
Abstract
Background. Dermatopathic lymphadenopathy is a well-defined histopathological entity with an underestimated prevalence in the general population. Objective. The present study was conducted to analyze the characteristics of histologically diagnosed cases of dermatopathic lymphadenopathy at our unit. We also aimed to investigate any association between the clinical features of the patients and the histological findings. Methods. A total of 39 lymph node samples from 39 patients diagnosed with dermatopathic lymphadenopathy were included in this prospective cohort study. Results. Thirty-four (87%) patients had a dermatological disorder. The presence of paracortical eosinophils were significantly higher in patients with dermatological disorders (P = .001), while the presence of dilated sinuses was significantly more common in patients without a dermatological disorder (P = .035). The presence of dilated sinuses and medullary histiocytes were significantly more common in patients with lower body surface area involvement of the disease compared to the ones with a higher body surface area (P = .003, P = .034; respectively). Conclusion. Most of the patients included in the study had one of a broad spectrum of undiagnosed dermatological disorders. The clinical significance of the relation between histological and clinical findings in dermatopathic lymphadenopathy remains to be explained. Dermatopathic lymphadenopathy should always be considered in differential diagnoses of patients with persistent lymph node enlargement even when absolute dermatological disorders are not present. Since various skin disorders may be the cause of lymphadenopathy, performing a full-body examination before lymph node excision might prevent unneccessary procedures.
Introduction
Dermatopathic lymphadenopathy was first described by Pautrier and Woringer in 1937, 1 but the term was defined and published in English by Hurwitt in 1942. 2 Dermatopathic lymphadenopathy is a well-defined histological entity with an underestimated prevalence in the general population. 3 It is commonly associated with chronic skin diseases, presented as enlarged lymph nodes with paracortical hyperplasia, however in some cases the lymph nodes may remain at a normal size and may not be associated with other system disorders rather than skin diseases.3–5
Recently, the immunophysiology underlying the histological features of dermatopathic lymphadenopathy has been studied. Antigen-presenting dendritic cell subsets are found in both healthy and chronically inflamed skin, as well as in skin draining lymph nodes, suggesting that cutaneous Langerhans cells and other types of dendritic cells migrate to the T-cell-rich areas of regional lymph nodes where they mediate an appropriate immune response. Some researchers have hypothesized that ongoing antigenic stimuli with a subsequent local production of cytokines, such as tumor necrosis factor-alpha (which downregulates epithelial adhesion molecules facilitating migration), lead this migration to lymph nodes. 6
The present study was conducted to analyze the characteristics of histologically diagnosed cases of dermatopathic lymphadenopathy at our unit. We also aimed to investigate any association between the clinical features of the patients and the histological findings.
Materials and Methods
The study was reviewed and approved by the local ethics committee, and all the individual participants gave written informed consent. The study was carried out according to the principles expressed in the Declaration of Helsinki.
A prospective cohort study was planned to evaluate the clinical and histological features of patients diagnosed with dermatopathic lymphadenopathy. The study cohort included 39 lymph node samples from 39 patients. The lymph nodes showing the following features were excised: (1) the lymph nodes that are 1.5 cm or larger in the longest transverse diameter or (2) firm, irregular, clustered, or fixed nodes regardless of size. 7 After phyisical examination ultrasonographic examination of the lymph nodes and abdomen (to rule out hepatosplenomegaly) was performed in all patients.
The histopathological examination of the lymph nodes was made at the Department of Pathology at University of Health Sciences Umraniye Training and Research Hospital from September 2019 through March 2020. The patients histopathologically diagnosed with dermatopathic lymphadenopathy were invited to the Department of Dermatology. For each patient, age, sex, clinical diagnosis, symptoms, systemic diseases, findings of physical examination, and results of laboratory investigations and histological findings were recorded. Patients with a history or diagnosis of any systemic viral, bacterial, or parasitic infections within the past 2 months and patients with hepatosplenomegaly that was confirmed by radiological examination were not included.
Histological Evaluation
Lymph nodes consistent with the diagnosis of dermatopathic lymphadenopathy according to Gould et al 8 were included in this study. Dermatopathic lymphadenopathy was morphologically defined as an expansion of lymph node paracortical areas by a mixed cellular infiltrate, including lymphocytes and dendritic cells, the latter with elongated, delicately folded, or twisted nuclear contours and abundant pale eosinophilic cytoplasm. 5 Paracortical eosinophils, neutrophils, plasma cells, histiocytes, medullary eosinophils, histiocytes, pigmented cells, plasmocytosis in medullary cords, dendritic langerhans cells, CD1a+ histiocytes, dilated sinuses, atrophic follicles were quantified as the average numbers in 10 high power fields (400×) and classified as 0 (absent), 1+ (mild, 1-3 per high power field), 2+ (moderate, 4-5 per high power field), and 3+ (severe, >5 per high power field).
Hematoxylin and eosin (H&E)-stained slides were obtained from formalin-fixed, paraffin-embedded tissue sections, including 39 excisional biopsy specimens of lymph nodes with dermatopathic lymphadenopathy. immunohistochemical CD20, CD3, Ki67, and CD1a staining was also performed for all samples. All the lymph node specimens were reviewed by one author.
Statistical Analysis
Statistical analyses were carried out using the R Core Team (2013) version 2.15.3. The descriptive data were expressed with mean ± standard deviation, numeric variables, frequency, and percentages. In the analysis of normally distributed variables, a Shapiro-Wilk test was applied to examine the differences between the 2 groups. The differences between the 2 independent groups were examined using the nonparametric Mann-Whitney U test for the non-normally distributed variables. Pearson chi-square test, Fisher's exact test and Fisher-Freeman-Halton exact test were used to compare qualitative variables. P < .05 was considered statistically significant.
Results
Clinical Features
The study group included 23 women and 16 men with a median age of 40.26 ± 13.1 years (range 20-69). The clinical and histological features are summarized in Table 1.
Clinical and Demographic Features of the Patients.
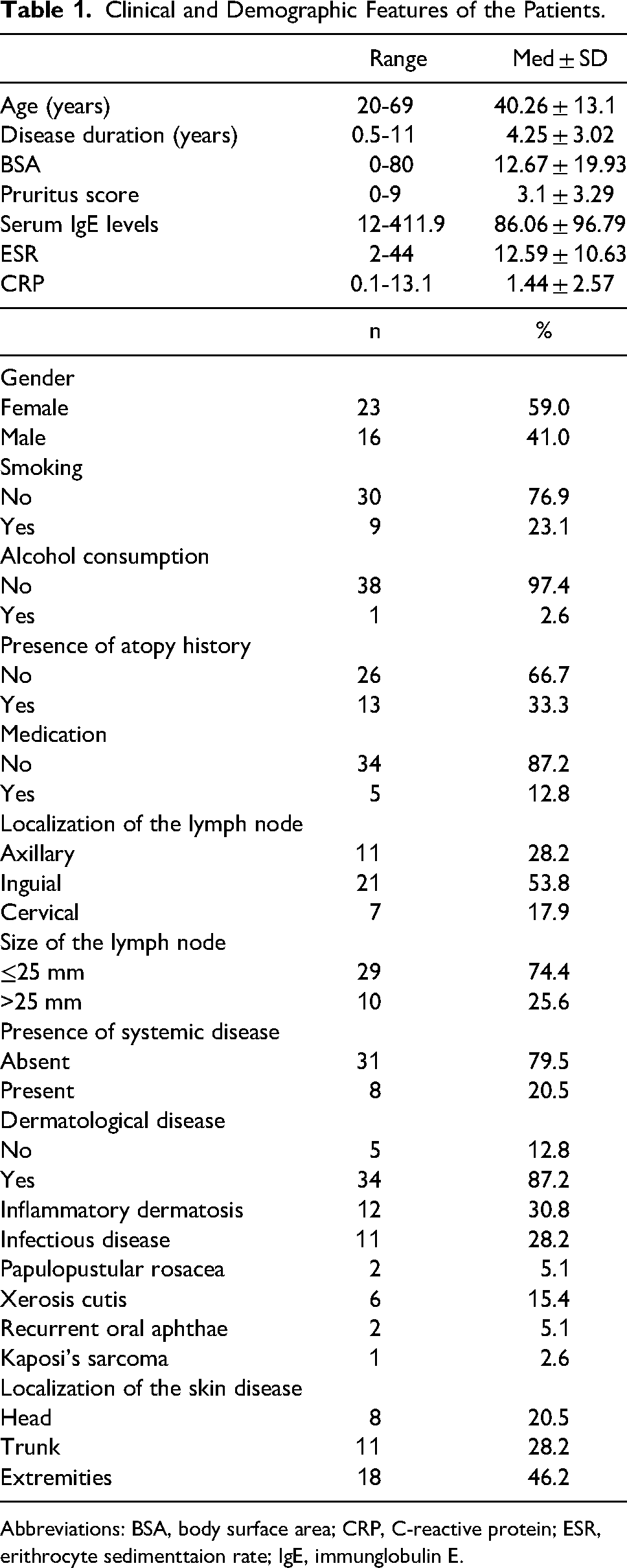
Abbreviations: BSA, body surface area; CRP, C-reactive protein; ESR, erithrocyte sedimenttaion rate; IgE, immunglobulin E.
All 39 patients had lymph node enlargement in only one area which was confirmed ultrasonographically. Thirty-four (87%) patients had a dermatological disorder, including xerosis cutis (n = 9), atopic dermatitis (n = 4), psoriasis (n = 3), seborrheic dermatitis (n = 3), dermatitis (n = 1), rosacea (n = 2), folliculitis (n = 2), recurrent oral aphthae (n = 2), tinea pedis (n = 1), prurigo simplex (n = 1), Kaposi's sarcoma (n = 1), and syphilis in a patient with human immunodeficiency virus (HIV) infection (n = 1). Five (13%) patients did not have dermatological manifestations, including 1 with prostate carcinoma and 1 with pancytopenia.
The lymph node biopsy specimens were inguinal in 21 (54%), axillary in 11 (28%), and cervical in 3 (8%) patients. Lymphadenopathy was unilateral in all the patients.
In patients with a history of dermatological disorders, the median interval from the onset of dermatological manifestations to the detection of dermatopathic lymphadenopathy was 4.25 ± 3.02 months (range 0.5-11 months). Radiologically, the maximal diameter of the largest lymph node was larger than 2.5 cm in 10 (26%) patients, while it was equal to or smaller than 2.5 cm in 29 (74%) patients.
Histological Features
All the lymph nodes showed expanded paracortical regions from a mixed cellular infiltration that included lymphocytes, variably sized aggregates of dendritic cells, and occasional macrophages. Examples of lymph node examinations are shown in Figures 1 to 4.
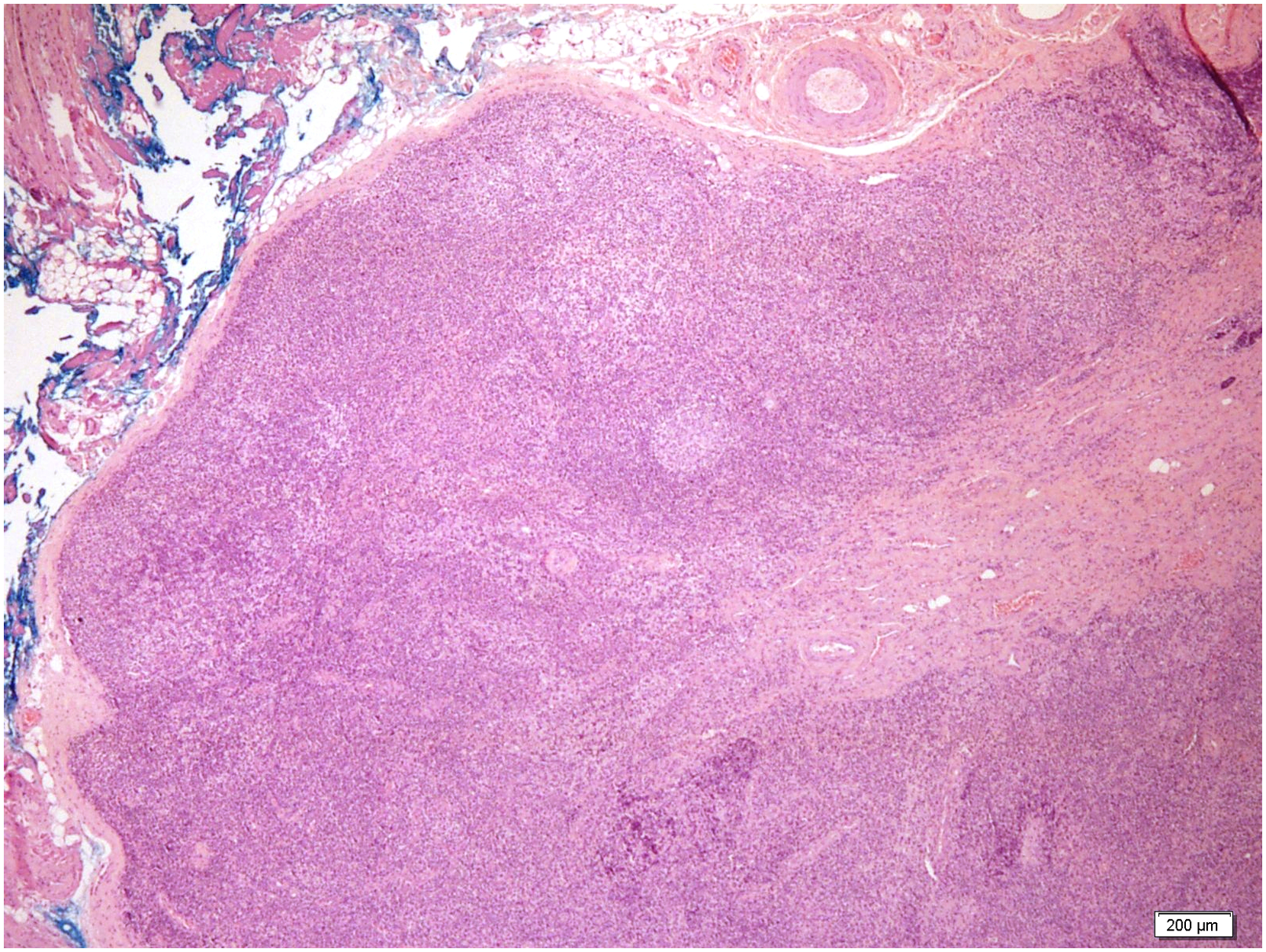
Enlarged lymph nodes (hematoxylin & eosin staining,×40).
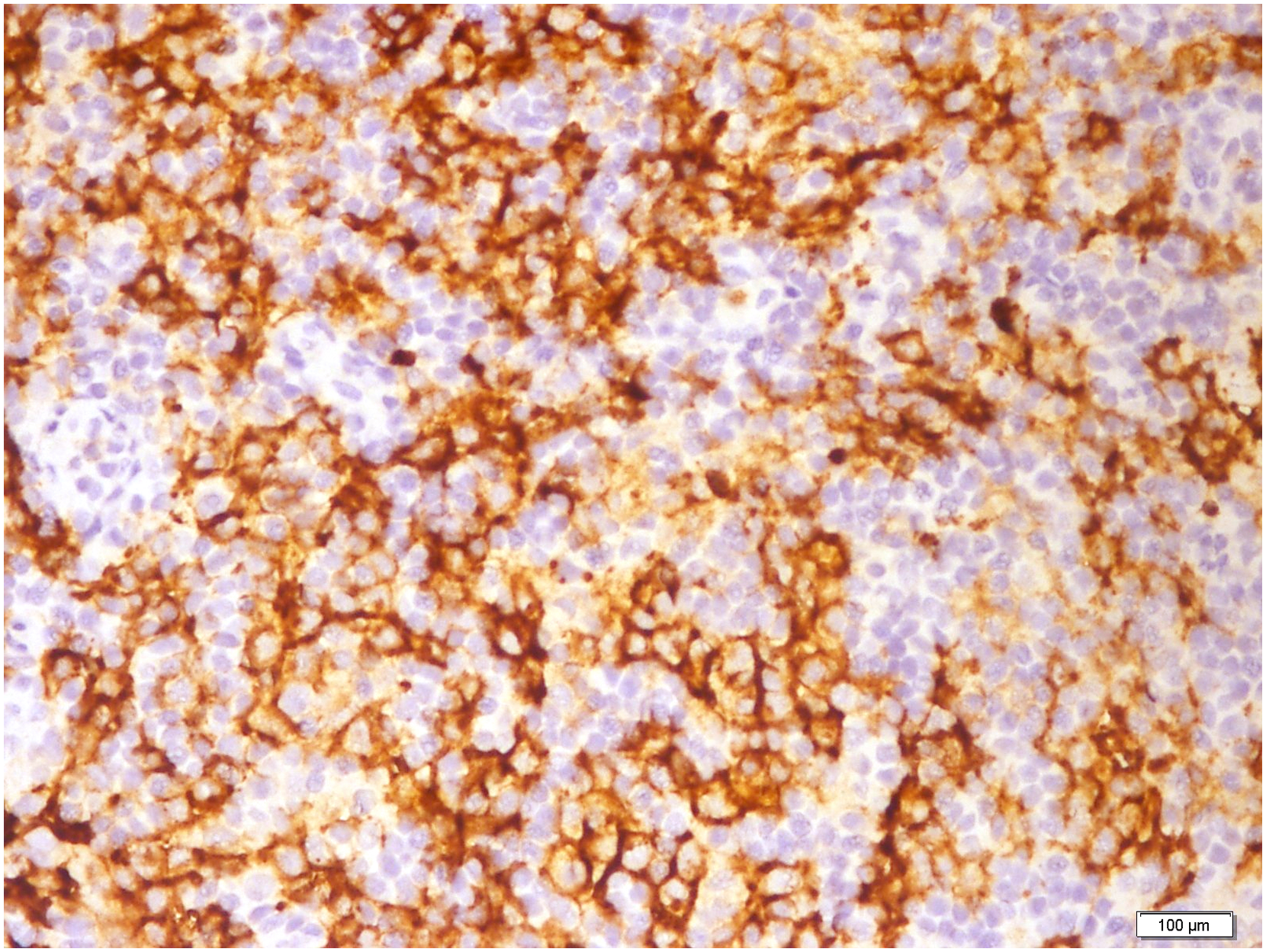
CD1a positive membranous staining in Langerhans cells.
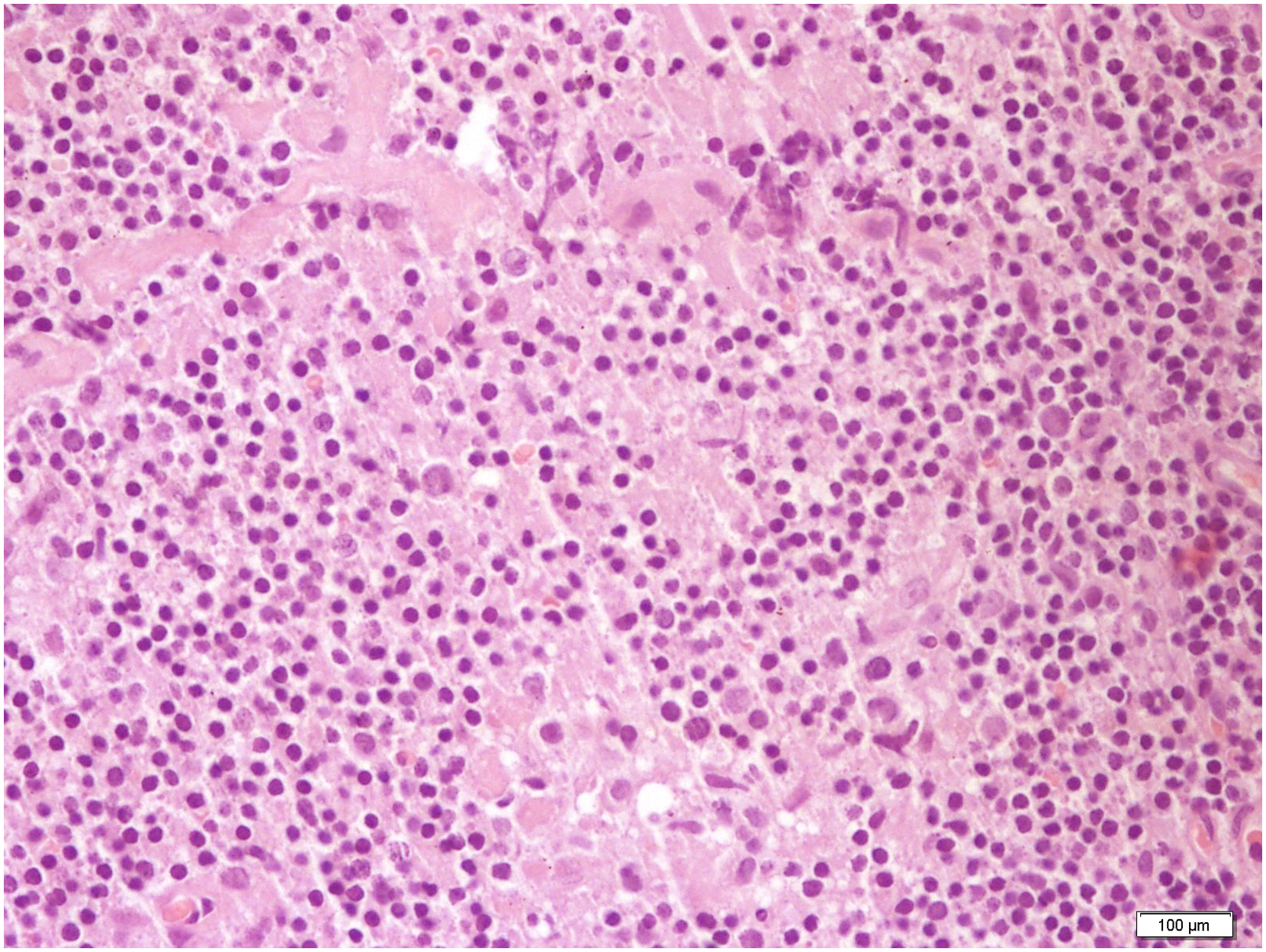
Pale, large Langerhans cells (hematoxylin & eosin staining,×400).
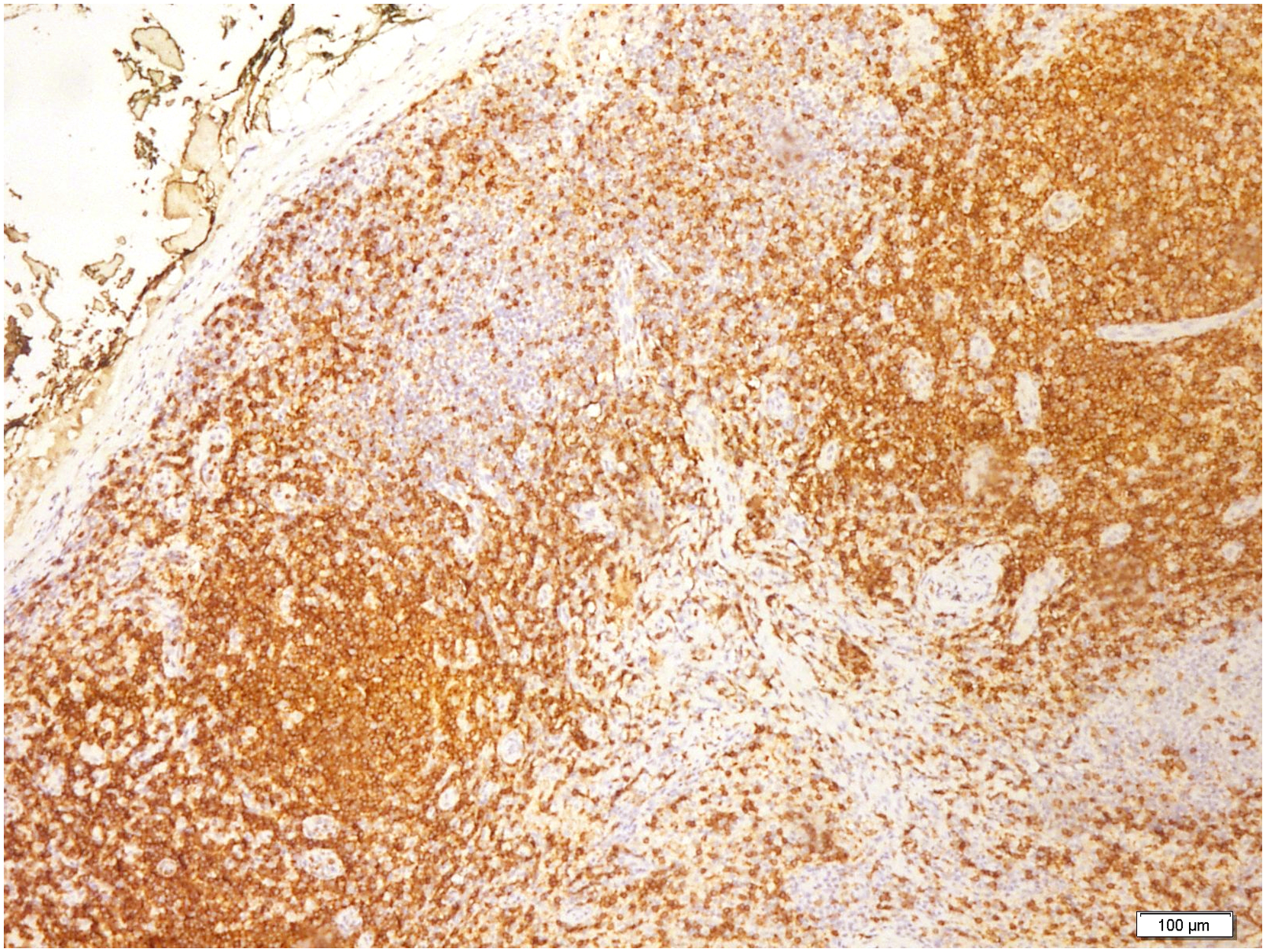
Hyperplasia in paracortical T cells (CD3 staining,×100).
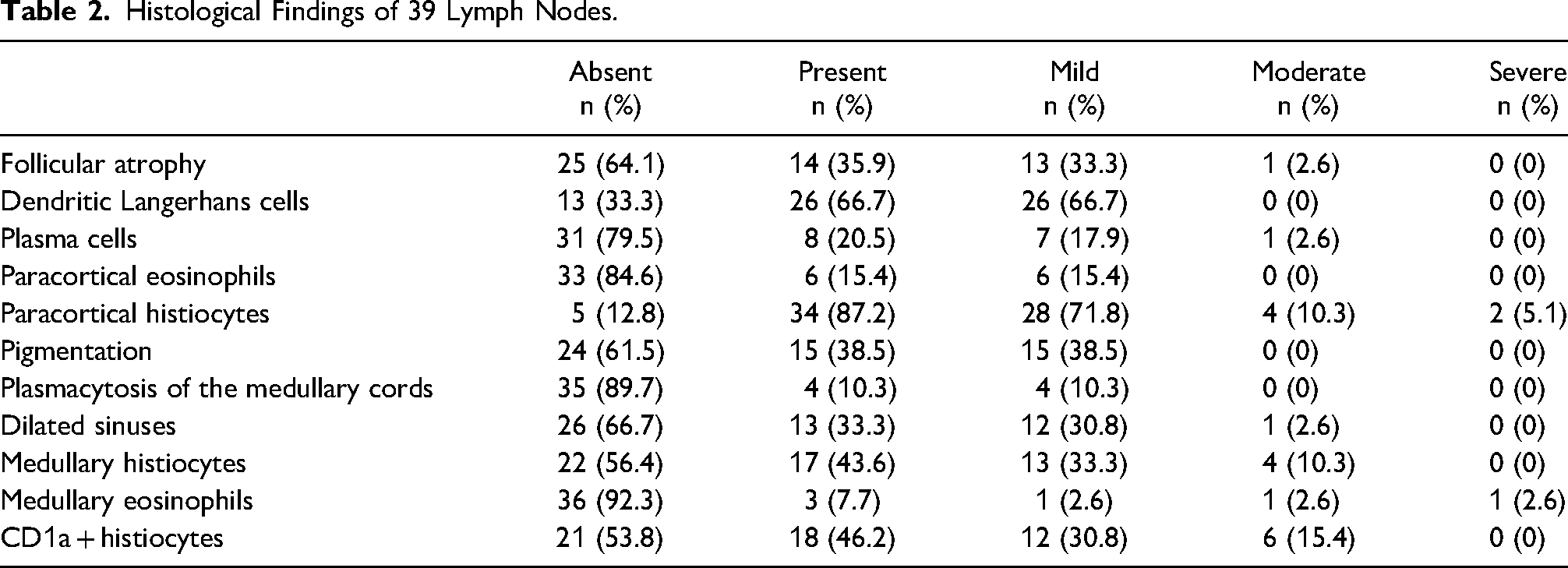
Follicular atrophy was observed in 14 (36%) cases, 13 were mild and 1 moderate. Dendritic Langerhans cells were noted in 26 (67%) cases, all showing mild infiltration. Paracortical eosinophils were present in 6 (15%) lymph node samples, and all were classified as mild. Medullary eosinophis were observed in 3 (8%) of the specimens, including 1 mild, 1 moderate, and 1 severe infiltration. In 8 (21%) lymph nodes, plasma cells were a part of the paracortical cellular infiltrate, including 7 mild and 1 moderate cases. In addition, 34 (87%) of the lymph nodes showed paracortical histiocytes, 28 mild, 4 moderate, and 2 severe. Medullary histiocytes were observed in 17 (44%) of the lymph nodes, 13 with mild and 4 with moderate infiltration. Pigmentation was present in 15 (39%) lymph nodes, all with a mild presentation.
Mild plasmacytosis of the medullary cords was observed in 4 (10%) lymph nodes. Thirteen (33%) lymph nodes showed dilated sinuses, 12 were mild, and 1 was moderate. Eighteen (46%) lymph node specimens showed positive staining for CD1a. None of the lymph nodes showed giant cells, granulomas, areas of necrosis, or overt morphological evidence of lymphoma involvement.
A summary of the histological features of 39 lymph nodes with dermatopathic lymphadenopathy is provided in Table 2.
Histological Findings of 39 Lymph Nodes.
Correlation Between Clinical and Histological Findings
The correlation between the clinical and histological findings is summarized in Table 3. The presence of follicular atrophy was more common in patients under medication compared to those who did not use any medication (P = .047). The presence of paracortical eosinophils was statistically significantly higher in patients with dermatological disorders (P = .001) and particularly in those with papulopustular rosacea (P = .02), while no significant difference was observed in any other dermatological condition in terms of the presence of paracortical eosinophils (P > .05).
Correlation Between Clinical and Histological Findings.
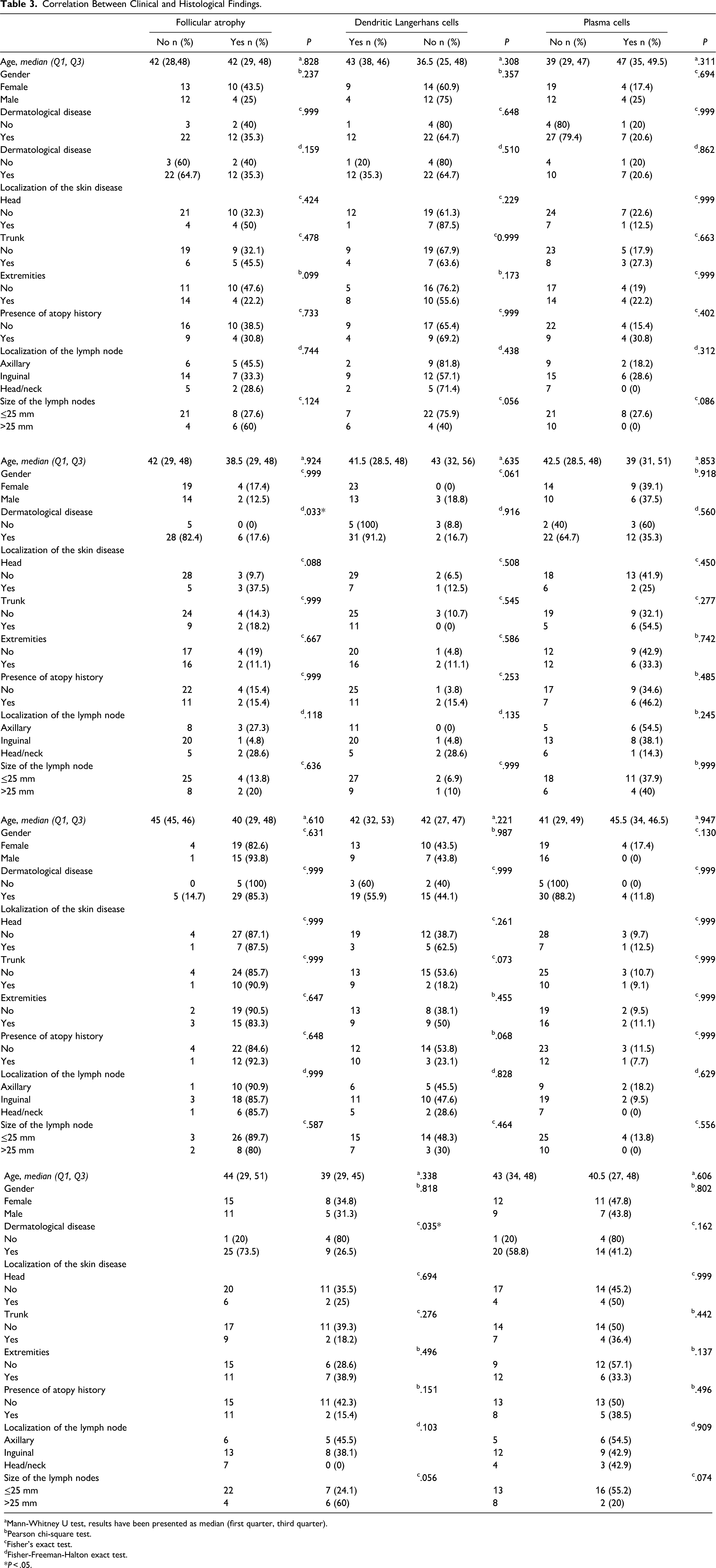
Mann-Whitney U test, results have been presented as median (first quarter, third quarter).
Pearson chi-square test.
Fisher's exact test.
Fisher-Freeman-Halton exact test.
*P < .05.
The presence of dilated sinuses was statistically significantly more common in patients without dermatological disorders (P = .035) and in those with lower body surface area involvement of the disease compared to the ones with higher body surface areas (P = .003). Additionally, the presence of dilated sinuses was statistically significantly more common in patients with lower pruritus scales than in the higher ones (P = .021).
The presence of medullary histiocytes were statistically significantly lower in patients with xerosis cutis (P = .027), while no significant differences were observed in any other dermatological condition in terms of the presence of medullary histiocytes (P > .05). The presence of medullary histiocytes was statistically significantly more common in patients with lower body surface area involvement of the disease compared to the ones with higher body surface areas (P = .034).
Discussion
A total of 39 patients with lymph node enlargement (cervical, axillary, inguinal) were included in this study. Thirty-four patients had a dermatological disorder (including xerosis cutis, atopic dermatitis, psoriasis, seborrheic dermatitis, dermatitis, rosacea, folliculitis, recurrent oral aphthae, tinea pedis, prurigo simplex, Kaposi’s sarcoma, and syphilis in a patient with HIV infection), while 5 patients did not have dermatological manifestations, including 1 with prostate carcinoma and 1 with pancytopenia. The most common histological finding was paracortical histiocytes, followed by dendritic Langerhans cells, medullary histiocytes, pigmentation, follicular atrophy, dilated sinuses, paracortical plasma cells, paracortical eosinophils, plasmacytosis of the medullary cords, and medullary eosinophils. The presence of paracortical eosinophils was statistically significantly higher in patients with a dermatological disorder and particularly in those with papulopustular rosacea. The presence of medullary histiocytes was statistically significantly lower in patients with xerosis cutis. Dilated sinuses and medullary histiocytes were more common in patients without a dermatological disorder and in those with lower body surface areas. The presence of follicular atrophy was more common in patients under medication compared to those who did not use any medications.
Dermatopathic lymphadenopathy is a rare, distinctive type of benign lymph node reaction that is associated with cutaneous lesions. All the lymph nodes may be involved, while inguinal and axillary lymph nodes are the most common involvement sites. The involved lymph nodes are moderately enlarged, firm, mobile, and painless.8,9 The diagnosis of dermatopathic lymphadenopathy is histologically made by demonstrating interfollicular and paracortical hyperplasia of lymph nodes from the infiltration of interdigitating dendritic cells (IDCs), Langerhans cells, macrophages, and T cells. Melanin granule-laden macrophages are often scattered in these lymph nodes. The lymph nodes on the drainage sites of the cutaneous disease are usually affected.8,10 Slightly expanded germinal centers surrounded by lymphocytes and a widened paracortical area are the characteristic findings. The follicular pattern is preserved. An expanded paracortical area and pale staining due to the presence of Langerhans cells and, in particular, interdigitating dendritic cells are the other pathagnomic features. Although macrophages are a minor component, they are characteristic due to the cytoplasmic pigment (mostly melanin, some hemosiderin) that they contain.3,11 The histological differentiation of dermatopathic lymphadenopathy from lymphoproliferative disorders is crucial. 4
Differential diagnosis of dermatopathic lymphadenopathy includes Hodgkin lymphoma, mycosis fungoides/Sezary syndrome, infectious lymphadenopathy including bacterial and viral and melanoma. Hodgkin lymphoma-associated lymphadenopathy is characterized with Hodgkin/Reed Sternberg cells and lack of proliferation of Langerhans cells and interdigitating dendritic cells provides the differentiation. In case of lymph node involvement in mycosis fungoides/Sezary syndrome T-cell clones and abnormal T-cell phenotypes are found in the lymph node. Lymphadenopathy caused by melanoma metastasis is characterized by nuclear atypia in melanocytes in contrast to histiocytes in dermatopathic lymphadenopathy. In viral lymphadenopathy absence of pale staining nodular proliferation of interdigitating dendritic cells and Langerhans cells is observed while infiltration of neutrophil leukocytes and macrophages, suppurative foci are present in bacterial lymphadenopathy. In each condition clinical findings also provide differential diagnosis.12–18
Among with other viral infections, HIV may cause lymphadenopathy. The most common histological pattern in HIV-associated lymphadenopathy is florid follicular hyperplasia, followed by depletion of CD4+ positive cells. The histological pattern may show various features and may not be specific. 19 Although it is not commonly reported, dermatopathic lymphadenopathy may be associated with HIV infection and immunohistochemistry should be considered for a definitive diagnosis. 20 In this study, a case of HIV-positive patient was diagnosed as dermatopathic lymphadenopathy due to histological and immunohistochemical findings.
Immunohistochemistry may provide the accurate diagnosis of dermatopathic lymphadenopathy as well as differential diagnosis of other causes of lymphadenopathy. S100 protein, CD1a and langerin which are expressed by the dendritic cells are the typical and mostly studied markers, while other markers such as T-cell antigens (CD4 and CD8), histiocyte markers (CD163 and lysozyme), and Ki67 (showing proliferation rate) may also be studied. 6 In this study CD20, CD3, Ki67, and CD1a were studied in all cases. Morphological and immunohistochemical examination of all the lymph nodes showed reactive pattern. CD3 positivity indicated paracortical t zone hyperplasia, CD20 indicated follicular centers, Ki67 showed polarized proliferation in germinal centers, CD1a indicated Langerhans cells. In metastatic cancers infiltration of subcapsular part of the lymph nodes is observed while Langerhans cells primarily present as enlarged layer in cortex, enlarging to medulla.
Dermatopathic lymphadenopathy occurs in association with various skin disorders, including infections (tuberculosis, fungal infections human immunodeficiency virus infection, and toxoplasmosis), inflammatory skin disorders (erythrodermas, psoriasis, and atopic dermatitis), skin irritation, or many other disorders, such as sarcoidosis, lymphoproliferative issues, tumor metastases, toxic shock syndrome, pemphigus, neurodermatitis, and atrophia cutis senilis. 11 However, dermatopathic lymphadenopathy in patients without active cutaneous disorders is also reported.7,9 It has also been reported that dermatopathic lymphadenopathy is more common in patients with extensive skin involvement. 3
In a large series of consecutive lymph node biopsy specimens, dermatopathic lymphadenopathy was detected in 4.8% of specimens with a male predominance; in the study, most of the patients had a skin disease, while 12% of the patients had no findings of a skin disease. 9 In another study evaluating 1000 axillary lymph nodes from 50 consecutive radical mastectomy specimens performed in women with breast cancer, 15% of the lymph nodes showed mild to moderate dermatopathic changes, with only 1 patient having a cutaneous disease (contact dermatitis). 11 Additionally, the authors reported that mild dermatopathic changes did not correlate with skin disease, and a finding of dermatopathic lymphadenopathy may be indicative of a healed skin disorder. 12
Dermatopathic lymphadenopathy is also a common reaction pattern in patients with mycosis fungoides and Sezary syndrome. Palpable lymphadenopathy is present in 75% of patients with mycosis fungoides/Sezary syndrome at the time of diagnosis; this lymphadenopathy may be dermatopathic or involve mycosis fungoides/Sezary syndrome or a mixture of both. It should be noted that distinguishing between dermatopathic lymphadenopathy and the early stages of mycosis fungoides/Sezary syndrome involvement is not always possible. Mycosis fungoides/Sezary syndrome patients with lymphadenopathy have a poorer prognosis compared to those without lymphadenopathy, regardless of the histological findings (ie, dermatopathic lymphadenopathy vs mycosis fungoides/Sezary syndrome). 21 Additionally, the presence of mycosis fungoides in patients with dermatopathic lymphadenopathy is associated with a poor prognosis. 3
With these data, close follow ups and several visits are crucial to exclude the development of lymphoproliferative disorders and/or mycosis fungoides/Sezary syndrome, particularly in cases without clear clinical diagnoses. 3 Fortunately, none of our patients developed any lymphoproliferative disorders after the detection of dermatopathic lymphadenopathy, they are still on annually scheduled follow-up program.
In this study, certain characteristics of dermatopathic lymphadenopathy were found to be statistically associated in some conditions, for example, presence of paracortical eosinophils was higher in patients with rosacea, or the presence of medullary histiocytes were lower in patients with xerosis cutis. However, it is not possible to make conclusion with such limited study population.
In the present study, a total of 39 patients with lymph node enlargement (cervical, axillary, and inguinal) were included, with a female predominance. Interestingly, all the patients were referred to another department due to lymph node enlargement, and after histological examinations of the lymph nodes resulted in dermatopathic lymphadenopathy diagnoses, they were referred to the dermatology department. Most of the patients had one of a broad spectrum of dermatological disorders. Only 5 patients did not have dermatological manifestations, including 1 with prostate carcinoma and 1 with pancytopenia. Among the histological findings, the association between the presence of paracortical eosinophils and any dermatological disorder, particularly papulopustular rosacea, and the association between the presence of medullary histiocytes and xerosis cutis was remarkable. However, the clinical significance of these findings remains to be explained.
In conclusion, dermatopathic lymphadenopathy should always be considered in differential diagnoses of patients with persistent lymph node enlargement, even when absolute dermatological disorders are not present. Additionally, it should be kept in mind that various skin disorders may be the cause of lymphadenopathy. Keeping this in mind might prevent unneccessary lymph node excisions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was reviewed and approved by the local ethics committee.
Informed Consent
All the individual participants gave written informed consent.
Trial Registration
Not applicable.