
Abstract
We present a case report of a 54-year-old male with a metastatic testicular sex cord tumor harboring a EWSR1::ATF1 gene fusion. The tumor displayed a solid and nested architecture with sclerotic stroma and variable inflammatory infiltrate, and was positive for SF-1, inhibin, EMA, CD30, and WT1 expression. Further genetic analysis identified a EWSR1::ATF1 gene fusion. Overall findings were consistent with an “inflammatory and nested testicular sex cord tumor,” a recently described testicular neoplasm characterized by EWSR1::ATF1 gene fusion and aggressive clinical behavior. Due to the aggressive nature of this entity and the limited response to current treatment options available, identification of potential biomarkers for early diagnosis and targeted therapies are critical. This case report provides important insights into the genomic landscape of testicular sex cord-stromal tumors, especially within the CTNNB1-negative subset of patients with an aggressive clinical course, and further supports the distinction of “inflammatory and nested testicular sex cord tumor” as a separate entity from Sertoli cell tumors due to its characteristic morphological, immunohistochemical and molecular, features and clinical behavior.
Introduction
Testicular sex cord-stromal tumors are rare neoplasms, accounting for ≤5% of all testicular tumors.1,2 The most common sex cord-stromal tumor subtype is the Leydig cell tumor, which represents approximately 75% of sex cord-stromal tumors, followed by the Sertoli cell tumor as the second most common. Other sex cord-stromal tumors include granulosa cell tumors, tumors in the fibroma thecoma group, mixed, and other sex cord-stromal tumors.2,3 These tumors pose a great diagnostic challenge in testicular pathology, because of their immunophenotypic characteristics and similarities between them. 3 The majority of sex cord-stromal tumors are indolent, but metastasis can occur even in tumors with relatively bland histology, posing challenges in predicting aggressive behavior in non-metastatic tumors.
Sertoli cell tumors comprise <1% of testicular tumors in children and adults and represent approximately 30-40% of all sex cord-stromal tumors.3,4 These may occur at any age, with a peak frequency between 35 and 50 years of age. 2 This entity usually presents as an incidentally identified unilateral testicular mass, and less commonly patients may present with gynecomastia. 5 Metastasis as the first presentation has been rarely described, and it is reported to occur in about 7% of the cases.2,5 To date, there are few studies investigating the molecular and genetic abnormalities found in testicular sex cord-stromal tumors. Recent reports indicate that many Sertoli cell tumors show CTNNB1 gene mutations and nuclear positivity for ß-catenin is demonstrated in nearly 60% of the cases, however, they do not necessarily correlate with an aggressive clinical course.6,7 Other genetic abnormalities seen in Sertoli cell tumors include a gain of X chromosome and complete or partial losses of chromosomes 2 and 19. 8
Recently, a distinct group of malignant testicular sex cord tumors initially classified as Sertoli cell tumors or as seminomas, were identified to harbor recurrent EWSR1::ATF1 fusions. Based on their distinct morphological, immunohistochemical, molecular, and clinical characteristics, the authors proposed to classify these tumors as a separate entity, introducing the term “inflammatory and nested testicular sex cord tumor.” 9
Herein, we report a case of a testicular sex cord tumor with lung metastasis at presentation, that was initially favored to be a metastatic Sertoli cell tumor but was later identified to harbor a EWSR1::ATF1 gene fusion; consistent with the recently proposed term “inflammatory and nested testicular sex cord tumor.”
Materials and Methods
Immunohistochemistry
Formalin-fixed paraffin-embedded (FFPE) sections from the lung biopsy specimen were cut at 4-micron thickness, and deparaffinized in Ventana EZ prep solution/Leica Dewax at 72°C for 16 min. The slides were then subjected to antigen retrieval in Ventana cell conditioning (CC1) solution/Leica ER1ER2 epitope retriever at 96°C for 36 min. Following this, the sections were blocked for non-specific binding of antibodies by incubating with goat Ig block at room temperature for 8 min. This was followed by incubation of the primary antibodies, with dilutions, vendors, and clones as reported in Table S1, at room temperature for 32 min. After rinsing, the autostainer performs Ventana Ultraview universal and optiview/Leica BOND polymer detection kit DAB detection procedure, which includes successive incubation with DAB inhibitor (3% H2O2) horseradish peroxidase-linked anti-mouse multimer, DAB chromogen, and substrate and copper enhancer. The procedure results in brown precipitation. This is followed by counterstain with one drop of hematoxylin for 8 min and one drop of bluing reagent for 4 min. The slides are removed from the autostainer, washed in water with dishwashing detergent, and mounted as per IHC standard operating protocols. All glass slides were reviewed and interpreted by a board-certified pathologist.
Molecular Genetic Testing
Molecular genetic testing using targeted next-generation sequencing (NGS) with the HopeSeq Solid Tumor Comprehensive platform targeting DNA (523 genes panel) to detect SNVs, copy number variants, fusions, microsatellite instability (MSI), and tumor mutation burden (TMB); and RNA sequencing platform (165 genes panel) to detect fusions with unknown gene partners was performed. DNA assay was performed using the Illumina TruSight™ Oncology 500 (TSO500) targeted hybrid-capture NGS method and sequenced on the Illumina NextSeq 550 instrument, and data were analyzed using the TSO Local Run Manager (LRM) software, CLC Genomics Workbench software, and QCI Interpret web-based software application. The TMB and MSI statuses were reported using the proprietary algorithms within these softwares. RNA test was a custom panel using the Invitae's Anchored Multiplex PCR (AMP™)-based NGS method and sequenced on the Thermo Fisher Ion S5™ system and data were analyzed using the Invitae/ArcherDX software.
Case Presentation
A 54-year-old male patient presented to the clinic with a 9-month history of progressive left testicular swelling. He also complained of a 70 lb weight loss, abdominal pain, and decreased appetite. On physical examination, a large left testicular mass with palpable nodularity extending up to the left spermatic cord was identified. Computed tomography imaging of the pelvis revealed an enlarged left testis with a large complex left scrotal fluid collection, with extension into the gonadal vein (Figure 1A). Also, there was moderate left hydronephrosis, with mid-left ureter compression by retroperitoneal adenopathy. Multiple bulky retroperitoneal lymph nodes were identified. Pulmonary computed tomography imaging showed multiple pulmonary nodules, compatible with metastases (Figure 1B). A right lung nodule biopsy was taken.
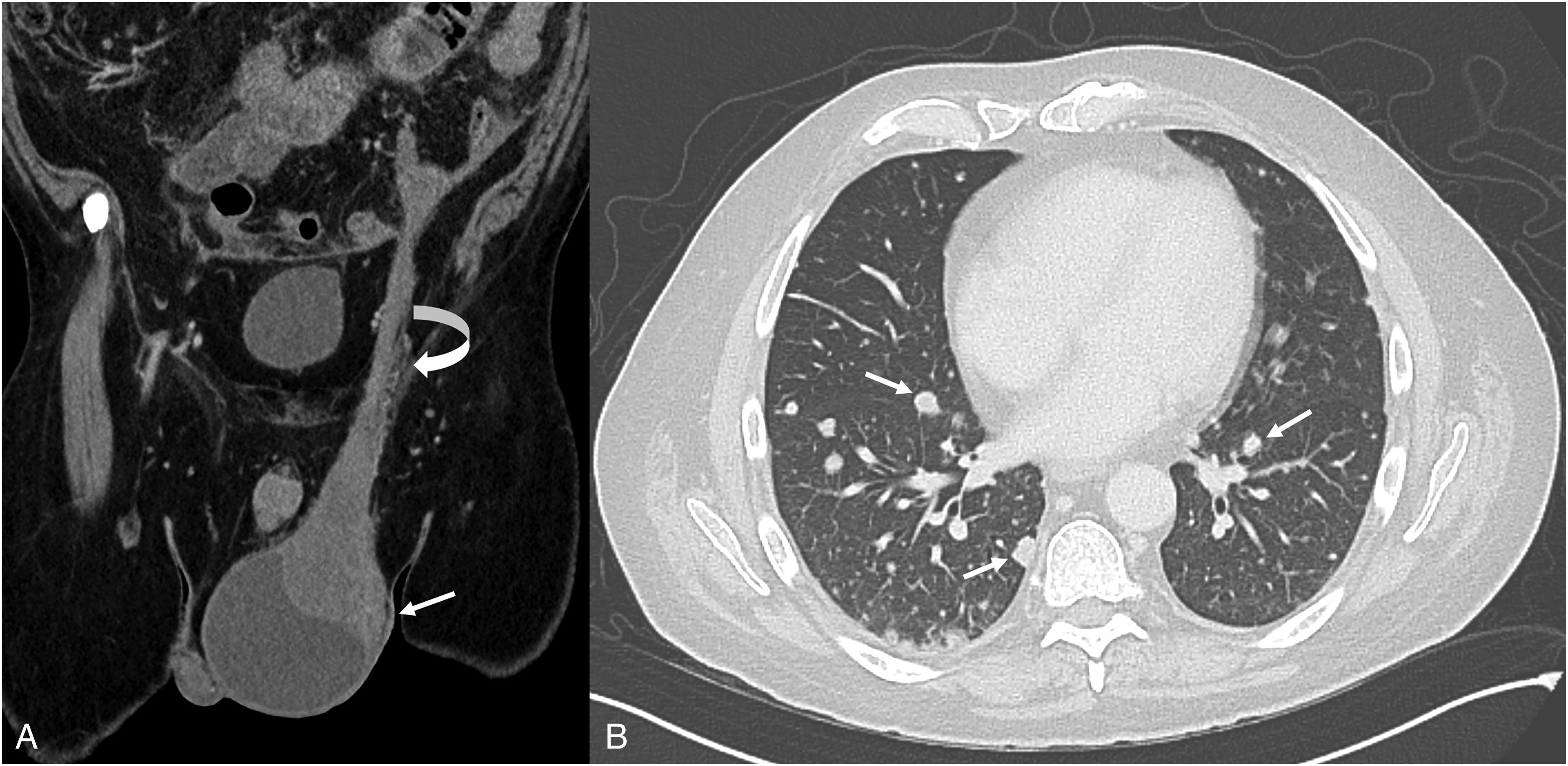
(A) Coronal CT image demonstrating solid and cystic left testicular mass (arrow) with extension into the gonadal vein (curved arrow). (B) Axial CT (lung windows) demonstrating multiple bilateral pulmonary metastases (arrows).
Histopathological Examination
Histologic sections showed lung parenchyma involved by a neoplasm composed of mostly solid architecture with some nested and retiform areas, and variable sclerotic stroma. The tumor was associated with variable inflammatory infiltrates ranging from sparse to moderate, including predominantly lymphocytes, frequent plasma cells, occasional eosinophils, and rare neutrophils. The tumor cells had moderate to abundant eosinophilic cytoplasm with some cells showing lipidized cytoplasm, imparting a “spider-web-like” appearance. The nuclei were mostly uniform round to ovoid with scattered larger nuclei with marked atypia. Focal necrosis was present (Figure 2). The morphology, in this patient's clinical context, was compatible with a metastatic testicular sex cord-stromal tumor. Although initially favored to be a metastatic Sertoli cell tumor, the differential diagnosis also included an inflammatory and nested testicular sex cord tumor.

Lung biopsy specimen. (A) Predominantly solid growth pattern with focal nested and retiform morphology with moderate lymphoplasmacytic infiltrate. (B) Prominent stromal sclerosis. (C) Variable size and shape of nests and tubules, including “pseudotubular” appearance with mild lymphoplasmacytic infiltrate and occasional eosinophils. (D) Focal area of necrosis present. (E) Relatively monomorphic nuclei with increased mitotic figures (circled) and few eosinophils. (F) Few cells with lipidized cytoplasm, and focal and scattered marked nuclear atypia.
Immunohistochemistry
Immunohistochemistry showed that the tumoral cells were positive for SF-1, inhibin, EMA, CD30, WT1, and CD99 (Figure 3); while negative for a battery of other immunohistochemical stains (Table 1). In this patient's clinical context along with the identification of a EWSR1::ATF1 fusion, a thorough immunohistochemical workup was performed to exclude other testicular tumors and tumors associated with this fusion.

Immunohistochemical stains (A) SF-1, diffuse and strong nuclear expression (×200). (B) Inhibin, patchy moderate to strong cytoplasmic expression (×200). (C) EMA, patchy strong cytoplasmic expression (×200). (D) CD30, diffuse and strong cytoplasmic and membranous expression (×200). (E) WT1, diffuse and strong nuclear expression (×200). (F) CD99, patchy and weak membranous expression (×400).
Immunohistochemical Stains Work-up and Results.

CD45, CD20, and CD138 highlighted inflammatory infiltrate within the tumor including white blood cells, B-lymphocytes, and plasma cells, respectively.
Next-Generation Sequencing
Molecular genetic analysis revealed a EWSR1::ATF1 gene fusion, and a TP53 frameshift (c.742dupC; p.R248fs*16) at a 70% variant allele fraction. MSI status was stable and TMB was low.
A final diagnosis of a metastatic testicular sex cord tumor with EWSR1::ATF1 gene fusion was made. Morphologic, immunophenotypic, and molecular findings were consistent with an inflammatory and nested testicular sex cord tumor. The patient passed away 2 months after the diagnosis.
Discussion
Recently, a group of malignant testicular sex cord tumors that were initially interpreted as Sertoli cell tumors or as seminomas, have been described to have recurrent EWSR1::ATF1 fusions. These tumors have characteristic morphologic and immunophenotypic features, and likely different clinical behavior from Sertoli cell tumors. The study by Acosta et al. proposed that these should be classified separately, and descriptively termed these neoplasms as “inflammatory and nested testicular sex cord tumor.” 9 In this article, we describe a case of a malignant testicular sex cord tumor that presented with a left testicular mass, retroperitoneal and mediastinal adenopathy, and lung metastasis, with only a lung biopsy specimen for tumor tissue diagnosis. This was a challenging case which was initially interpreted as metastatic testicular sex cord tumor, favoring a Sertoli cell tumor based on morphology and immunohistochemistry; but later reclassified as an inflammatory and nested testicular sex cord tumor due to the identification of a EWSR1::ATF1 fusion.
Approximately 7-10% of testicular sex cord tumors have been reported to be malignant, with metastasis at presentation in 7% of the cases. 5 It is important to note that some morphological and immunohistochemical features may overlap in both Sertoli cell tumors and inflammatory and nested testicular sex cord tumors.3,6,7 We report a tumor that exhibited a predominantly solid growth pattern with focal nested and retiform morphology. Additionally, prominent stromal sclerosis with a variable inflammatory infiltrate and the presence of focal areas of necrosis were observed. Relatively monomorphic nuclei with scattered marked nuclear atypia and increased mitotic figures were identified, along with a few cells exhibiting lipidized cytoplasm. This tumor was positive for immunohistochemical markers such as SF-1, inhibin, EMA, CD30, WT1, and CD99, some of which are consistently reported to be positive in both tumor types.9-14 Distinguishing inflammatory and nested testicular sex cord tumors from Sertoli cell tumors may be challenging, but identifying the presence of tumoral inflammatory infiltrate, expanding immunohistochemical work-up and the identification of EWSR1::ATF1 fusion will help to differentiate them apart. It is important to consider a comprehensive assessment of clinical, morphological, and molecular features to establish an accurate diagnosis.
The advances of molecular techniques, particularly next-generation sequencing, have expanded our understanding of different malignancies. 15 However, the genomic landscape characterization of testicular sex cord-stromal tumors is still limited. Recent studies have identified recurrent alterations in many cases; nevertheless, a subset of testicular sex cord-stromal tumors show no definite somatic pathogenic alterations or show variable nonrecurrent findings. Rizzo et al described three distinct subgroups of aggressive Leydig cell tumors characterized by FH inactivation, Wnt pathway activation (CTNNB1 or APC mutations), and copy number changes without recurrent mutations. 16 Perrone et al identified CTNNB1 mutations in the majority (71%) of their cohort of 14 Sertoli cell tumors of the testis, including 1 (of 2) malignant Sertoli cell tumors. 6 Moreover, CTNNB1 gene mutations were associated with β-catenin protein accumulation in the nuclei, and indeed all the mutated cases showed both nuclear and cytoplasmic b-catenin expression. Siegmund et al 17 tested 22 cases of sex cord-stromal tumors NOS/mixed sex cord-stromal tumors and identified 7 (32%) of these tumors to harbor CTNNB1 or APC mutations. They suggested that six of these could be re-classified to Sertoli cell tumors based on DNA methylation analysis, combined with morphology, immunohistochemistry, and other molecular data. The remaining cases had no definite somatic pathogenic SNVs with recurrent chromosome-level copy number gains or variable nonrecurrent alterations including pathogenic APC, RB1, and TP53 variants with a subset showing chromosome-level copy number changes. Acosta et al recently described a subset of malignant sex cord tumors that were initially interpreted as Sertoli cell tumors or seminomas and proposed that it should be classified as a distinct new entity: “inflammatory and nested testicular sex cord tumor.” These neoplasms have a characteristic morphology with SF-1, inhibin, EMA, CD30, and WT1 expression by immunohistochemistry, along with recurrent EWSR1::ATF1 fusions. They identified that inflammatory and nested testicular sex cord tumors had an aggressive behavior with a tendency for early systemic spread and suggested that should be differentiated from Sertoli cell tumors and seminoma. 9
In our case, the final diagnosis of inflammatory and nested testicular sex cord tumor was established based on the characteristic solid and pseudotubular architecture with sclerotic stroma, the presence of inflammatory infiltrate, and epithelioid cells showing eosinophilic and clear vacuolated cytoplasm; in combination with positive staining for SF-1, inhibin, EMA, CD30, and WT1 by immunohistochemistry, and the detection of EWSR1::ATF1 fusion. The patient passed away 2 months after the diagnosis. The pathological and clinical findings of our case parallels with that of Acosta et al. 9 It broadens the spectrum of molecular abnormalities previously identified in testicular sex cord-stromal tumors, specifically within the CTNNB1 negative subset. Our case report supports the recurrent nature of EWSR1::ATF1 fusion detection in a subset of testicular sex cord-stromal tumors; highlighting its potential role in the pathogenesis, as a molecular diagnostic marker, in clinical behavior, and for management in inflammatory and nested testicular sex cord tumors.
The EWSR1 gene encodes for a multifunctional RNA-binding protein that is involved in various cellular processes, including transcriptional regulation, splicing, and mRNA transport. 17 The EWSR1 gene can fuse with CREB transcription factors (ATF1, CREB1, CREM) leading to various neoplasms.18,19 The EWSR1::ATF1 fusion gene is a pathologic hallmark of clear cell sarcomas20,21 and has been found in other tumors including angiomatoid fibrous histiocytoma, malignant mesothelioma, clear cell-like tumors of the gastrointestinal tract, primary pulmonary myxoid sarcoma, angiosarcoma of the parotid, and other tumors.22-26
Most testicular sex cord-stromal tumors have a favorable prognosis overall unless it metastasizes, and only up to 10% of cases are malignant at initial staging or at follow-up. Orchiectomy followed by early retroperitoneal lymph node dissection are often the treatment of choice in early stages and localized disease with radiation and chemotherapy used in a limited number of cases with limited effectivity. 27 Metastatic testicular sex cord-stromal tumors are difficult to treat and respond poorly to systemic treatment. Because of the lack of effective chemotherapy and radiation treatment options in these cases, sex cord-stromal tumors metastasis often results in adverse outcome and death 27 which highlights the importance of identifying potential biomarkers for diagnosis, prognosis, and treatment. Similar to our case, which showed positive CD30 staining, Acosta et al reported positive CD30 in 8 of 10 tested cases of inflammatory and nested testicular sex cord tumor. 9 Interestingly, Albany et al reported durable responses in a subset of patients with CD30-expressing germ cell tumors or sex cord-stromal tumors treated with brentuximab vedotin, 14 which highlights potential treatment modalities for these difficult-to-treat tumor types. The absence of effective non-surgical treatment options and the unfavorable clinical outcomes observed in individuals with malignant sex cord-stromal tumors underscore the critical need for biomarkers that can identify aggressive tumors at an early stage, allowing for timely surgical intervention such as retroperitoneal lymph node dissection and potentially improving clinical outcomes. The recognition of inflammatory and nested testicular sex cord tumors as a distinct and novel group of tumors represents a significant finding that could aid in identifying and stratifying patients into high-risk groups.
In conclusion, we report a case of an inflammatory and nested testicular sex cord tumor with a EWSR1::ATF1 gene fusion with metastasis at initial presentation. Identification of the EWSR1::ATF1 fusion in this patient highlights the molecular heterogeneity within sex cord-stromal tumors, supports a specific recurrent genomic alteration within the CTNNB1-negative subset of patients with an aggressive clinical course, and provides additional evidence that inflammatory and nested testicular sex cord tumor should be separately classified as a distinct entity. In addition, EWSR1::ATF1 fusion may be used as a diagnostic biomarker in localized and/or in metastatic cases to improve risk stratification and help guide clinical management.
Supplemental Material
sj-docx-1-ijs-10.1177_10668969231195043 - Supplemental material for Metastatic Testicular Sex Cord Tumor Harboring a EWSR1::ATF1 Gene Fusion—A Case Report of a Novel Neoplasm: “Inflammatory and Nested Testicular Sex Cord Tumor”
Supplemental material, sj-docx-1-ijs-10.1177_10668969231195043 for Metastatic Testicular Sex Cord Tumor Harboring a EWSR1::ATF1 Gene Fusion—A Case Report of a Novel Neoplasm: “Inflammatory and Nested Testicular Sex Cord Tumor” by Hugo Carrillo-Ng, Leonidas Arvanitis, Saro Manoukian and Javier A. Arias-Stella in International Journal of Surgical Pathology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval was not required for this case report. This report was compliant with HIPAA standards. This report does not include any personal identifiers.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.