
Abstract
Introduction: Cytological diagnosis of sarcomas requires detailed cytomorphological assessment and integration of immunocytochemistry and/or molecular testing. The role of exfoliative cytology, as compared to aspiration cytology, is less understood. This case series describes well-differentiated/dedifferentiated liposarcomas in effusions, with cytomorphological features, ancillary test results and clinical outcomes detailed. Methods: A computerized search of the department pathology archives was performed for sarcomatous effusions with histological diagnosis or clinical history of well-differentiated/dedifferentiated liposarcoma. Clinical progress, cytology slides, immunocytochemistry and molecular test results were reviewed. Results: Six patients were identified. In 5 patients with clinical follow up, 4 (80%) were deceased within 5 months of malignant effusion. One patient was alive with 12 years disease-free survival after radical resection with adjuvant radiotherapy. Three patients showed dedifferentiation on histology, and high-grade (dedifferentiated) tumor cells were present in effusion cytology of 2 patients. Two showed well-differentiated components only on biopsy, but high-grade (dedifferentiated) tumor cells were identified in cytology. The high-grade tumor cells displayed marked nuclear irregularity, enlargement, size variation, with macronucleoli and multinucleation. Well-differentiated lipomatous components were demonstrated in 4 patients (66.7%), comprising of multivacuolated lipoblasts and atypical lipocytes. CDK4 and MDM2 immunoreactivity in all 3 cases with cell blocks, and CDK4 and MDM2 amplification in one were successfully demonstrated. Conclusion: Lipomatous and dedifferentiated components can be sampled and cytomorphologically identified on effusion fluids of liposarcomas, with sufficient cellularity for immunocytochemistry and molecular testing. Although generally associated with poor prognosis, long disease-free survival with sarcomatous effusion is possible with radical surgery and adjuvant treatment.
Introduction
Diagnosis of sarcomas on cytological specimens is challenging as detailed cytomophological assessment and integration of ancillary test results, including immunocytochemistry and molecular testing, are required. Approaches and limitations of aspiration cytology on sarcoma diagnosis have been studied, 1 but reports of sarcomatous effusions are rare.2,3 In this case series with the greatest number to date, 6 patients of sarcomatous effusion of well-differentiated/dedifferentiated liposarcomas are described, with cytomorphological features, ancillary test results and clinical outcomes detailed, aiming to expand the understanding of the role of exfoliative cytology in the diagnosis of sarcomas.
Methods
A computerized search of the department pathology archives from the year 2010 to 2021 was performed to retrieve cytology and surgical specimens with the diagnosis of well-differentiated or dedifferentiated liposarcoma. The patient identity number of the surgical specimens retrieved was further matched to those of effusion cytology specimens, and matched specimens with a diagnosis of atypia or above (C3-5, including suspicious and malignant diagnoses) were also retrieved.
All cytology slides, and corresponding histology slides if available, were examined by 2 pathologists (JJXL and JKMN) to confirm the presence of tumor cells and for assessment of cytomorphological features. Ancillary tests, including immunocytochemistry and fluorescence in situ hybridization (FISH) were reviewed if performed. Discrepancies were resolved by reviewing the slides on a multiheaded microscope or images on a digital monitor until a consensus is reached.
Results
A total of 6 patients were identified, including 3 female and 3 male patients, aged 47 to 80 years. Four of the patients had pleural fluids whereas the remaining 2 were peritoneal fluids. Histological evidence of dedifferentiation and high-grade undifferentiated components were present in 2 and 1 patients, respectively. Only core biopsy was available for 2 patients, and both only consisted of well-differentiated liposarcomatous component, and in 1 the corresponding histology slides were not available for review (Table 1).
Clinical Features of the Cohort.
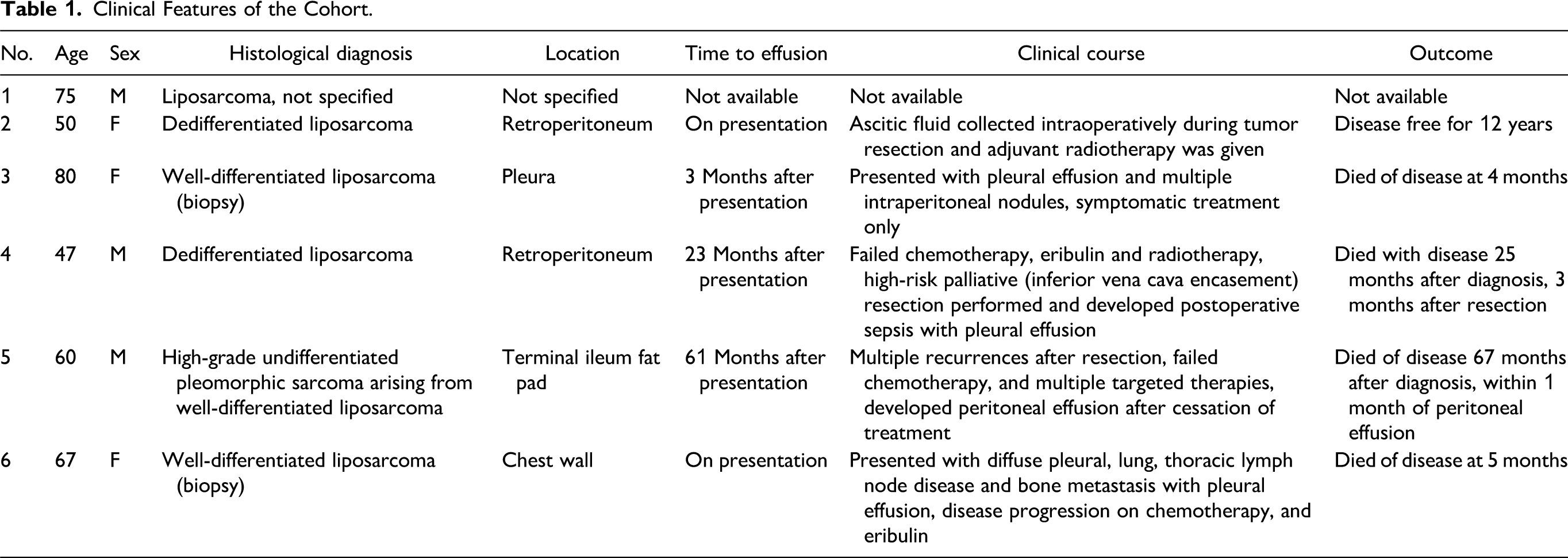
In the 5 patients with clinical follow up, 4 (80%, n = 4/5) were deceased within 5 months of malignant effusion. Although one of the patients (patient 4) died of sepsis, the patient had already failed multiple lines of therapy, and only palliative (grossly incomplete) resection could be performed. The prognosis of these patients with malignant effusion was dismal and all were associated with advanced disease (Figure 1). There was 1 patient (patient 2) alive with no evidence of recurrence despite having tumor cells detected on peritoneal fluid cytology. In that isolated patient with prolonged survival, treatment was aggressive with surgery and adjuvant radiotherapy (Table 1).
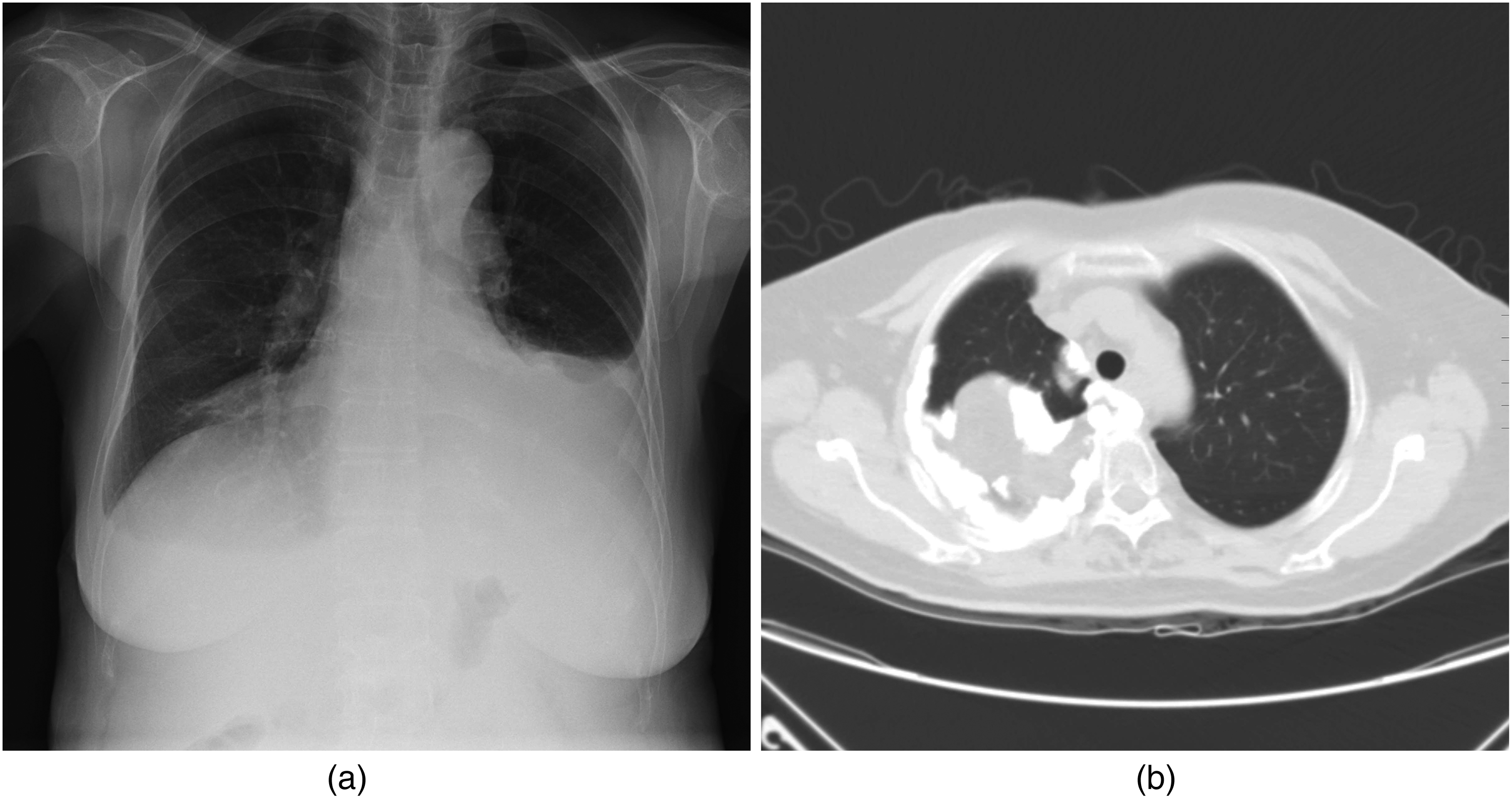
Radiological findings. (a: patient 3) Unilateral pleural effusion, chest X-ray. (b: patient 6) Liposarcoma of the right lung involving the hilum and mediastinum, computed tomography.
On review of cytology slides, lipomatous components were demonstrated in specimens of 4 patients (66.7%, n = 4/6), comprising of multivacuolated lipoblasts in all, with one additionally containing atypical lipocytes (Figure 2). High-grade pleomorphic tumor cells were seen in 3 (50%, n = 3/6). The high-grade tumor cells generally displayed severe nuclear atypia including marked nuclear irregularity, enlargement, size variation, macronucleoli, and multinucleated tumor cells (Table 2 and Figure 3). Cell block preparation was available for 3 specimens (patients 3, 5, and 6), which were prepared using plasma-thrombin (procedures in Supplemental file 1), and all showing positivity to CDK4 and MDM2 immunocytochemistry (Figure 4). CDK4 and MDM2 FISH were performed for patient 6 and revealed amplification (Table 1 and Figure 5).
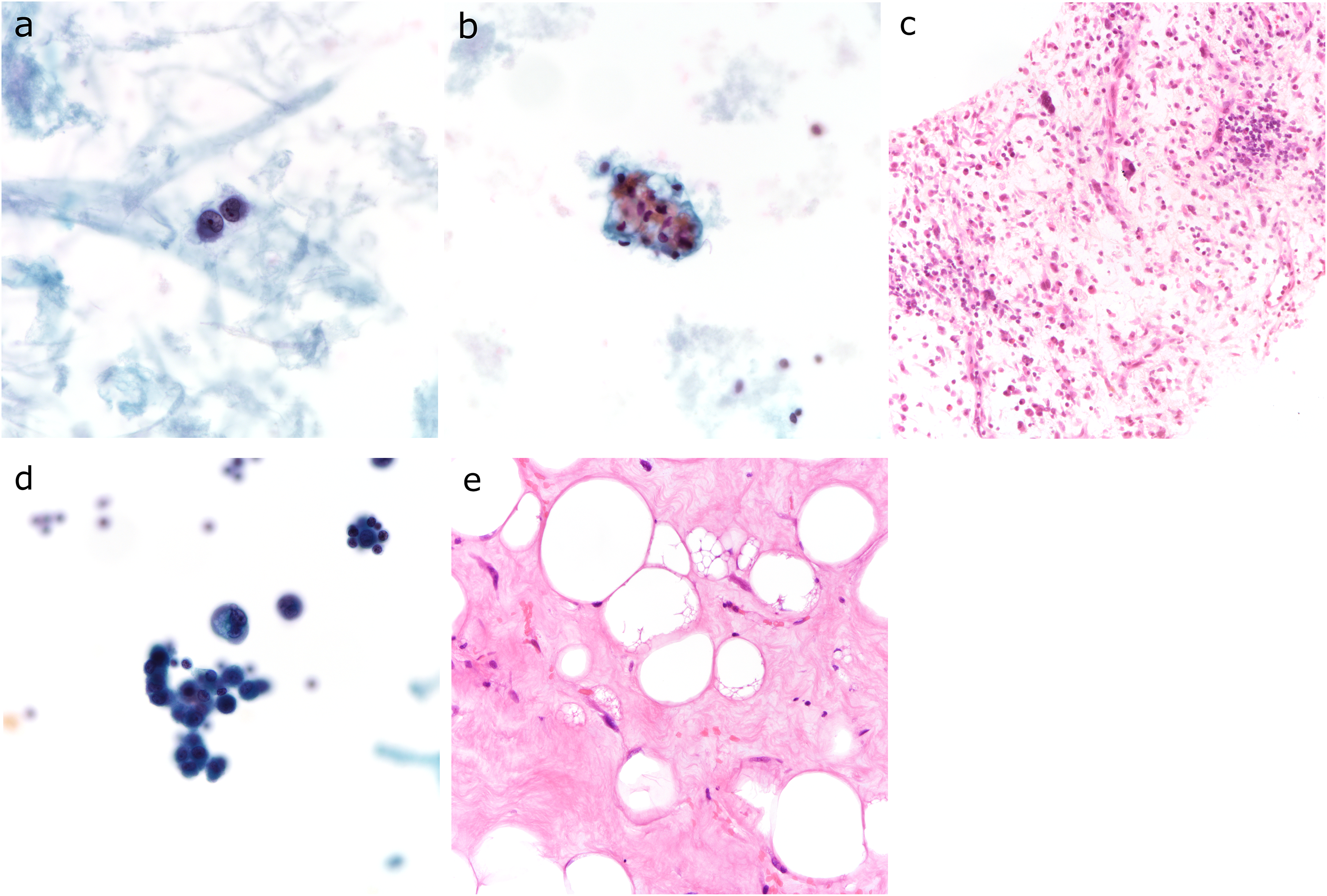
Cytomorphological evidence of lipomatous differentiation. (a: patient 1) Multivacuolated lipoblasts, cytospin, pap stain, 400× magnification. (b: patient 2) Atypical lipocytes and multivacuolated lipoblasts, cytospin, pap stain, 400× magnification. (c: patient 2) Histology of Figure 1b with atypical multinucleated cells and multivacuolated lipoblasts, H&E, 100× magnification. (d: patient 3) Multivacuolated lipoblasts with severely atypical, dedifferentiated tumor cells, cytospin, pap stain, 400× magnification. (e: patient 3) Histology of Figure 1d with atypical lipocytes, stromal cells, and multivacuolated lipoblasts on histology, H&E, 200× magnification. Abbreviation: H&E, hematoxylin and eosin.
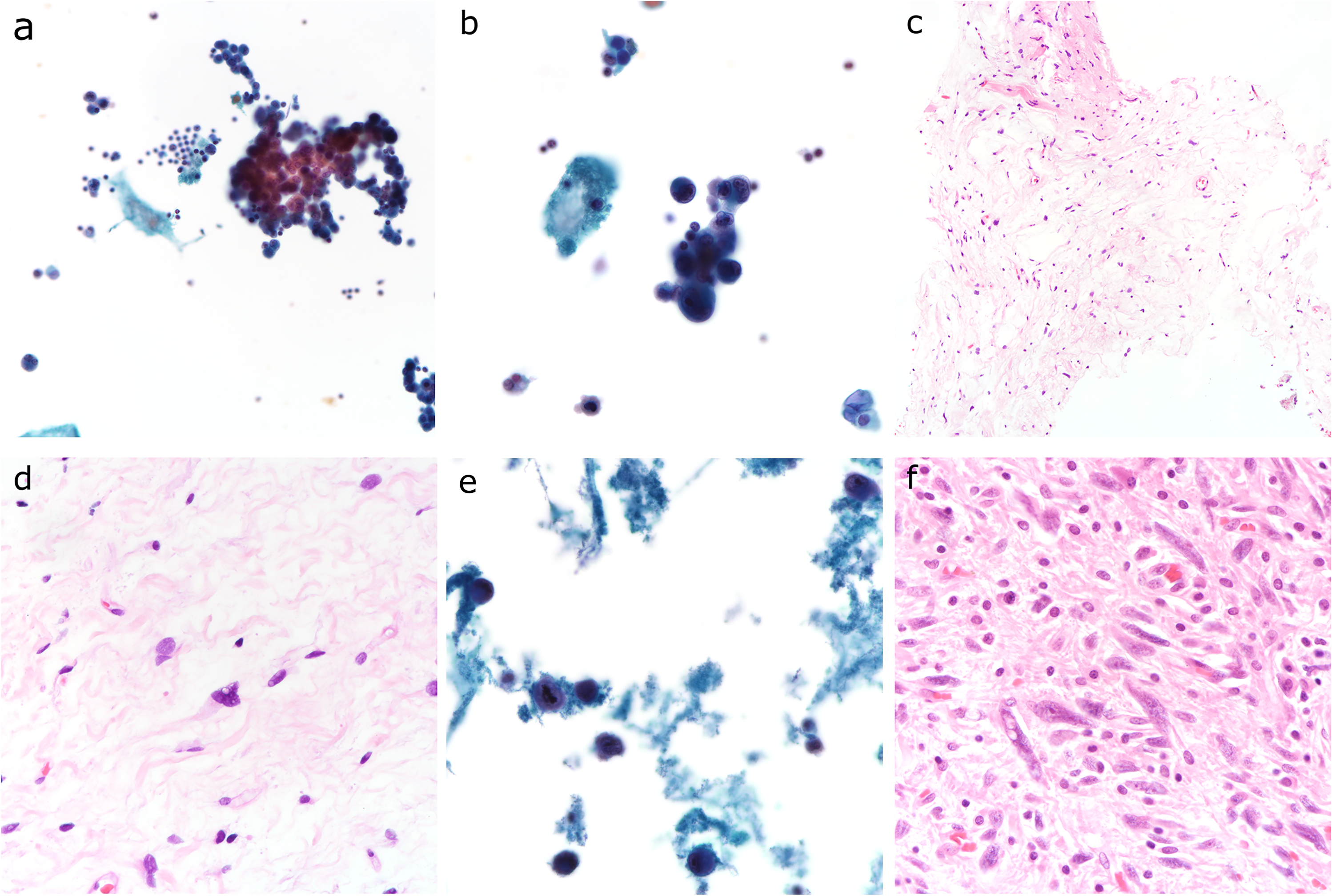
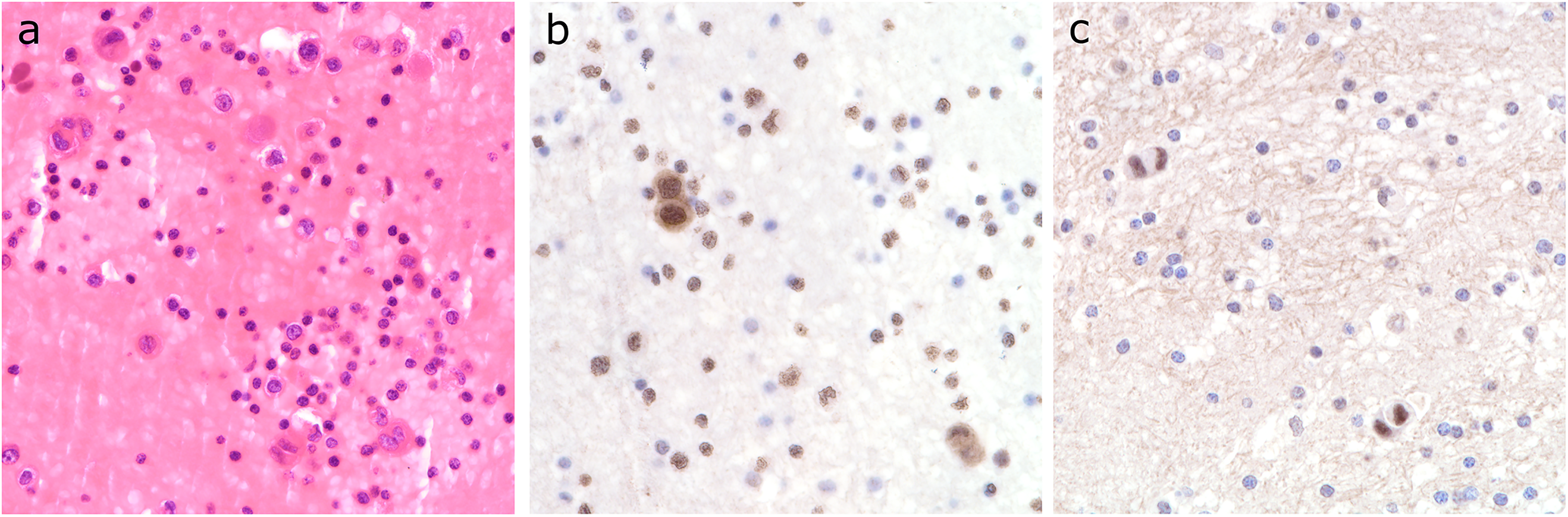
Cytomorphological evidence of dedifferentiated tumor cells. (a: patient 3) High cellularity with large clusters of tumor cells, cytospin, pap stain, 200× magnification. (b: patient 3) Multinucleated tumor cells, cytospin, pap stain, 400× magnification. (c: patient 3) Histology of Figures 2a and b showing lack of lipomatous differentiation at low magnification, H&E, 100× magnification. (d: patient 3). Histology of Figures 2a and b with low-grade dedifferentiated tumor cells, H&E, 400×magnification. (e: patient 5) Tumor cells showing severe nuclear atypia with irregular, hyperchromatic, enlarged nuclei and macronucleoli, cytospin, pap stain, 400× magnification. (f: patient 5) Histology of Figure 2e showing pleomorphic hyperchromatic dedifferentiated tumor cells, H&E, 400× magnification. Abbreviation: H&E, hematoxylin and eosin.
Cell block CDK4 and MDM2 immunocytochemistry. (a: patient 5) Cell block section, H&E, cell block, 400× magnification. (b: patient 5). CDK4 immunocytochemistry, cell block, 400× magnification. (c: patient 5) MDM2 immunocytochemistry, cell block, 400× magnification. Abbreviation: H&E, hematoxylin and eosin.
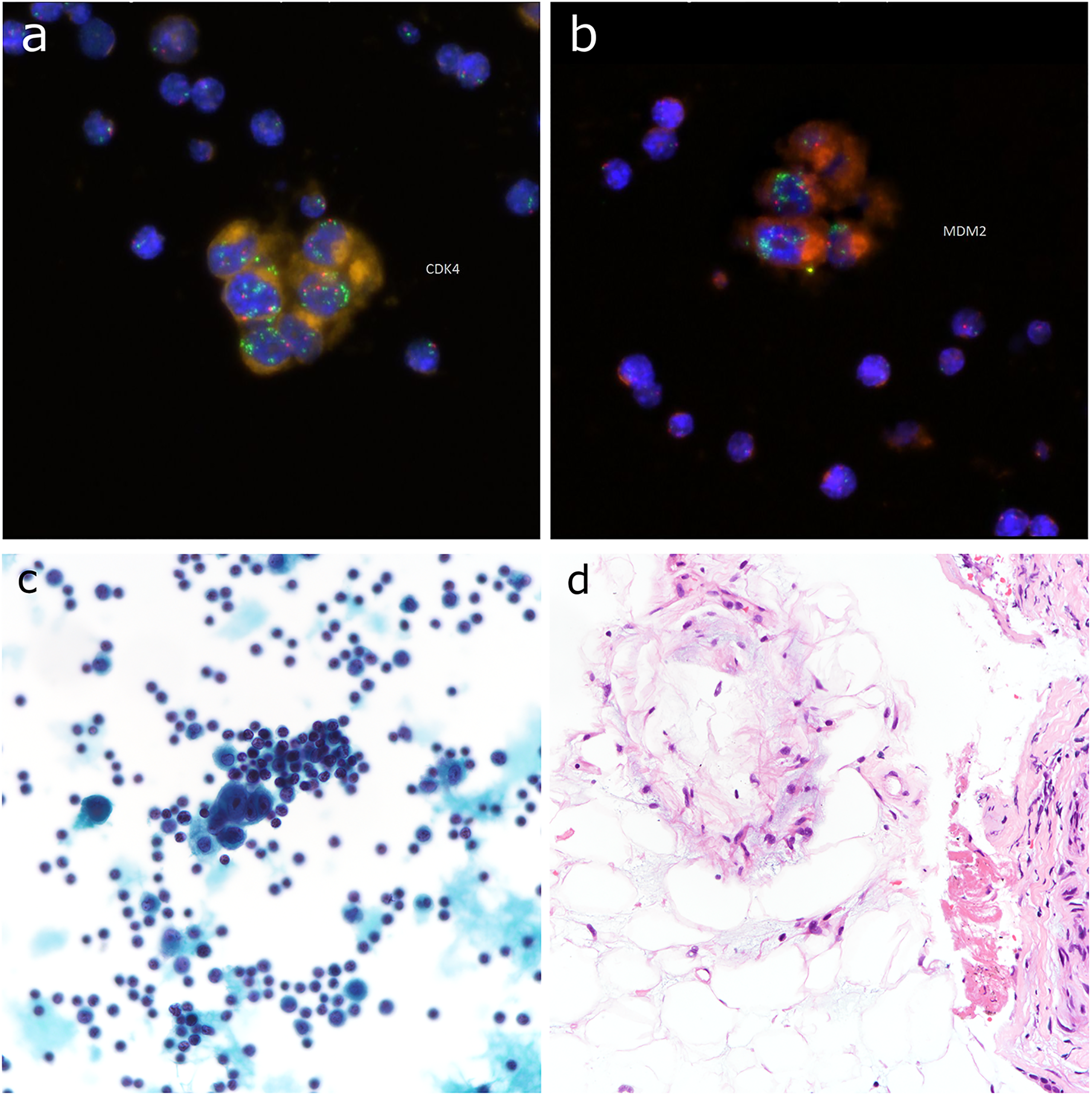
FISH performed on cell block preparation. (a: patient 6) CDK4 amplification, 400× magnification. (b: patient 6) MDM2 amplification, 400× magnification. (c: patient 6) Reference cytology image, pap stain, 400× magnification. (d: patient 6) Reference biopsy image, H&E, 400× magnification. Abbreviation: FISH, fluorescence in situ hybridization ;H&E, hematoxylin and eosin.
Cytological Features of the Cohort.
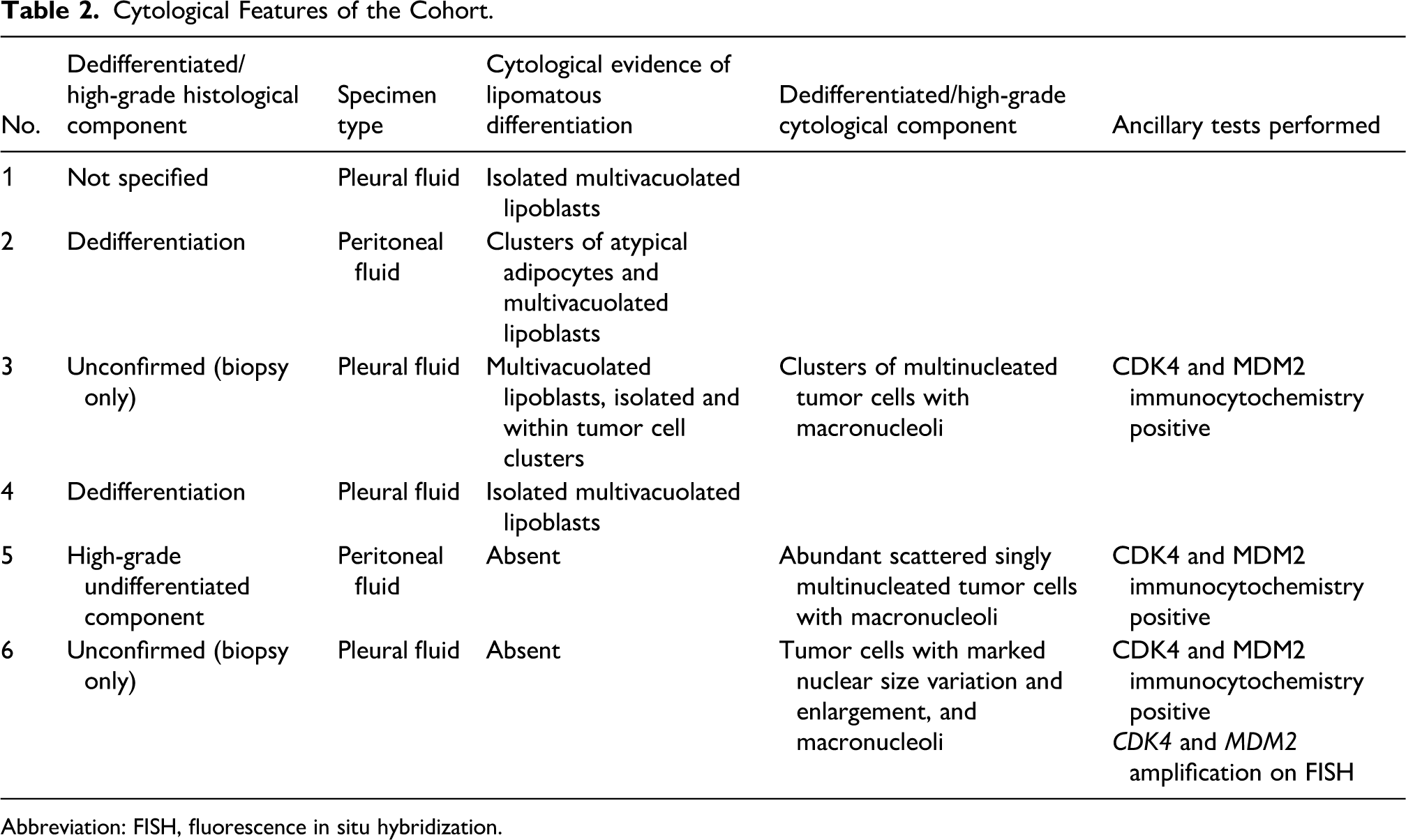
Abbreviation: FISH, fluorescence in situ hybridization.
Discussion
Similar to carcinomas, tumor cells in sarcomas exfoliate into fluid filled body cavities and can be detected on cytology. 2 However, the incidence of sarcomas are relatively low compared to carcinomas, 4 and malignant sarcomatous effusions are far less often encountered than carcinomatous effusions in routine cytology practice. 3 Retroperitoneal liposarcomas not uncommonly extends to the peritoneal cavity, and are associated with a higher risk of peritoneal sarcomatosis than sarcomas of the extremities. 5 In addition, dedifferentiation in well-differentiated liposarcoma can give rise to highly cellular areas with severely atypical cells, 6 while still retaining evidence of lipomatous differentiation with lipoblasts and/or well-differentiated components. 1 The tendency for serous cavity involvement, readily recognizable markedly atypical tumor cells, high tumor heterogeneity, retention of cytological features indicative of line of differentiation, and specific immunocytochemical/molecular profile in well-differentiated/dedifferentiated liposarcomas provide a solid basis for cytological diagnosis in effusion fluids.
Histologically, well-differentiated liposarcoma comprises of adipocytes and spindled stromal cells exhibiting mild nuclear atypia, and commonly accompanied vacuolated lipoblasts. 7 Lipoblasts can usually be sampled on fine-needle aspiration cytology (FNAC). 8 Dedifferentiation describes the transformation of well-differentiated liposarcomas into nonlipogenic sarcomas, most commonly high-grade pleomorphic sarcoma. 7 Representative sampling is difficult to obtain in liposarcomas, as dedifferentiated components may be missed in biopsies due to intratumoral heterogeneity. 9 Similarly, although lipoblasts are the relatively reliable morphological clue to a cytological diagnosis of dedifferentiated liposarcoma, lipoblastic components can be diminished in dedifferentiated liposarcomas. A cohort of 25 FNACs of dedifferentiated liposarcomas reported a detection rate of <10% (n = 2/25) for lipoblasts. 1 In these patients, effusion fluid cytology, if present, may be helpful in demonstrating heterogenous components of a tumor/sarcoma, allowing for an accurate cytological diagnosis.
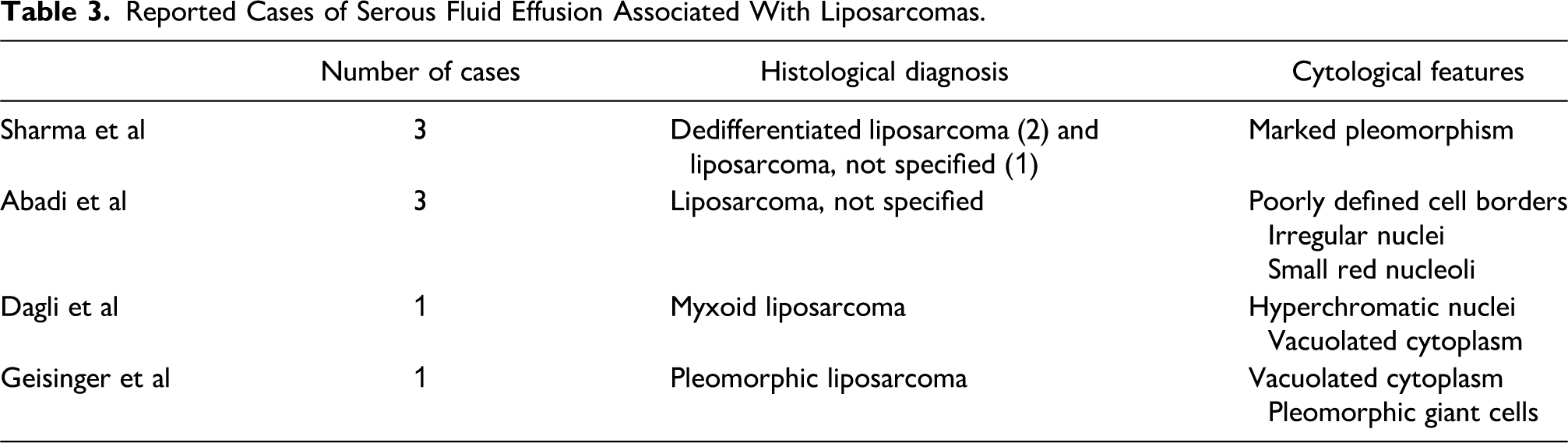
Literature on the cytology of liposarcoma (including other subtypes) on effusion fluids is limited. Literature search yielded 2 case series and 2 case reports (Table 3). The case series by Sharma et al 10 described 2 patients of dedifferentiated liposarcoma and 1 liposarcoma, not specified, and another by Abadi et al 11 included 3 patients of liposarcoma without specifying the subtype. Both described high-grade cytological features including marked pleomorphism, nuclear irregularity, and distinct red nucleoli, but no cytological evidence of lipomatous differentiation (ie, atypical adipocytes or lipoblasts) was discussed. Vacuolated cells, most likely being lipoblasts, were present in the case reports from Dagli et al 12 and Geisinger et al. 13 Although the primary tumor from these case reports were myxoid liposarcoma and pleomorphic liposarcoma, lipoblastic and high-grade tumor components were present together on cytological examination12,13 (Table 3).
Reported Cases of Serous Fluid Effusion Associated With Liposarcomas.
In the current series, lipoblasts were identified in 4 patients (66.7%, n = 4/6) and dedifferentated/high-grade tumor cells in 3 (50%, n = 3/6), with 1 showing both components. Of note, in the 2 patients histologically confirmed with core biopsy, dedifferentiated components were only seen on effusion cytology but not the reference biopsy (Table 2), illustrating that in occasions, effusion cytology can complement core biopsy in sarcoma diagnosis. It should be noted that the conclusion of dedifferentiation can only be made with prior knowledge of a history of liposarcoma. The morphology of dedifferentiated sarcomatous components in liposarcoma, including low-grade dedifferentiation with mild to moderate increase in cellularity and cellular atypia, or dedifferentiation into high-grade pleomorphic undifferentiated sarcomas. 14 Presence of markedly cytomorphologically atypical cells, with corroborating clinicopathological information and ancillary test results, can be a basis for the diagnosis of dedifferentiation. However, the absence of such findings does not exclude the possibility of low-grade dedifferentiation nor mere inadequate sampling.
Immunostaining and FISH for CDK4 and MDM2 are defining for well-differentiated and dedifferentiated liposarcomas. 15 However, immunostain results on biopsies often do not entirely correlate with resection results. 16 The low cellularity of well-differentiated components and incidental sampling of adjacent nonlesional adipose tissue may be the contributing factors. This limitation is also observed on FNAC of dedifferentiated liposarcomas, with a negative rate of 20% to CDK4 immunocytochemistry. 1 In the current series, cell blocks were prepared for the 3 patients where cytologically high-grade (dedifferentiated) tumor cells were present, and CDK4 and MDM2 immunoreactivity were successfully demonstrated to varying degrees in all. CDK4 and MDM2 amplification were also seen in the specimen with FISH performed. As high-grade or cellular tumors tend to exfoliate larger quantities of tumor cells, cell block preparations from effusion fluids may represent a valuable source of tumor material for ancillary testing.17–19
Conclusion
In this case series, most patients with sarcomatous effusion are associated with short survival. There was only 1 patient alive with long (12 years) disease-free survival when radical resection and adjuvant radiotherapy were given. Lipoblastic and dedifferentiated components can be sampled and cytomorphologically identified on effusion fluids of liposarcomas, with sufficient cellularity for immunocytochemistry and FISH testing. In the context of supporting clinical histology, radiological findings, previous tissue diagnosis, immunocytochemistry and/or molecular testing, a cytological diagnosis of well-differentiated/dedifferentiated liposarcoma can be reached in exfoliative cytology, illustrating the value of effusion cytology in the diagnosis of sarcomas.
Supplemental Material
sj-docx-1-ijs-10.1177_10668969231206344 - Supplemental material for Liposarcoma Involving Serous Fluid Cavities—A Case Series Illustrating Clinical Implications and the Diagnostic Role of Exfoliative Cytology
Supplemental material, sj-docx-1-ijs-10.1177_10668969231206344 for Liposarcoma Involving Serous Fluid Cavities—A Case Series Illustrating Clinical Implications and the Diagnostic Role of Exfoliative Cytology by Joanna K. M. Ng and Joshua J. X. Li in International Journal of Surgical Pathology
Footnotes
Author Contributions
JKMN contributed to conceptualization, investigation, methodology, and writing—original draft. JJXL contributed to conceptualization, data curation, investigation, methodology, visualization, and writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (approval number: 2020.289).
Informed Consent
The study was granted the exemption of requiring written informed consent by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.