
Abstract

We present a biopsy specimen prepared from a 63-year-old female with a prolonged course of systemic lupus erythematous (SLE), who presented at the rheumatology clinic for clinical management. She initially experienced joint pain and stiffness; however, her symptoms grew more severe with musculoskeletal pain, serositis, chronic kidney disease, alopecia, and sicca symptoms. As part of the work up, the patient underwent routine screening mammography. Radiology demonstrated grouped, amorphous, coarse, and round calcifications in the right breast. The findings were classified as category BI-RADS 4 1 ; suspicious of malignancy, according to the Breast Imaging and Reporting and Data System, and a stereotactic core biopsy was performed.
Tissue sections prepared via hematoxylin and eosin (H&E) staining methodology yielded primarily fatty, inactive breast tissue. Upon deeper sectioning, amorphous eosinophilic material was identified, primarily in extracellular areas. The material architecturally formed large spheres or “secretion-like” deposits with centralized calcium phosphate (Figure 1A). Smaller spherical deposits were also identified in a perivascular fashion (Figure 1B). No material was seen within benign ducts or lobules.
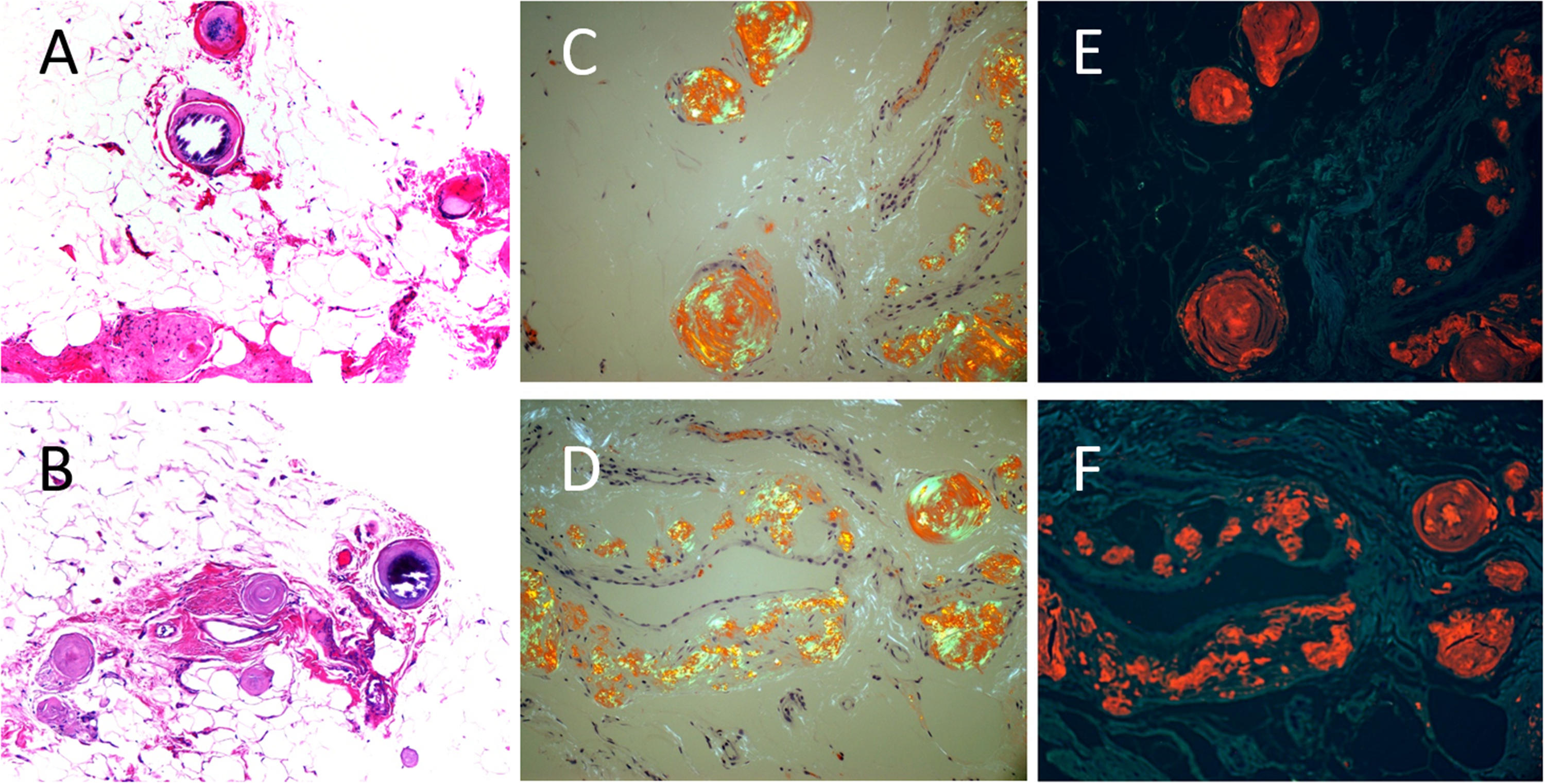
Microscopic images of breast amyloidosis. (A) and (B) Eosinophilic amorphous material seen as both extracellular spherical and perivascular deposits with centralized calcium phosphate. (C) and (D) “Apple-green birefringence” under polarized light microscopy. (E) and (F) Fluorescent microscopy utilizing a “Texas red filter.”
Congo red staining under polarized light microscopy showed a characteristic “apple-green” birefringence (Figure 1C-D). In this specimen, confirmation was achieved by using fluorescent microscopy with a “Texas red filter” on the Congo red stained tissue section. 2 Fluorescent microscopy enhances the diagnostic yield of Congo red as the amyloid fibrils demonstrate by the crimson appearance (Figure 1E-F). Unfortunately, there was insufficient material available for typing by mass spectrometry.
Stereotactic core biopsies are routinely performed for suspicious, grouped calcifications during screening routine mammography. The differential diagnosis includes invasive and in situ carcinoma and calcifications in benign breast glands and vessels. Amyloidosis of the breast is rare,3–7 which may present as grouped calcifications or a mass lesion. Amyloidosis is a clinical disorder in which deposition of amyloid fibrils in tissues leads to symptoms. For patients suspect with a suspicion of amyloidosis additional workup, including fat pad aspiration and possibly bone marrow examination, is required for diagnosis of systemic versus localized amyloidosis as well as amyloid typing. 8 In breast, localized amyloid deposition is more likely than systemic involvement and has an associated with extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT). There are multiple types of amyloidosis based on the type of protein and mechanisms of deposition. Type AL (or primary) is light chain associated and is related to plasma cell disorders. Type AA (or secondary) is associated with circulating inflammatory proteins and can be measured by serum amyloid A and predominately affects the kidneys and liver. Type TTR (or familial), is caused by unstable, mutant transthyretin, which is produced in the liver and generally affects the nervous system and heart. Lastly, type SSA (or senile system), primarily affects seniors and is associated with wild-type (i.e., normal) transthyretin proteins and generally affects the heart.
In modern pathology laboratories, Congo red is the preferred screening method for amyloidosis; however, deficiencies of polarized light microscopy are well documented. 9 The specificity of Congo red stain for amyloid via light microscopy is operator dependent. Common pitfalls include misinterpretation of collagen bundles within the mammary stroma, which appear as white fibers under polarization. These findings may be mistaken as amyloid, even by the most experienced pathologist. Thus, especially in patients without a medical history of amyloidosis, it is important to render a definitive diagnosis. Studies have shown fluorescent microscopy improves detection of amyloid in the evaluation of Congo red stained tissue sections,2,10 as seen in this patient.
This biopsy specimen is interesting because the patient had no documented history or clinical suspicion of amyloidosis. Additional staging biopsies for this patient were not performed. One must use caution before rendering a first-time diagnosis. Thus, confirmation using fluorescent microscopy was essential.
Footnotes
Author's note
Erinn Downs-Kelly, Laboratory Medicine and Pathology, Mayo Clinic, Scottsdale, AZ, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.