
Abstract
Gastric adenocarcinoma with enteroblastic differentiation is a specific subtype of gastric cancer that is rare and highly malignant, usually presenting at an early stage with lymphovascular invasion, lymph node, and distant metastases, resulting in a poor prognosis. The pathology of this patient showed a classic tubular adenocarcinoma infiltrating into the mucosal layer, with the presence of cytoplasmic translucent tumor cells below the mucosal layer. It is noteworthy that this patient did not exhibit lymphovascular invasion, lymph node, and distant metastasis. Additionally, a large amount of calcification was observed; therefore, it remains unclear whether there exists any correlation between the two factors. To the best of our knowledge, this is the first case report demonstrating massive calcification in gastric adenocarcinoma with enteroblastic differentiation, which may have implications for future diagnosis of this rare subtype of gastric cancer.
Introduction
Gastric adenocarcinoma with enteroblastic differentiation is a rare subtype of gastric cancer that mainly affects elderly males and exhibits a higher propensity for early lymphovascular invasion, lymph node, and distant metastasis compared to conventional gastric adenocarcinoma. The pathology of gastric adenocarcinoma with enteroblastic differentiation is characterized by the presence of tumor cells exhibiting hyaline cytoplasm and forming tubular or papillary structures, reminiscent of fetal intestinal epithelial morphology. There are only about 40 reports on gastric adenocarcinoma with enteroblastic differentiation to date and the pathogenesis of gastric adenocarcinoma with enteroblastic differentiation is unclear. Here we report a case of gastric adenocarcinoma with enteroblastic differentiation in the presence of massive calcification which has been reported to play a possible protective role in some tumors, and the relationship between tumorigenic calcification and gastric cancer remains to be investigated as no lymphovascular invasion or metastasis was observed in this patient.
Case Report
A 68-year-old Chinese man was found to have a gastric mass during a routine physical examination. Abdominal enhanced computed tomography (CT) showed thickening and enhancement of the gastric antrum, as well as several small lymph nodes adjacent to the abdominal aorta, consistent with gastric cancer (Figure 1A). Preoperative laboratory tests: α-fetoprotein (AFP) 13.11 ng/ml, carcinoembryonic antigen (CEA) 2.55 ng/ml, CA199 8.10 μ/L, CA125 13.20 μ/L, Ca 2.25 mmol/L, all of which were normal. In September 2022, the patient underwent laparoscopic gastric resection and lymph node dissection.
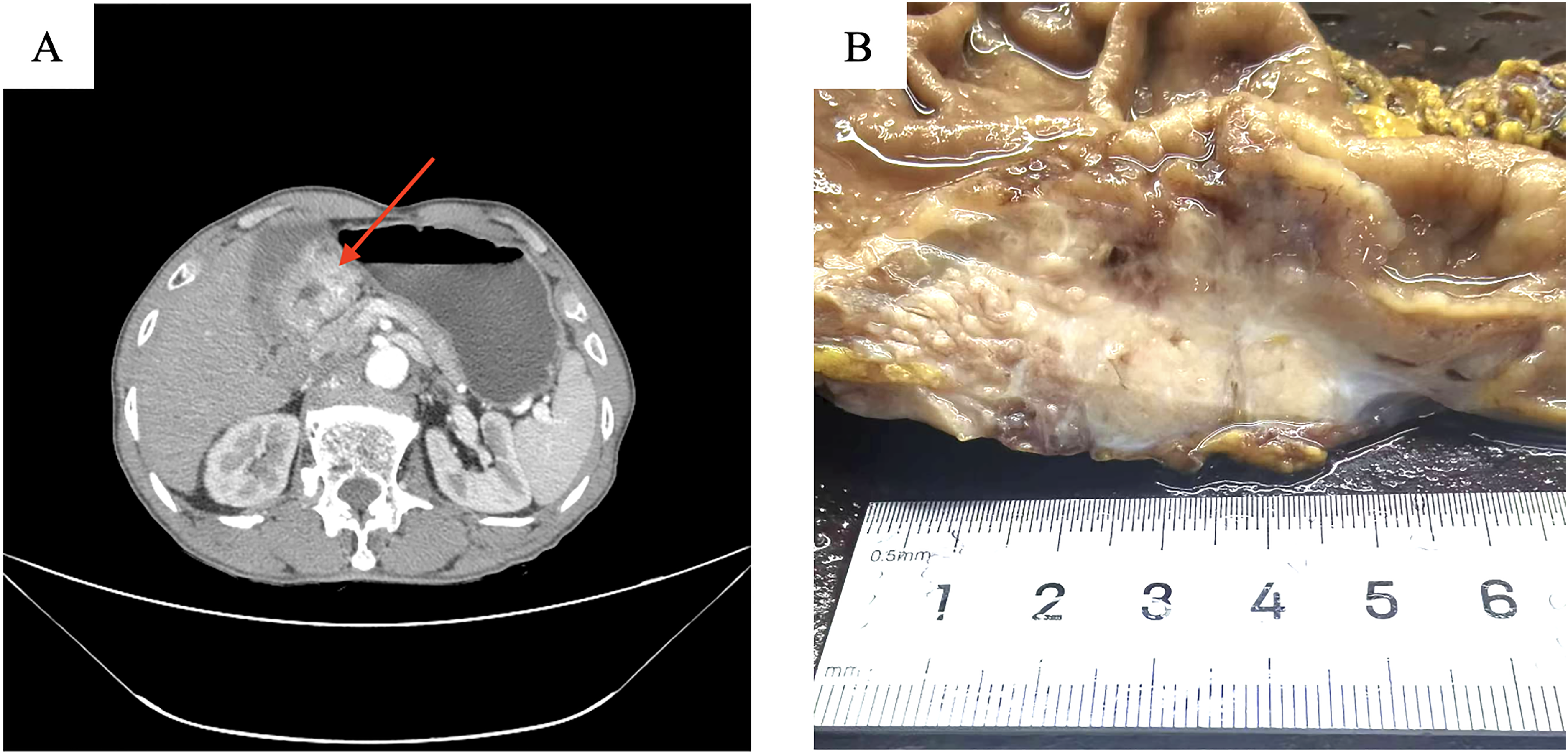
Abdominal enhanced CT showed thickening and enhancement of the gastric antrum, shown by the arrow (A). Gross examination showed an ulcerated mass in the gastric antrum (B).
Histopathology
Macroscopically, the resected specimen showed an ulcerative mass in the gastric antrum, measuring 4.5 × 3.5 × 3.0 cm, with a gray-white color and moderate texture. The tumor invaded the serosa layer (Figure 1B).
Microscopically, highly differentiated classic tubular adenocarcinoma was seen in the mucosal layer (Figure 2A). The tumor cells below the mucosal layer formed tubular and papillary structures (Figure 2B). Notably, a large amount of calcification was observed in the glandular lumen or fibrous septum (Figure 2C). The tumor cells below the mucosal layer were square or columnar in shape with clear cell boundaries and hyaline cytoplasm, similar to fetal intestinal epithelium. The nuclei of the tumor cells were round or ovoid, with coarse granular chromatin and partially visible nucleoli, and mitotic figures were easily seen (Figure 2D). There is no evidence of lymphovascular or perineural invasion, and tumor metastasis was not seen in gastric lymph nodes or distant organs.

Highly differentiated classic tubular adenocarcinoma was seen in the mucosal layer (A). The tumor cells below the mucosal layer formed tubular and papillary structures (B). A large amount of calcification was seen (C). The tumor cells below the mucosal layer were square or columnar in shape with clear cell boundaries and hyaline cytoplasm, similar to fetal intestinal epithelium (D). (A–C: H&E, original magnification ×40; D: H&E, original magnification ×200).
Immunohistochemistry
The tumor cells below the mucosal layer were positive for SALL4, CDX2, MUC2, CD10, MLH1, MSH2, MSH6, and PMS2 and negative for AFP, glypican-3, ERBB2/HER2, KRT7, KRT20, and P53 (Figure 3A–C). Ki67 expression was 60% (Figure 3D).

Diffuse strong positive expression of SALL4 (A). Negative expression of AFP (B). Diffuse strong positive expression of CDX2 (C). Ki67 expression was 60% (D). (A–D: immunohistochemistry, original magnification ×40).
Antibodies against SALL4 (6E3, 1:200, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China), MUC2 (Ccp58, 1:200, Guangzhou Lbp Medicine Science & Technology Co., Ltd, Guangzhou, China), CD10 (UMAB235, 1:800, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China), AFP (EP209, 1:400, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China), CDX2 (EP25, 1:800, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China), KRT20 (EP23, 1:800, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China), Ki67 (UMAB107, 1:400, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, China), P53 (DO-7, 1:800, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China), KRT7 (OV-TL 12/30, pre-diluted, DAKO, Glostrup, Denmark), MLH1 (ES05, pre-diluted, DAKO, Glostrup, Denmark), MSH2 (FE11, pre-diluted, DAKO, Glostrup, Denmark), MSH6 (EP49, pre-diluted, DAKO, Glostrup, Denmark), PMS2 (EP51, pre-diluted, DAKO, Glostrup, Denmark), ERBB2/HER2 (EP3, 1:400, Gene Tech (Shanghai) Company Limited, Shanghai, China), and glypican-3 (OTI1G5, 1:400, Beijing Zhong Shan Goldenbridge Biotechnology Company Ltd, Beijing, China) were used in this study.
Based on the morphological and immunohistochemical characteristics, the final pathological diagnosis was gastric adenocarcinoma with enteroblastic differentiation, infiltrating the serosa layer, without metastasis in 37 lymph nodes. The patient received three cycles of postoperative chemotherapy and has been followed up for three months without recurrence or metastasis.
Discussion
Gastric adenocarcinoma with enteroblastic differentiation is a concept first proposed by Matsunou et al in 1994. 1 However, it was not clearly defined until the fifth edition of the WHO classification of digestive system tumors in 2019, which named it gastric adenocarcinoma with enteroblastic differentiation. Research indicates that the clinical features of gastric adenocarcinoma with enteroblastic differentiation are similar to those of traditional gastric adenocarcinoma, and it predominantly affects elderly men, with the most common site being the gastric antrum. The incidence rate of gastric adenocarcinoma with enteroblastic differentiation accounts for 10–15% of gastric cancer. However, compared to traditional gastric adenocarcinoma, gastric adenocarcinoma with enteroblastic differentiation is more likely to invade into lymphatic vessels and vascular lumen, and to metastasize to the liver and lymph nodes.2,3 Morphologically, gastric adenocarcinoma with enteroblastic differentiation grows in a tubular or papillary pattern, characterized by cuboidal or columnar cells, with transparent cytoplasm and nuclei located at the base, similar to the morphology of early fetal intestinal epithelium.4,5 Immunohistochemically, gastric adenocarcinoma with enteroblastic differentiation expresses at least one marker of the intestinal progenitor cell lineage (AFP, glypican-3, SALL4), with glypican-3 being the most sensitive. In addition, based on the expression combination of MUC2, CD10, MUC5AC, and MUC6, gastric adenocarcinoma with enteroblastic differentiation can be classified as intestinal or gastroenteric type. 6 The pathology of this patient shows that the traditional components of gastric adenocarcinoma are distributed within the mucosal layer, whereas the enteroblastic differentiation components are located below the mucosal layer. It is worth noting that there are massive calcifications in the tissue below the mucosal layer, which is an extremely rare phenomenon.
Calcification refers to the phenomenon of calcium salt deposition in cells or tissues, including physiological and pathological calcification. Physiological calcification occurs in bones and teeth. Pathological calcification is divided into dystrophic calcification and metastatic calcification. The former occurs on the basis of cell injury and necrosis, while the latter is caused by hypercalcemia. 7 Tumor calcification is usually mainly dystrophic calcification and is related to tumor progression, diagnosis, and prognosis. Tumor calcification is common in meningioma, papillary thyroid carcinoma, ovarian mucinous papillary carcinoma, and even serves as one of the diagnostic criteria.8–10 Calcification in gastric cancer is rare, occurring in less than 3% of gastric cancer patients. Tumor calcification in gastric cancer can be classified into two types: dystrophic calcification, which is typically associated with mucin deposition and commonly observed in gastric mucinous adenocarcinoma, presenting as diffuse or patchy calcification within the mucus pool and psammomatous calcification, which has been reported in both early and advanced tubulopapillary adenocarcinoma.11–13 Currently, there are ongoing reports regarding gastric adenocarcinoma with calcification and gastric adenocarcinoma with enteroblastic differentiation, respectively. However, to the best of our knowledge, this case is the first to report gastric adenocarcinoma with enteroblastic differentiation in the presence of calcification.
It is well-known that gastric adenocarcinoma with enteroblastic differentiation is highly invasive and can metastasize early. Although the tumor invaded into the serosa layer in this patient's pathology, it did not show lymphovascular invasion, lymph node and distant metastases. It remains unclear whether calcification played a role in this outcome. Research has found that in mucinous gastric adenocarcinoma with calcification, tumor cells undergo ischemic necrosis after chemotherapy, leading to further increase in calcification, which may indicate effective chemotherapy and improved prognosis. 11 The current reports of gastric adenocarcinoma with psammoma bodies suggest that prognosis for gastric adenocarcinoma with calcification may be better than that for the conventional type. Additionally, Burkill et al have shown that the presence of calcification in ovarian cancer is usually associated with low-grade tumors and a better prognosis. 9 Easson et al found that calcification in colorectal liver metastases appears to be associated with a better prognosis. 14 However, Nakada et al concluded that thymomas with calcification have more invasiveness and poorer prognosis. 15 Therefore, it remains uncertain whether calcification is associated with a protective effect against gastric cancer. Further accumulation of case reports with follow-up information is required to clarify this issue.
The definitive establishment of the mechanism underlying the formation of dystrophic calcification and psammomatous calcification in gastric cancer remains inconclusive. Current evidence suggests that dystrophic calcification may be formed by multiple factors in the tumor microenvironment. Firstly, factors such as ischemia, radiotherapy, and chemotherapy may cause tumor cell necrosis, leading to the deposition of calcifications in the tissue. For example, calcification in uterine fibroids often occurs after tumor cell necrosis due to their rapid growth rate compared to blood supply. 16 Secondly, the high secretion activity of cells in the tumor microenvironment may induce enhanced calcium metabolism, leading to the gradual accumulation of calcium salts. Tsuchida et al found that collagen and vesicles secreted by tumor cells in the ultrastructure of meningiomas can form psammoma bodies. 17 Lastly, Scimeca et al found that epithelial-mesenchymal transition in breast cancer may induce epithelial cells to acquire osteoblast-like features, resulting in calcium salt accumulation through physiological mineralization. 18 The formation mechanism of psammomatous calcification remains a subject of controversy, as some studies propose that psammomatous bodies may arise from dystrophic calcification associated with cellular degeneration. 19 However, Murayama et al demonstrated that psammomatous bodies evolve from osmiophilic intracytoplasmic deposits to crystalline apatite and are eventually released into the extracellular space. 13 In summary, tumor calcification may be attributed to multiple molecular mechanisms. However, in gastric cancer, especially in gastric adenocarcinoma with enteroblastic differentiation, the mechanism of calcification formation requires further investigation.
Furthermore, due to the rarity of gastric adenocarcinoma with enteroblastic differentiation, there is very limited research available. Akazawa et al showed that the most common mutated gene in gastric adenocarcinoma with enteroblastic differentiation is TP53, which results from aberrant methylation due to reduced expression of the promoter of TP5320,21 . In addition, it has been shown that DNMT3A positive gastric adenocarcinoma with enteroblastic differentiation is more likely to develop distant organ metastases. 22 Meanwhile, SMAD4 inactivation increased the invasiveness of gastric adenocarcinoma with enteroblastic differentiation. 23 Currently, the pathogenesis and prognosis of gastric adenocarcinoma with enteroblastic differentiation remain poorly understood, and further research is needed to explore these areas.
In summary, we have presented the first case of gastric adenocarcinoma with enteroblastic differentiation in the presence of calcifications. Although gastric adenocarcinoma with enteroblastic differentiation is characterized by high invasiveness and a propensity for metastasis, these features were not observed in this patient. It remains unclear whether this is related to tumor calcification, and the pathological significance and mechanism of tumor calcification in gastric adenocarcinoma with enteroblastic differentiation require further clarification.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Youth Research Fund of Shaoxing People’s Hospital, (grant number 2022YA08).
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any clinical trials.
Trial Registration
Not applicable, because this article does not contain any clinical trials.