
Abstract
Recent years have seen the recognition and establishment of numerous subtypes of renal cell carcinoma (RCC), including adoption of an entire category of “molecularly defined renal carcinomas” in the fifth Edition of World Health Organization Classification. To add value, new diagnostic entities should be clinicopathologically distinct, or better, imply specific management and treatment angles, especially if adjunctive testing is needed for diagnosis. One such promising future treatment angle for a molecularly defined subtype, TFEB-amplified RCC, is immunotherapy, for which recent scholarship has demonstrated frequent expression of PD-L1. Herein, we report a case of metastatic TFEB-amplified RCC, where the patient experienced a long-term, complete response to PDL1-directed therapy, which had been serendipitously used years ago under a renal tumor subtype-agnostic indication. This promising experience suggests formal exploration of immunotherapy for these tumors.
Case Report
One of the drivers in the evolution of classification of renal cell carcinoma (RCC) over time has been the observation, starting around the turn of the millennium, that histologic classification predicts prognosis in this disease. 1 More recently, developments in therapy have further supported the classification of RCC into histopathologic subtypes, which map to specific treatment regimens. 2 The most recent trend in the classification of RCC, evident in the fifth Edition of World Health Organization Classification, 3 is that of a group of “molecularly defined renal carcinomas,” which encompasses seven subtypes of varying clinical and biological potential. These range from subtypes with strong hereditary associations, such as fumarate hydratase and succinate dehydrogenase-deficient RCCs, to two groups of RCCs defined molecularly by alterations of the micro-opthalmia transcription factor family transcription factors, TFE3 and TFEB. In the case of TFEB, the subtype is further complicated by groups harboring either (or rarely, both) rearrangement and amplification involving this locus, such that the overall category is designated TFEB-altered RCCs. TFEB-rearranged RCCs tend to occur in younger patients, with a median age in the fourth or early fifth decade, while TFEB-amplified RCCs occur in older patients with a median age in the seventh decade.4,5 Moreover, TFEB-amplified RCCs tend to show more aggression, with the presentation at higher stage or with metastasis.3,6
In light of recent scholarship, functionally implicating TFEB itself as a mediator of immune evasion through induction of PDL1 expression, 7 as well as observations of PDL1 expression in TFEB-altered RCCs,8,9 including most recently TFEB-amplified RCCs, 10 we performed retrospective searches of institutional pathologic databases, with the goal of characterizing PDL1 expression in our patient population. Unexpectedly, we identified one previously “unclassified RCC” case, which we would now reclassify as a TFEB-amplified RCC, where the patient was serendipitously and successfully treated using PDL1-directed therapy. To our knowledge, this represents the first-ever report of a long-term, complete immunotherapy response of an aggressive TFEB-amplified RCC. We describe the case as follows, with hopes of providing, retrospectively, support for both the potential value of the increasingly complex classification of RCC, as well as to spur investigation of this promising therapeutic angle for an aggressive group of tumors.
The 48-year-old patient (reported previously, within a large series
11
) had presented for nephrectomy for an incidentally-encountered 9.5 cm right renal mass, over 8 years ago (Figure 1a and b). Upon resection, the tumor evinced difficult-to-classify histology (Figure 1c and d

(a) Coronal contrast-enhanced CT-scan, demonstrates a 9.5 cm renal mass. (b) Macroscopically, the tumor was solid and cystic, hemorrhagic and fleshy and tan-yellow. (c) Histologically, the tumor was solid and cystic at low power. (d) Variable tubulopapillary growth was present, with mostly nuclear features in the WHO grade 3 range. (e) Several areas demonstrated incipient necrosis, inflammatory infiltration and grade 4 nucleolar features; focal Melan A expression was evident immunohistochemically (inset), triggering additional workup.
Then, at 30 months postoperatively, nivolumab 240 mg IV every 2 weeks was initiated, under the drug's already extant US FDA approval for advanced RCC of any histology progressing after anti-angiogenic therapy. After 12 weeks of nivolumab therapy, restaging scans were initially non-reassuring, questionable for progression versus pseudoprogression. Toxicity related to nivolumab therapy included a grade I colitis, treated with prednisone. Yet, over the course of the ensuing year, the patient reported remarkable clinical improvement, and restaging scans first documented stable disease, then mixed responses including resolution of thoracic disease, and then, by 20 months a substantial decrease in the size of the larger abdominal deposits. At 24 months, nivolumab was discontinued after interdisciplinary review deemed the patient to have a near complete response to therapy, including both the tumor bed recurrence and smaller metastases, comparing pre-treatment and post-treatment contrast CT-scans (Figure 2a–d). This interpretation was further supported by scans from subsequent years, including at 36 and 48 months from initiation of nivolumab, when restaging scans again demonstrated no active disease, off therapy. The patient remains free of disease, under observation, over 98 months after initial diagnosis. Retrospectively, though not presently required as a companion diagnostic for nivolumab or pembrolizumab indications for RCC, we performed a PDL1 immunostain on this patient's tumor (Figure 2e and f), which demonstrated diffuse expression, overall in the range of what would be in keeping with a combined positive score (CPS) of ∼75, a range similar to that reported for TFEB-amplified RCCs recently. 10
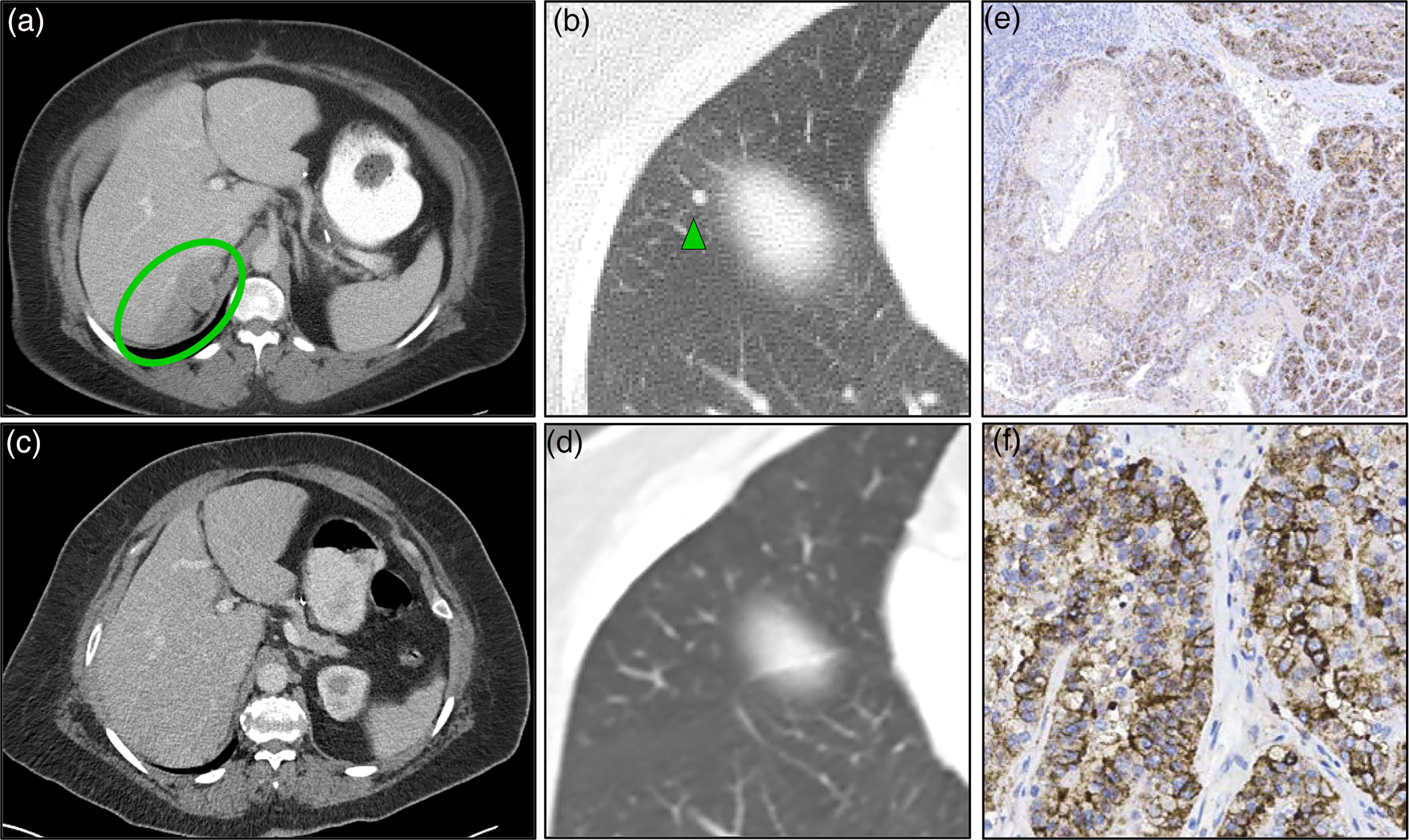
(a) Representative transverse contrast computed tomography (CT)-scan demonstrating a multinodular soft tissue mass in the superior aspect of the surgical bed, documenting local recurrence (green, area of interest), before initiation of therapy. (b) Representative transverse contrast lung CT scan showing an 8 mm metastatic nodule (green arrowhead), one of several lung metastases. (c) 48 months post-treatment CT scan at the approximate same level as panel (a), showing complete resolution of the surgical bed recurrence. (d) 48 months post-treatment contrast lung CT at the same level as panel (b), interpreted as complete response. (e) Though not performed at the time of therapy initiation (or currently indicated as a companion diagnostic for PDL1 agents in RCC), a PDL1 immunostain (clone 22C3), was preformed retrospectively, demonstrating diffuse expression estimated as a CPS of 75, at intermediate magnification. (f) Diffuse membranous and variable cytoplasmic expression is apparent at higher power.
Overall, our experience with this case, taken with growing experience documenting frequent expression of PDL1 in RCCs related to MiT family transcription factor alterations8,10,15 supports investigation of nivolumab and related therapies for aggressive cases of these tumor types. The recent fifth Edition of WHO Classification's 3 unification of these tumors under the rubric of TFEB-altered RCC should enable recognition and risk assessment of these tumors, especially as molecular testing for TFEB status, whether by FISH or Next-Gen sequencing methods 16 has become more widely available. Moreover, we hope that our serendipitous but long-term retrospective experience with this case illustrates the potential of integrative diagnostic surgical pathology to support precision therapy for RCC patients. In short, we have progressed from an unclassified tumor, with a unique but incidental molecular finding, to supporting an investigational treatment target in only a few years.
Footnotes
Acknowledgements
SCS discloses consulting and royalty income from Amirsys/Elsevier Publishing that does not pose a conflict of interest with regards to the foregoing manuscript and findings.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Appropriate approval was obtained RAMS-IRB (HM20002545).
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.