
Abstract
We present the case of a 6-year-old girl who presented with alterations in the voiding stream. On physical examination, a very small urethral meatus was identified at the expense of a membrane. The renovesical ultrasound showed no alterations. An uroflowmetric study was performed, showing a bladder outlet obstruction pattern. The urethral meatus was calibrated and a ventral meatotomy was performed. The histological study of the resected membrane showed a transitional urethral mucosa with chronic focal inflammation and discrete hyperplasia. The patient evolved favorably, with resolution of the symptoms and no notable complications. This is, to the best of our knowledge, the first reported case with a histological study of a congenital meatal urethral stenosis. In the presence of lower urinary tract obstruction, this entity should be considered in the differential diagnosis. Surgical treatment is curative.
Introduction
Congenital urethral distal stenosis in female patients constitutes an extremely infrequent pathological spectrum. The existing literature to date is limited.
Material and Methods
The usual methodological and ethical principles for scientific publication were followed. Photographs, sociodemographic and clinical data of a patient with a confirmed diagnosis of congenital urethral distal stenosis managed at our center in 2023 were collected. All information was anonymized in accordance with current legislation. A review of the existing scientific literature was also carried out. Eligible studies were identified by searching the main existing medical bibliography databases (PubMed, Medline, Web of Science, Scopus). The search was last executed on 6.4.2023.
Case Report
We present the case of a 6-year-old girl, with a healthy dichorionic biamniotic sister, who came for evaluation because she presented with alterations in the voiding stream. Sphincter control had developed normally in early childhood, but her parents reported that she had always had difficulty urinating with a thin, cranial stream that required significant abdominal pressure to achieve complete bladder emptying, with a voiding time of up to 5 min (Supplemental video 1). She did not present any urinary tract infections at any time. On physical examination, a poriform urethral meatus was identified, discreetly ectopic (with a cranial disposition) at the expense of a membrane covering (Figure 1). A renovesical ultrasound study was requested, which showed no alterations. An uroflowmetric study was performed, showing a very low urinary flow throughout the study, highly suggestive of bladder outlet obstruction (mean flow 1.6 mL/s, maximum flow 3.8 mL/s, total volume 232 mL, residual volume 5 mL, voiding time 145 s). No alterations in renal function (serum creatinine) were observed. With these findings, the clinical diagnosis of congenital urethral distal stenosis was established and urethrocistoscopy and surgical correction were indicated.

Clinical photograph of the patient. Above: Note the presence of a stenotic urethral foramen, cranially disposed. Below: with urination, a marked bulging of the membrane caudal to the foramen is seen.
The urethral meatus was calibrated with a Fogarty 3 French balloon, and a ventral membrane cut was performed over it to avoid damaging adjacent structures. The edges of the aforementioned membrane were resected and sent for anatomopathological study and a meatoplasty was performed with a 6/0 non-absorbable monofilament interrupted suture. Subsequently, an exploratory urethrocystoscopy was performed, which showed a discrete trigonitis with orthotopic ureteral meatus and no bladder trabeculation or diverticula (Figure 2). No other alterations were identified in the urethral exploration. An 8 French Foley catheter was left in place for 24 h, after which it was removed. The patient was discharged the day after the operation, with resolution of the symptoms and no complications. The anatomopathological study showed that the membrane fragments corresponded to transitional urethral mucosa with chronic focal inflammation and discrete hyperplasia (Figure 3). Postoperative evolution was favorable, with a resolution of symptoms and a normalized uroflowmetric study 2 months after surgery.
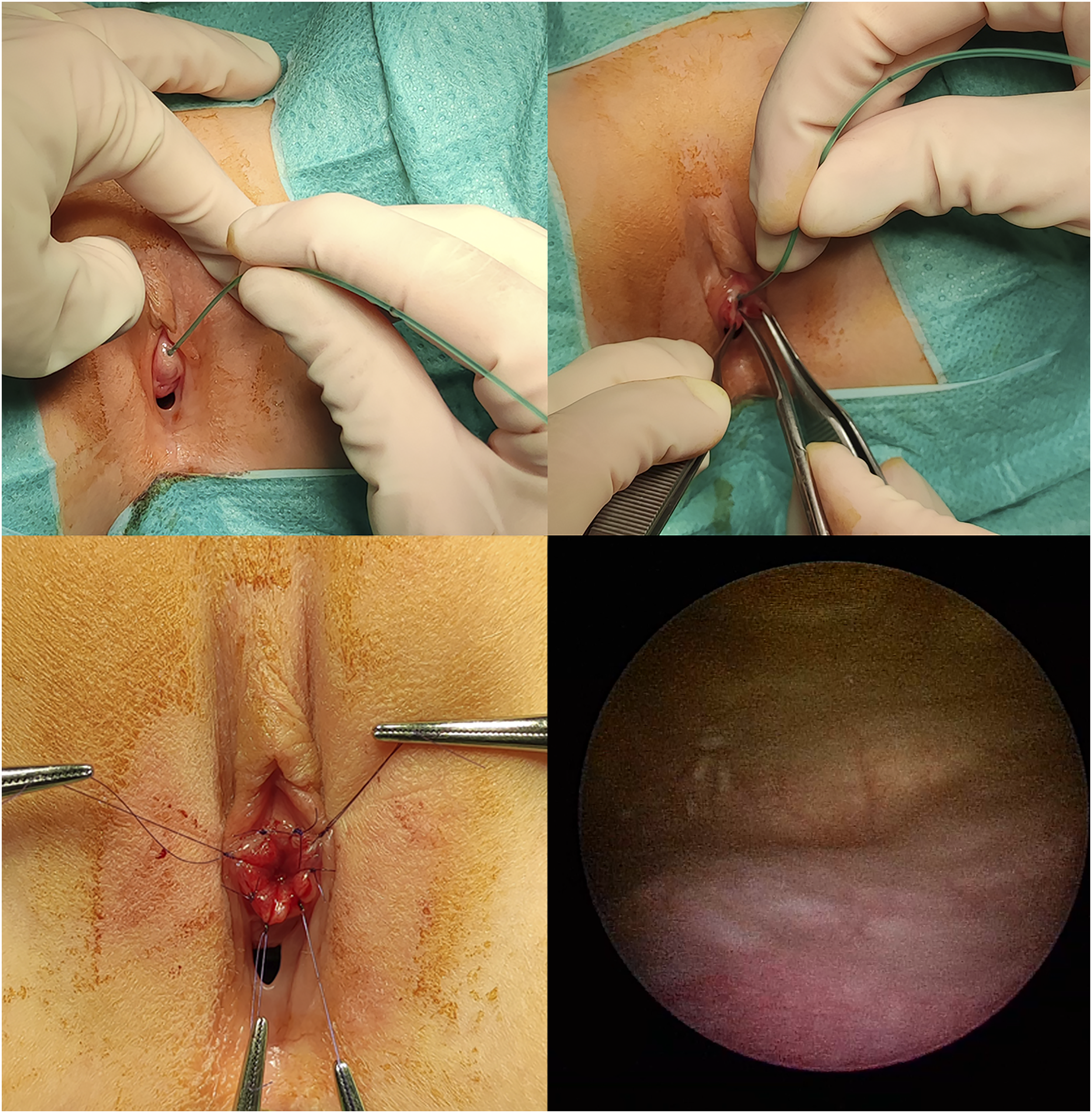
Intraoperative imaging. Above, left: calibration of the urethral meatus with a Fogarty 3 Fr catheter. Above, right: ventral meatotomy over the catheter. Below, left: immediate postsurgical result after meatoplasty. Below, right: cystoscopic image showing moderate trigonitis without other alterations.

Histopathological examination of the membrane. Transitional urethral mucosa with chronic focal inflammation and discrete hyperplasia.
Discussion
From an embryological point of view, an alteration in the development of the distal urogenital sinus could condition urethral stenosis, especially at the level of the bulbar urethra in males. 1 The embryological alteration underlying the type of distal stenosis here presented (congenital urethral distal stenosis) has not been clarified to date but could be an extension of the mechanism proposed by Watanabe et al. 1
Regarding the clinical implications, this aborted or incomplete form justifies that, in our patient, we did not find the spectrum of nephrourological alterations present in the severe cases of congenital lower urinary tract obstruction (eg, bladder trabeculation, vesicoureteral reflux, nephropathy). 2 This, in turn, justifies the fact that the patient's symptoms were only moderate and that the diagnosis was established at an advanced age. The fact that it is a mildly clinical form is a factor that increases the delay and diagnostic complexity of these patients.
In our review of the literature, we found only 2 references that partially overlapped with ours. The first paper, published by Biewald et al. in 1987, 3 refers to all female congenital urethral distal stenosis. The authors classify these stenoses as incomplete, complete, and pure distal stenoses, the latter representing 1% of the series presented. The authors discuss the associated symptomatology (recurrent infections and voiding problems) and the applicable therapy, consisting of calibration and meatotomy, with an adequate symptom resolution rate. Subsequently, Shi et al. succintily reported a case in 2017 4 which was very similar to ours, with the particularity that the patient had unilateral grade III vesicoureteral reflux and urethral dilatation in the voiding cystourethrography. In our case, given the normality of the ultrasound study and the absence of upper urinary tract sintomatology, we opted not to perform a voiding cystourethrography to avoid ionizing radiation to the patient. The patient reported by Shi et al. was also treated with meatoplasty and the condition resolved favorably.
It should be considered that there is a potential variant of this entity, of an acquired nature, in which fibrosis or stenosis forms secondary to repeated urinary tract infections in young girls. 5 Although the clinical management may be similar, these are 2 distinct entities and should be considered as such (eg, when further studies are indicated).
Regarding the histopathological study and to the best of our knowledge, this is the first work in which the histological characteristics of the affected tissue are documented. The characterization of the membrane as urothelial tissue with moderate inflammation and hyperplasia fits within the clinical findings and in our opinion does not require additional studies in this regard.
Congenital urethral distal stenosis is an exceptional finding but should be considered as a potential cause of voiding disturbance/voiding dysfunction in female pediatric patients. Uroflowmetric study and renovesical ultrasound are, in our opinion, essential to establish an accurate diagnosis. Meatotomy and meatoplasty seem to be an effective and safe treatment for this condition.
Supplemental Material
Footnotes
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was not sought due to the descriptive and retrospective nature of this isolated case report. All clinical information was anonymized following institutional guidelines and current legislation.
Informed Consent
Before the submission of this article, verbal and written informed consent was obtained from the legal guardians of the patient whose clinical photographs are included in this publication. Patient medical records were accessed according to our institutional guidelines.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.