
Abstract
A 54-year-old woman who incidentally noticed a “knot” in her left breast subsequently underwent excisional biopsy which yielded a diagnosis of malignant neoplasm with sarcomatous features. Given the broad differential diagnosis and imaging findings, the patient underwent bilateral mastectomy and intraoperative sentinel lymph node assessment. An 8.5 cm tumor that was further classified as a malignant phyllodes tumor was identified in the left breast, while the frozen section interpretation came back as positive for metastatic disease which resulted in left axillary lymphadenectomy. Two months later the patient progressed to distant metastatic disease and unfortunately passed away within 6 months after her initial diagnosis. Lymph node metastasis in phyllodes tumor is an exceptionally rare event for which patients usually do not undergo intraoperative sentinel lymph node examination; however high clinical suspicion of metastatic disease would be evidence for further investigation.
Introduction
Breast phyllodes tumors are a rare type of fibroepithelial tumor (<1% of all breast tumors) that are graded by the World Health Organization (WHO) as benign, borderline, or malignant based on certain histologic features. 1 Malignant features are characterized by stromal cellularity and overgrowth with atypia, permeative tumor border, increased mitotic count, and the presence of malignant heterologous elements. 1 Overall, patients with phyllodes tumors tend to have a good prognosis and are generally managed surgically, 2 with most being graded as benign. 1 While only accounting for a small fraction of phyllodes tumors, malignant phyllodes tumors that metastasize have devastating outcomes, with one review article estimating a 2.2-year survival rate of 11%. 3 Malignant phyllodes tend to behave like sarcomas and metastasize hematogenously, with the lungs being the most common site of metastasis. 4 Although 10–15% of patients with malignant phyllodes tumors may present with lymphadenopathy, they are usually benign, reactive hyperplastic lymph nodes. 4 Lymph node metastases were less frequent. Gullet et al conducted a retrospective study of lymph nodes from patients with phyllodes tumors, where they analyzed data across a 16-year period from the Surveillance, Epidemiology, and End Results SEER database. 5 They found that most patients with phyllodes tumors did not undergo regional lymphadenectomies (only approximately 25% of 1035 patients did), and only 9 of the 1035 patients had nodal involvement. Given the low lymph node involvement rate in phyllodes tumors, the National Comprehensive Cancer Network (NCCN) guidelines “recommend wide excision of the tumor without axillary staging”. 6
Case Presentation
A 54-year-old woman incidentally noticed a “knot” in her left breast after experiencing minor trauma. When it continued to increase in size, she followed up with her primary care provider, who scheduled her for excisional biopsy. The biopsy showed an undifferentiated malignant neoplasm with epithelioid and sarcomatoid morphology. Numerous immunohistochemical stains (IHC) performed on the biopsy showed no evidence of epithelial, melanocytic, or smooth muscle differentiation. Both TLE-1 and CD99 immunohistochemical stainings were weakly positive; therefore, FISH studies for ESWR1 and SS18 were performed and were negative, essentially excluding a Ewing sarcoma-related tumor and synovial sarcoma, respectively.
The patient was followed up with a CT scan of the chest, abdomen, and pelvis, as well as an MRI of the breast. While the CT scan did not reveal any evidence of metastasis at that time, a 6.5 cm mass involving the pectoralis muscle was observed in the breast. Furthermore, a breast MRI revealed an abnormal axillary lymph node. Due to the pathological findings, she was scheduled for a mastectomy (per patient preference, which ended up being a bilateral mastectomy). A sentinel lymph node biopsy was also planned based on the MRI findings. The frozen section intraoperative sentinel lymph nodes examination was positive for macro-metastatic disease which grant the patient left axillary lymph node dissection.
Grossing and Histology Description of the Tumor
The left total mastectomy showed 8.5 cm (in greatest dimension) ill-defined tan-white firm lesion located in span from medial to central breast that abuts the posterior margin and involving the subcutaneous in the areola region, additionally multiple tumor satellites were identified (Figure 1). H&E-stained sections showed diffuse spindle cell proliferation with a leaf-like epithelial pattern, stromal overgrowth (Figures 2 and 3), multinucleated stromal osteoclast-like giant cells, rare osteoid heterogeneous elements (Figure 4), high mitotic rate (>30 mitosis in one HPF), and high proliferation rate (Ki67 60% Figure 5). Satellite lesions showed similar tumor morphology. The surgical margins were negative for malignancy. CD34, S100, MSA (myosin specific actin), MyoD1, and high- and low-molecular-weight cytokeratins immunostaining were all negative. Additionally, 42 lymph nodes, including four sentinel lymph nodes, were examined and one of the sentinel lymph nodes was positive for macrometastatic disease (Figure 6). The histologic findings of extensive tumor overgrowth, high mitotic activity, invasion of the adjacent breast tissue, and positive lymph node warranted the diagnosis of high-grade (malignant) phyllodes tumor. The specimen was sent to an outside institution for next-generation sequencing of a sarcoma-targeted gene fusion panel that can detect the presence of rearrangements for 138 targeted genes, including MED12. 7 No reportable target fusions were identified, including MED12 fusion.
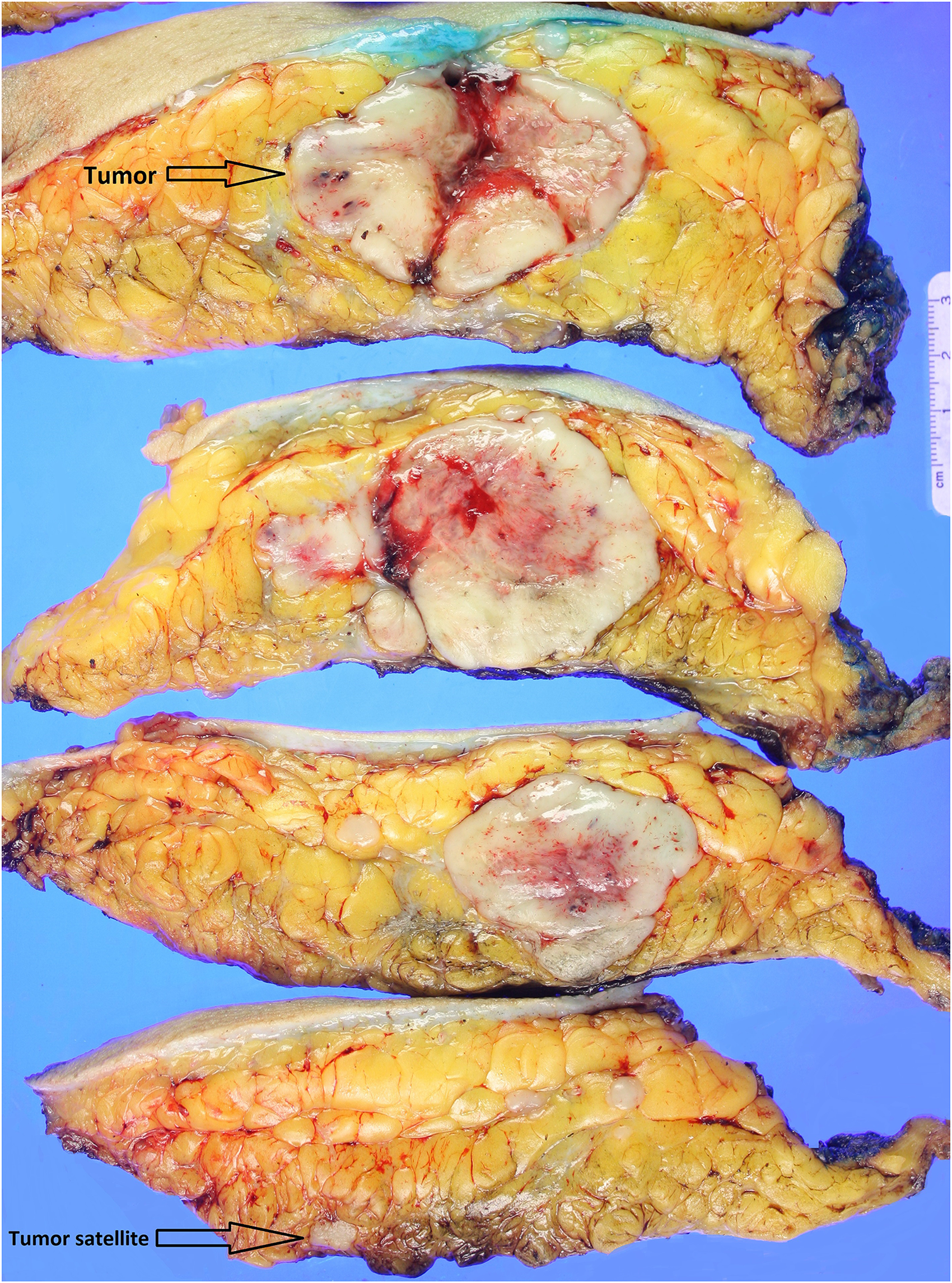
Mastectomy specimen, serially sectioned and revealed ill-defined tan-white tumor measured approximately 8.5 × 8.0 × 5.5 cm. It has an area of central necrosis, and multiple tumor satellites were appreciated.
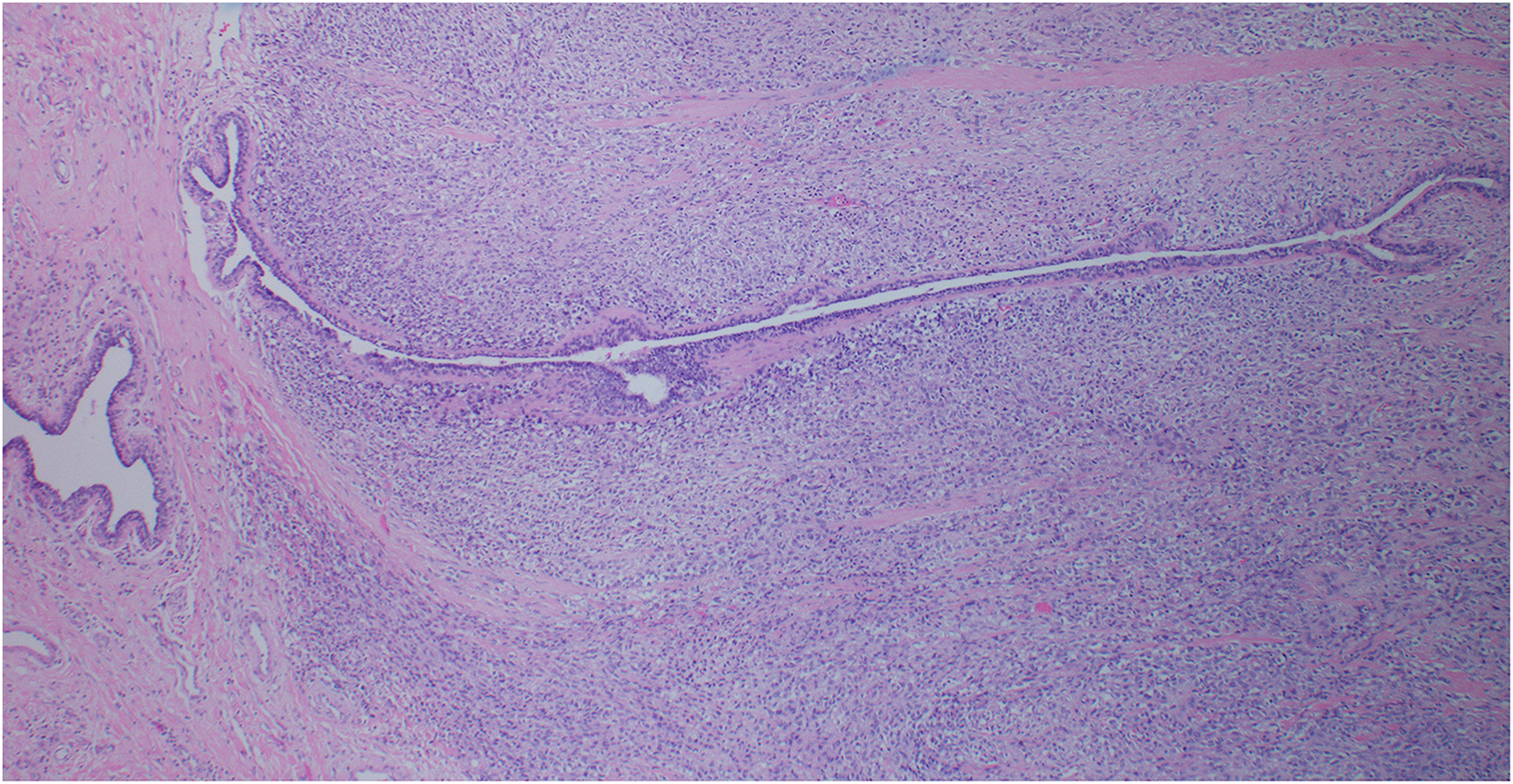
H&E- stained section of the breast tumor and shows leaf-like (phyllodal) epithelial pattern with sub-epithelial stromal condensation with increased stromal cellularity adjacent to epithelium.
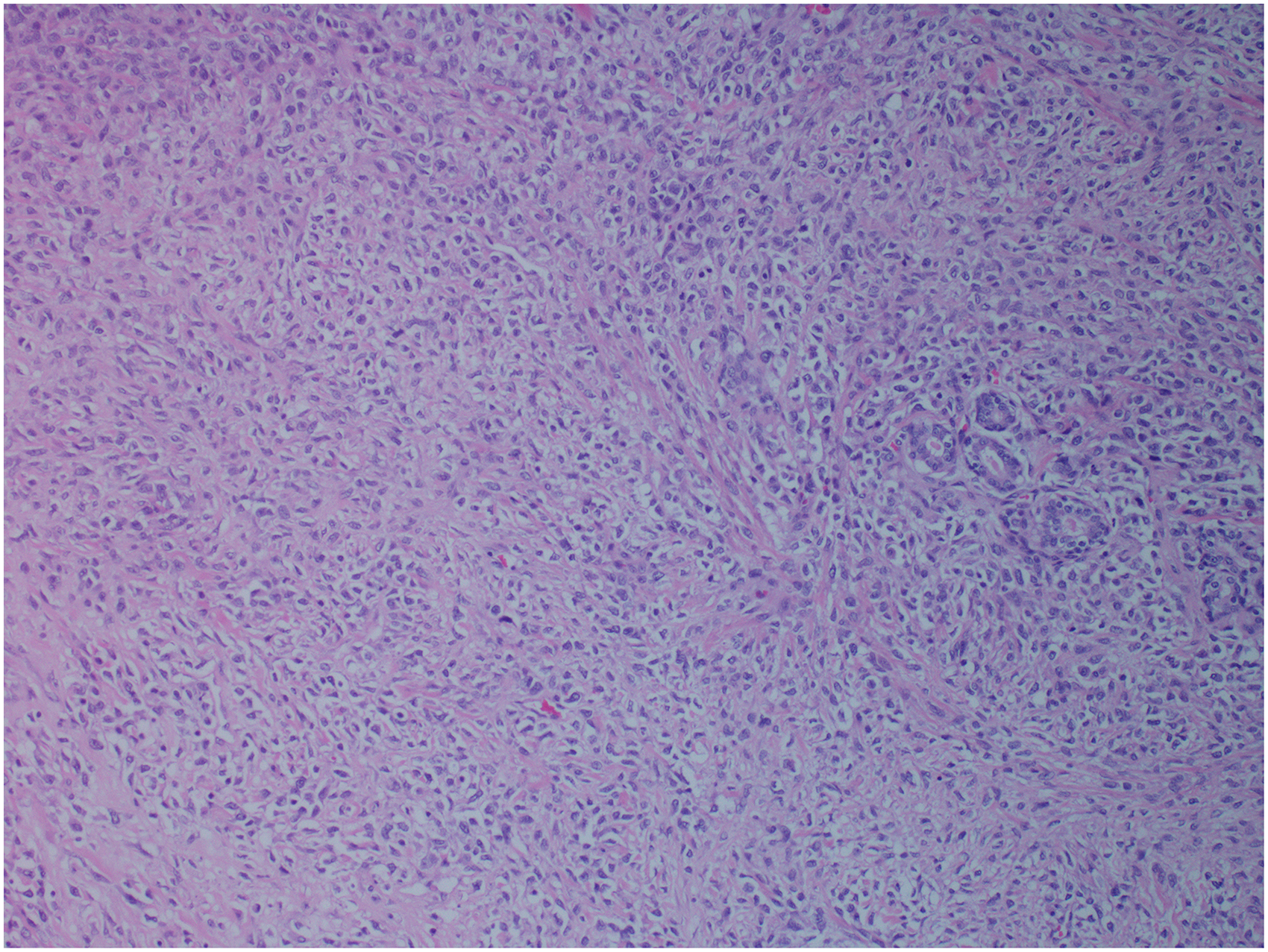
H&E- stained section of the breast tumor and shows stromal overgrowth at 4x magnification.
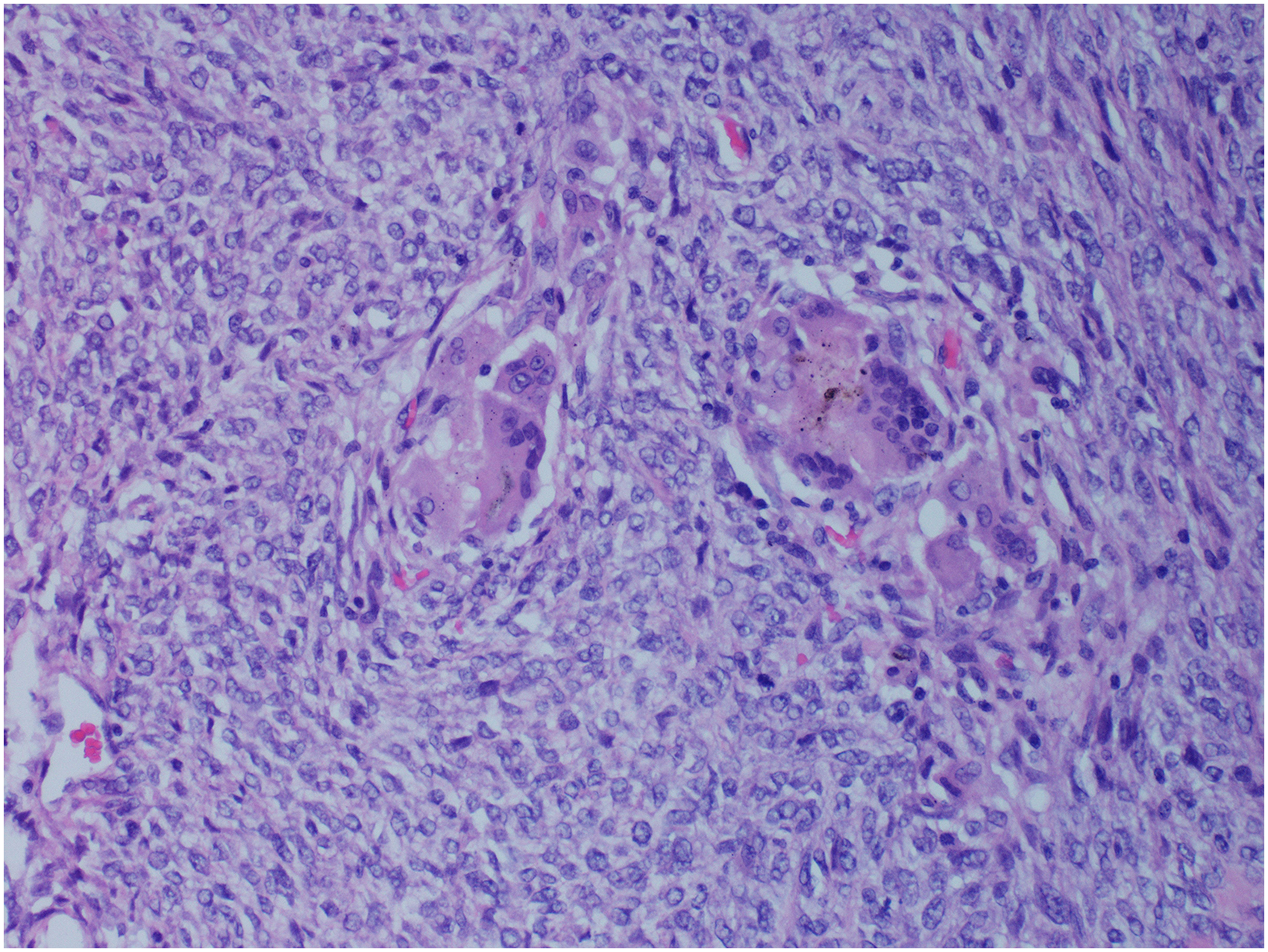
H&E- stained section of the breast tumor, higher magnification, shows a cellular stroma with atypia, mitosis and osteoclast like-giant cells.
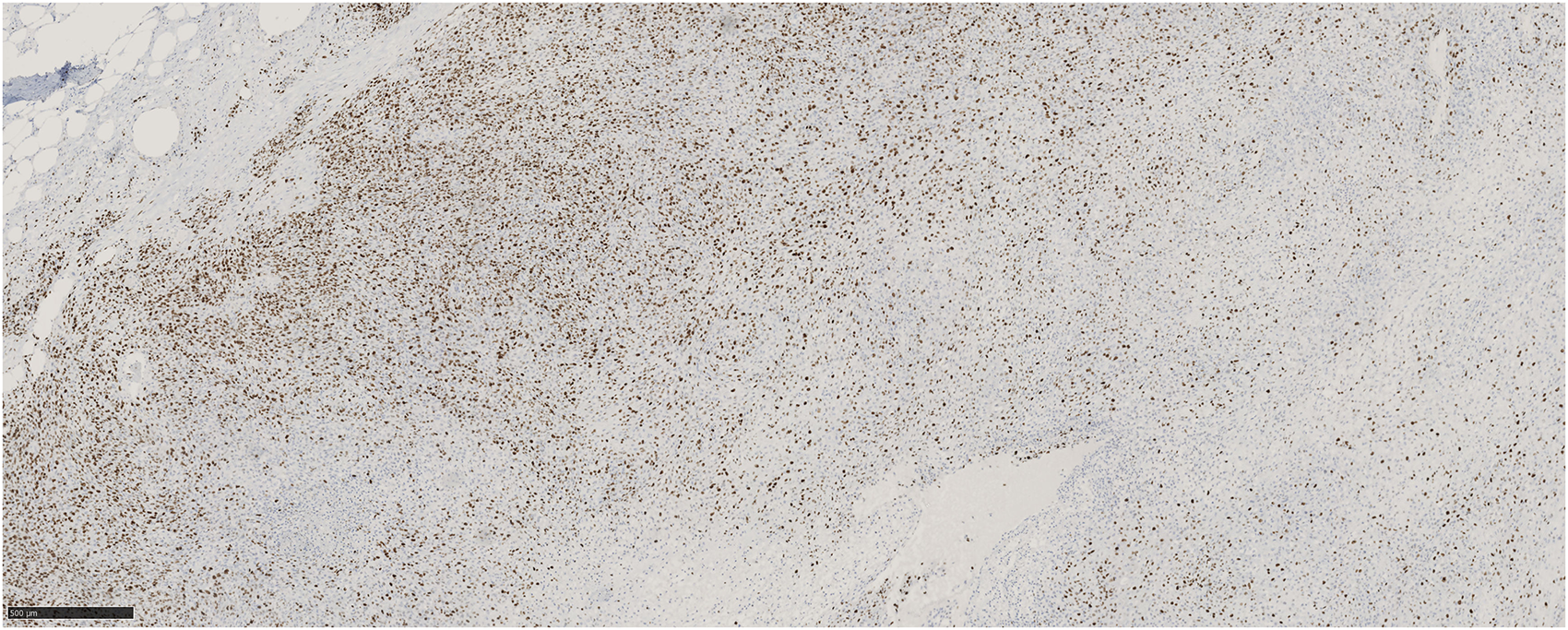
Ki-67 immunohistochemical stain, shows high proliferation rate.
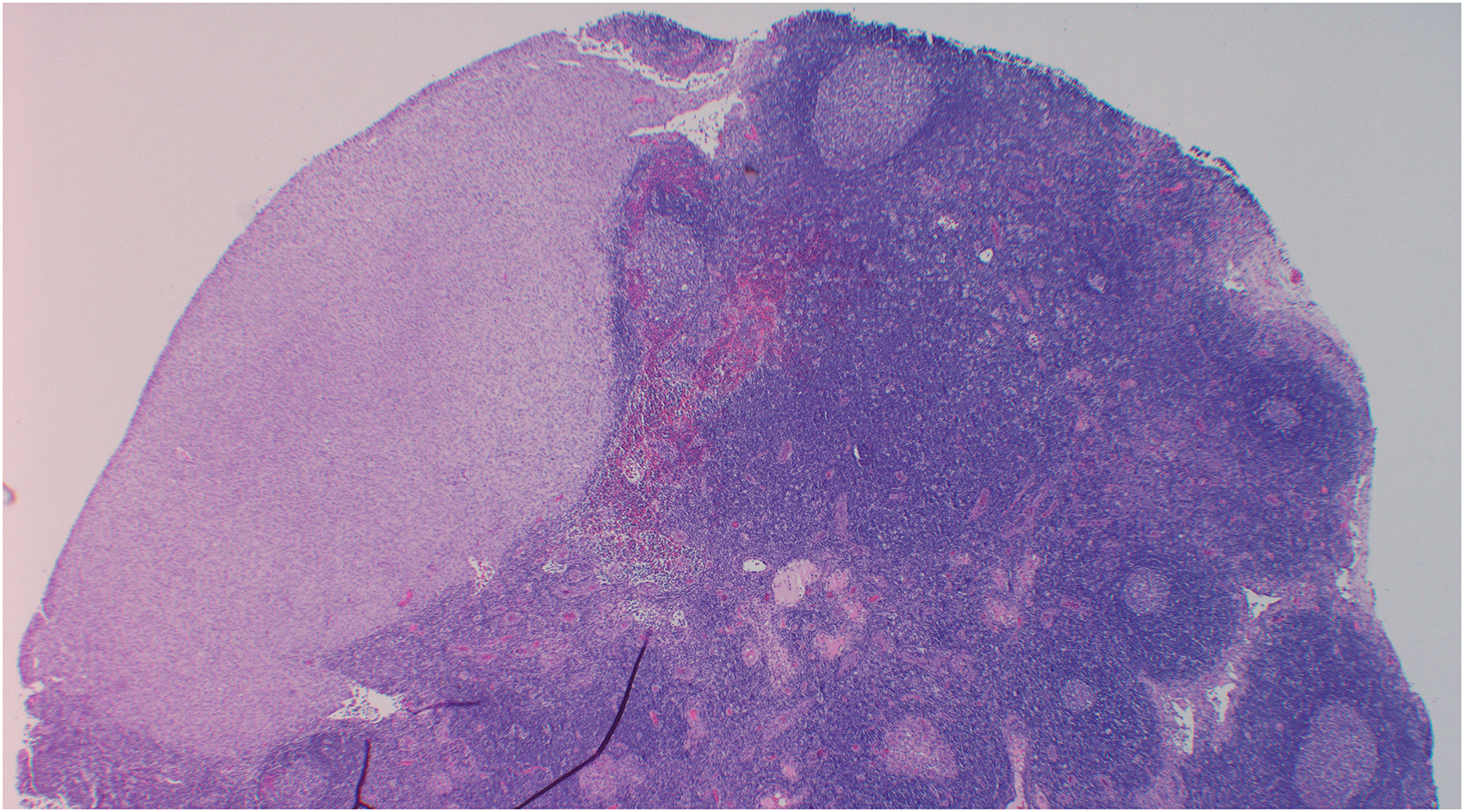
H&E- stained section of sentinel lymph node with subcapsular macrometastasis (wedge shaped), the tumor composed of spindle cell proliferation (stromal component only) with no epithelial component.
Despite the initial CT being negative for metastatic disease; two months later, a follow-up CT scan showed epidural, spinal, and pulmonary lesions concerning for metastatic disease. Resection of the left lower lobe lung wedge showed a tumor with histological features consistent with the previously diagnosed malignant breast phyllodes tumor, confirming patient’s metastatic disease. Follow-up palliative surgeries of the sacrum showed similar histological findings. Unfortunately, despite treatment measures, the patient died 6 months later due to respiratory failure caused by metastatic disease complications.
Discussion
We report this case to demonstrate a fatal and aggressive metastatic phyllodes tumor to the axillary sentinel lymph node, lung, and bone with negative MED12 and sarcoma gene fusion panel.
Metastatic phyllodes to the lymph nodes are rare events because they typically metastasize hematogenously. Therefore, the NCCN guidelines do not consider axillary staging necessary for patients with phyllodes tumors. However, a suspicious lymph node on imaging should warrant additional work-up, such as a lymph node biopsy, to rule out the presence of metastatic disease. 4 The rarity of this type of metastasis was demonstrated in a 2017 literature review by Koh et al, who analyzed 1806 cases of metastatic breast phyllodes tumors that were specifically assessed for axillary lymph node involvement. Of these cases, only 12 showed metastasis in the axillary nodes (0.7%), with study-specific percentages ranging from 0% to 14.3%. 4
Although histologic features such as tumor size, high mitotic count, presence of stromal hypercellularity, presence of stromal overgrowth, necrosis, marked cytologic atypia, and heterologous differentiation are associated with worse phyllodes classification (benign, borderline, to malignant); however, the phyllodes-related relapse- free survival is interestingly associated just with marked cytologic atypia, and the presence of heterologous elements based on Di Liso E, et al study. 8 These study findings are similar to what Koh et al reported previously in a series of 83 cases of malignant phyllodes which concluded that large tumors (≥9 cm) containing malignant heterologous elements have significantly worse metastasis-free survival and poorer prognosis. 9
To evaluate the genomic profile of malignant phyllodes tumors, Liu et al, at the University of California San Francisco studied 30 patients with phyllodes tumors (including 10 with malignant tumors). 510 cancer-related genes, selected introns from 40 genes, and TERT promoter mutations were evaluated by next-generation sequencing, and the following recurrent gene mutations were identified: TERT promoter (6/10), TP53 (4/10), MED12 (3/10), PIK3CA (3/10), FGFR1 (2/10), SETD2 (2/10) and KMT2D/MLL2 (2/10). 10
The frequency of MED12 mutations were studied thoroughly in 176 patients with phyllodes tumor (49 benign, 49 borderline, and 78 malignant) by Yoon et al, and showed clinicopathological characteristics associated with MED12 mutations. The presence of these mutations was associated with younger age, and lower mitotic activity; however, they were not associated with marked atypia or presence of heterologous elements. MED12 mutations tended to be associated with improved disease-free survival in malignant phyllodes tumor, but this was not statistically significant in this study because the number of patients who died of malignant phyllodes were only four. 11 Our patient in this case report had a negative MED12 which can be considered as a poor prognostic factor. Patient also has negative sarcoma fusion panel and did not include the above-mentioned fusions and TERT promoter mutations.
Additionally, the epithelial expression of estrogen receptors (ER) and progesterone receptors (PR) were studied in 143 patients with phyllodes tumors (87 benign, 37 borderline, and 19 malignant) and showed that the expression decreases with increasing degree of malignancy; however, the neoplastic stromal cells has decreased ER, and PR expression in all variants of phyllodes tumor. This can suggest a possible role of hormonal effect on tumor progression but limited role of endocrine therapy, since the stomal cells are the main neoplastic cells. 12
Conclusion
While metastatic breast phyllodes tumors to the lymph nodes are rare events, additional work-up (such as axillary staging) should be considered in patients with suspicious lymph nodes by imaging. Our case demonstrates that while malignant phyllodes tumors are rare, their implications for patient prognosis are extremely significant.
Acknowledgments
Dr. Sarah Alnaqshabandi, MD, Pathology, Clevelnad Clinic Main Campus, for her general support.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical Approval
Case report of deceased patient. No mentioning of patient identifications.