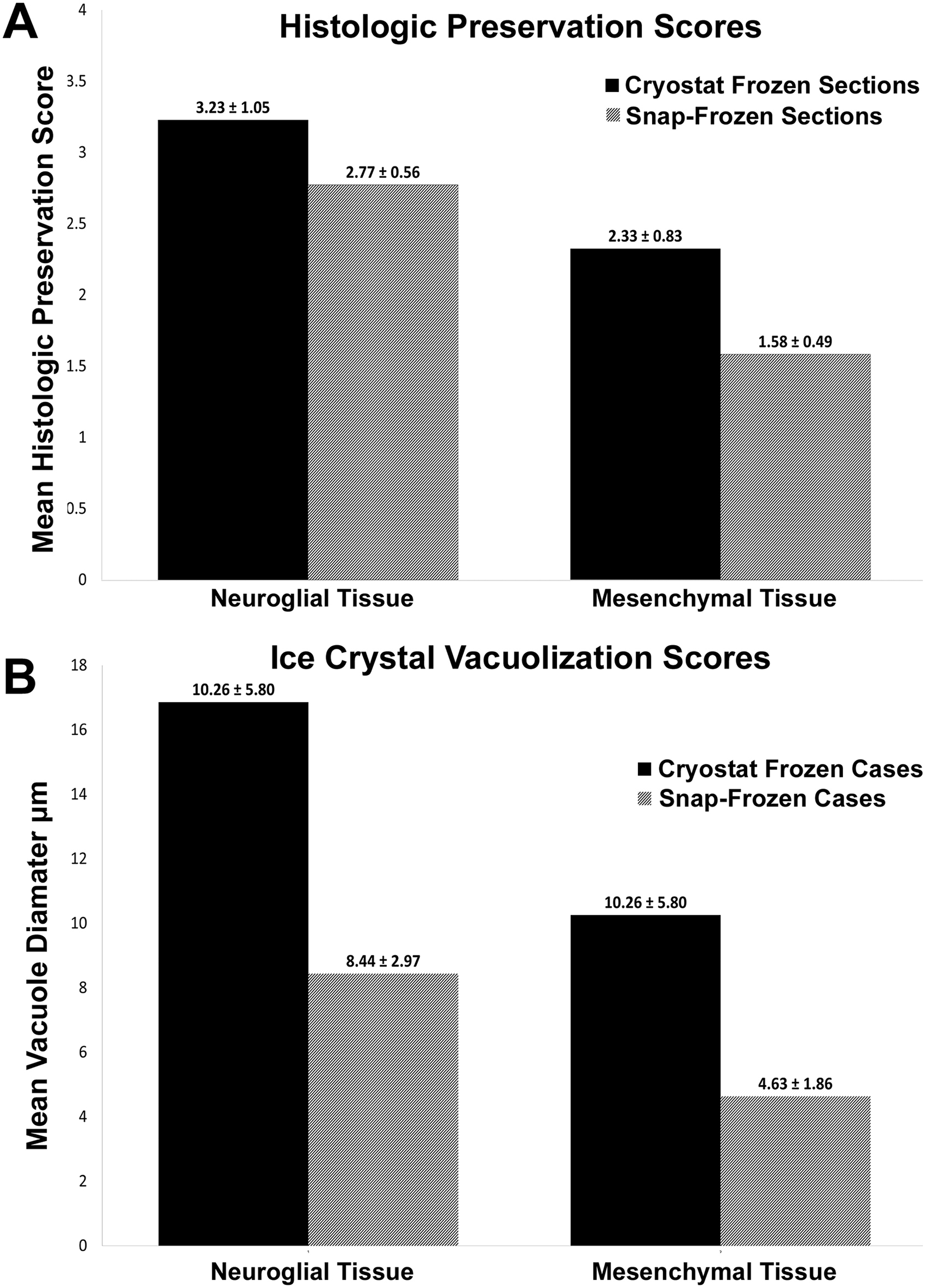
The mean ± SD HPS for neuroglial tissue was 2.77 ± 0.56 versus 3.23 ± 1.05, and for mesenchymal tissue was 1.58 ± 0.49 versus 2.33 ± 0.83 for snap-frozen sections versus cryostat-frozen sections, respectively. There was a statistically significant difference of the mean HPS (p-value < 0.001) for neuroglial versus mesenchymal tissue, but only for cryostat-frozen sections, explained by the fact that 10 of 12 (83.3%) cryostat-FS that had an HPS of 4-5 were neuroglial tissue. The mean ICVS for neuroglial and mesenchymal tissues were 8.44 ± 2.97 and 4.63 ± 1.86 µm, versus 16.86 ± 9.18 and 10.26 ± 5.80 µm for snap-frozen sections versus cryostat-frozen sections, respectively (Figure 2). There was a statistically significant difference (p-value < 0.001) between the mean ICVS of neuroglial versus mesenchymal tissue, but only for cryostat-frozen sections. Ten (71.4%) of the 14 cryostat-frozen sections with ICVS > 20 µm (large vacuoles) were of neuroglial tissue, three (21%) were in the miscellaneous tissue group (pituitary adenoma, germinoma, metastatic malignancy), and one (7%) was a mesenchymal tumor (meningioma).
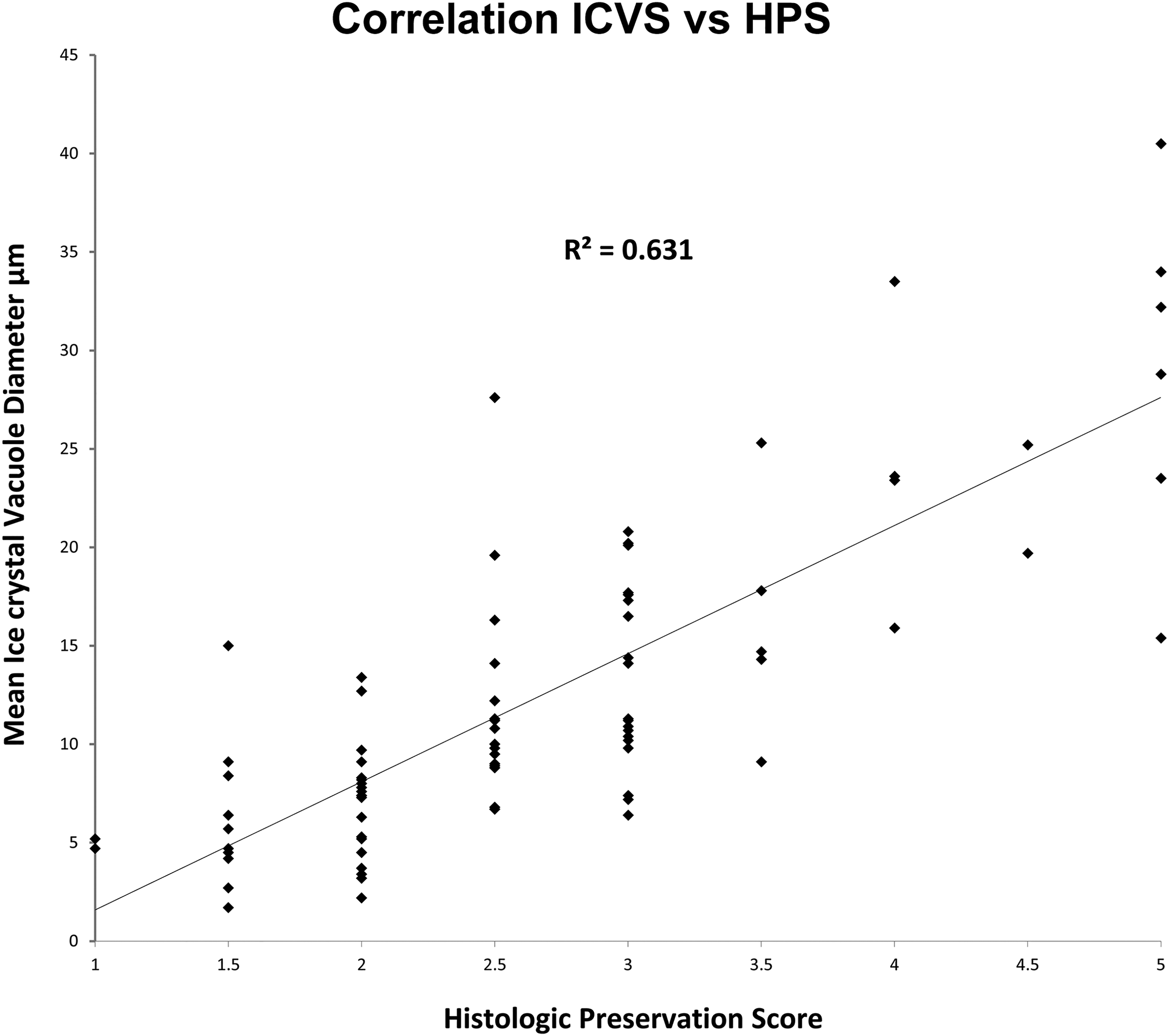
Correlation of HPS and ICVS
Photomicrograph examples of representative snap- and cryostat-frozen sections with their corresponding HPS and ICVS are shown in Figure 3. Both scores showed a significant strong correlation: coefficient of determination R2 = 0.63, p-value <0.0001 (Figure 4).

Effects on Diagnosis and Surgical Management
For the study, frozen section diagnoses were classified into “non-specific” versus “specific” diagnosis. Non-specific included cases in which the diagnosis was deferred to permanent sections, or a diagnosis of “tumor tissue present” was reported, without specifying tumor lineage or grade. Specific diagnoses included cases in which a diagnosis of neoplasm, including tumor lineage and grade were reported, and cases reported as benign. Fifteen of 86 specimens (17%) had a high HPS of 4 or 5 (severe distortion): most of these cases (n = 13, 87%) were cryostat-frozen sections, and the remaining two (13%) were snap-FS. All five non-specific diagnoses occurred in cryostat-frozen section cases within this group. After review of the neurosurgical operative notes, a definitive impact on surgical management after a “” nonspecific diagnosis” could not be identified. It is nevertheless reasonable to assume that lack of diagnostic precision may impact surgical management and/or require submission of additional tissue samples with possible harm to the patient.
Discussion
Despite the potentially devastating consequences that an erroneous interpretation of a CNS-frozen section may have for the patient, and the medicolegal ramifications it may have for the neuropathologist or an institution,3, 7 it is difficult to find evidence-based data about which freezing technique yields the best histological preservation for CNS-frozen sections.
We made a comparative qualitative analysis of 86 consecutive CNS-frozen sections using two of the most widely available freezing techniques: cryostat-frozen section versus snap-frozen section. For the study we created a 5-tiered semiquantitative histologic scale: the Histologic Preservation Score or HPS, which assigns increasing scores according to the degree of histologic distortion: none (score 1), mild (score 2), moderate (score 3) and severe (scores 4/5), using a non-frozen FFPE half of the specimen as the comparator. The severe group was further segregated into cases in which some interpretation was still possible (score 4) and cases in which no interpretation was possible (score 5). Scoring was performed by two experienced neuropathologists. Additionally, since one of the most important known freezing artifacts is the formation of water crystals that disrupt and distort the tissues, 2 we used a second parameter previously established in nonhuman tissue studies 6 to assess freezing induced tissue distortion: The Ice Crystal Vacuolization Score or ICVS. For this analysis, frozen section slides were digitized using a pathology slides digital scanner. The ICVS is the average diameter of the five largest vacuoles (in µm), measured with the measuring tools provided by the scanner's software, within an area of 0.05 mm2. The ICVS was assessed only in the most well-preserved areas of the FS slide. In our study, the HPS and ICVS showed a strong correlation, supporting the notion that water-crystallization plays a major role in causing freezing artifacts. Additionally, snap-frozen sections showed significantly lower HPS and ICVS than cryostat-frozen sections, indicating that snap-frozen sections yield a better histologic preservation due to reduced formation of water crystals, and therefore represent a superior technique for CNS-FS. Most of the cases with severe distortion (87%) and all the cases in which a specific diagnosis was not possible were in the cryostat-frozen section group. In studies with non-human tissues, it has been previously established that the rate of heat removal from tissues during freezing significantly affects the water crystallization process. 6 The critical range for water crystallization in tissues is between −1 and −8° C, 6 and the rate of formation, size, and morphology of the ice crystals is directly linked to the length of time required to cool down out of this range, also known as the “characteristic freezing time”.8, 9 An experimental study on a range of freezing velocities found a consistent logarithmic correlation between the ICVS and the time-length needed to surpass the “characteristic freezing time”. 10 Our results show that snap-frozen sections produce a significantly lower ICVS than cryostat-frozen sections and therefore this method must be associated with a shorter “characteristic freezing time”, which translates into less and smaller ice crystals. Our study also shows higher ICVS (vacuolar distortion) in frozen sections from neuroglial tissues than mesenchymal tissues with both methods; however, the differences only reached statistical significance for cryostat-frozen sections. This result suggests that the water content, and thus the susceptibility to freezing artifact, is higher in neuroglial lesions, and that this phenomenon is worse in cryostat-frozen sections than snap-frozen sections. A likely explanation for this result is that neuroglial lesions, in general, have a higher content of water, since most neuroglial pathologies, neoplastic and non-neoplastic are usually associated with edema. Shape and size of the samples affect the freezing process because these parameters influence the heat transfer coefficient: size is inversely proportional, and surface area is directly proportional to cooling time, respectively; however, the vast majority of samples sent for frozen section are small and comparable in size and shape. For this reason, these parameters were not included as inclusion/exclusion criteria for this study. 11
These results also suggest that the quality of CNS-frozen sections could be further improved by freezing techniques with faster heat extraction leading to shorter “characteristic freezing time”. Snap-frozen section studies using liquid nitrogen, which has a boiling temperature of minus 195.79 °C, describe that the interaction between the fresh tissue and the liquid nitrogen creates a vapor barrier that leads to an unpredictable freezing pattern that causes cracking of the tissue and OCT making it inadequate for intraoperative frozen section . 12 This could be avoided by using a liquid cooling medium for efficient homogeneous heat extraction such as isopentane, as is usually done for muscle biopsies; however, since this method requires freezing and thawing of the isopentane, which will lead to increased turn-around time, it is not practical for intraoperative use.
In our laboratories, we use containers with isopentane cooled with dry ice in a Styrofoam cooler for snap-frozen sections. It takes about 20 to 30 min for the isopentane to cool down to the intrinsic temperature of the dry ice (−78.5 degrees Celsius), and then it can be used for the remainder of the day. The temperature is monitored with a NIST certified thermometer. Advantages of this method include that it is easy to implement, it is far less costly than commercially available mechanical freezing baths, it relies on the intrinsic properties of the dry ice and therefore does not require regular maintenance of the cooling mechanism, and finally, it maintains the purity of the isopentane and prevents hydration, because it is replaced daily. Our study was intended as a “best practice” activity to provide scientific support for choosing the optimal freezing method for CNS-frozen sections.
Snap-freezing of surgical tissue has no negative effects on the turn-around time. The freezing process is accelerated by snap-freezing compared to cryostat-freezing. After snap-freezing, however, the tissue block is significantly cooler compared to the cryostat temperature, and a waiting time could theoretically be considered for the block temperature to equalize with the cryostat temperature; however, in practice, we section the snap-frozen block immediately in the cryostat without any technical difficulties.
Even though snap-freezing yields higher histologic quality than cryostat freezing for CNS frozen sections, the latter is the most widely used method. Reasons for this include the lack of clinical studies comparing these methods resulting in neuropathologists being unaware of the differences yielded by these techniques, the universal availability of cryostats but not freezing baths in frozen section stations, the ability to easily freeze simultaneous samples with little effort in cryostats (since it does not require a submersion step or the use of a dipper), and not having to coordinate the logistics of having isopentane, dry ice, or mechanical freezing baths with their inherent cost and maintenance. Another reason not addressed in our study is that many neuropathologists circumvent the poor quality of cryostat frozen sections by complementing their intraoperative evaluation with cytologic preparations such as touch imprints and squash preparations.
We did not find evidence that a non-specific diagnosis due to poor quality of CNS-FS impacted the surgical management, but it did impact the quality of the diagnosis rendered at the time of the frozen section. The surgical questions leading to intraoperative consultation vary greatly according to the different clinical scenarios and neurosurgeon expectations. In some instances, the information sought is simply whether sampling is representative, if the amount of tissue is adequate for ancillary testing, and/or if there is a need to have a representative frozen sample for possible molecular studies. In such cases, a non-specific result, such as “abnormal tissue present”, may suffice. However, in other scenarios, differentiation between infectious, reactive, benign, and malignant processes, and further segregating among malignancies such as gliomas, lymphoma, or metastases, may be critical for triaging the sample adequately determining the extent of the resection. It is reasonable, therefore, to presume that the quality of CNS-FS could impact the surgical management, or at least lead to additional diagnostic procedures in some patients; however, this could not be proven in our study, possibly because our sample size is too small, and our study was not designed to address this complex question.
One major limitation of this study is that the two freezing methods could not be applied in parallel to the same specimen. The minute size of most neurosurgical specimens, the time constraints for frozen sections, and our department's policy of saving a portion of the specimen for optimal permanent processing (ie FFPE), did not allow such a study design. In fact, the “experimentation” performed in this study was only possible because in-house protocols allow for both freezing procedures to be performed and there is no data to favor one method over the other and equipoise between the two methods existed.
We provide evidence that snap-freezing of frozen pathological CNS tissues is superior to cryostat-freezing. Based on our findings, CNS biopsies are now routinely snap-frozen in our institution. Our study also showed that neuroglial tissues are more susceptible to freezing artifact than mesenchymal lesions, most likely due to edema-associated increased water crystallization. We plan to conduct studies to determine if this also applies to other tissue types.
Conclusions
Our study confirms that a statistically significant inversely proportional relationship exists between water crystallization and histologic quality of CNS-frozen sections. Among the two freezing methods tested, snap-frozen sections yield lower water crystallization and better histologic quality than cryostat-frozen sections. We were unable to show that the quality of frozen sections had an impact on surgical management of neurosurgical patients. We hypothesize that the reason for this paradoxical result is the small sample size, and that the design of our study was inadequate to answer such a complex question.
Footnotes
Acknowledgements
The authors acknowledge Charlotte Brunner, PA and Cassandra M. Butler, PA for skillful performance of frozen sections. Dr Sihem Khelifa reviewed and edited the manuscript.
Author Contributions
DSP Performed microscopic evaluation of neuropathology glass slides and digitized images, data collection. TW Data collection, verified analytical methods, literature review, manuscript draft. FZ assisted in preparation of frozen samples, data collection and analysis. NA assisted in data collection and statistical analysis. HM Submitted IRB application, study design, data analysis, figures and tables drafting and editing, and manuscript draft. AOV Conceived the project, study design, microscopic evaluation of neuropathology slides and digitized images, manuscript draft.
Authors’ Note
David S. Priemer is also affiliated with Department of Pathology, F. Edward Hebert School of Medicine, Uniformed Services University, Bethesda, MD, USA 20814 and Henry M Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD, USA 20817.
Funding
This research was supported by funds of the IUHealth Pathology Laboratory. This research has been approved by the institutional review board (IRB).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approved study.
Trial Registration
Not a clinical trial.