
Abstract
Metaplastic thymoma is a rare thymic neoplasm that has generally been considered to follow a benign to indolent clinical course; however, 3 metaplastic thymomas with high-grade malignant transformation to sarcomatoid carcinoma have been reported. In recent years, both conventional metaplastic thymomas and this subset showing malignant transformation have been associated with recurrent YAP1::MAML2 fusions. We report a metaplastic thymoma showing transformation to squamous cell carcinoma, that to our knowledge is the fourth reported in the literature with transition to overtly malignant features and the first showing pure carcinomatous transformation, and in which YAP1::MAML2 fusion was demonstrated via next generation sequencing.
Case Report
The patient was a 61-year-old man employed as a veterinarian with no significant past medical history and no myasthenic symptoms or other history of autoimmune disease, who presented with 1 year's history of cough. Chest x-ray and subsequent computed tomography (CT) imaging revealed a 10.4 × 6.9 × 8.6 cm lobulated mass arising from the left anterior mediastinum into the left upper pulmonary lobe, with high-grade tracer uptake (SUVmax 17.1) and large areas showing necrosis. There was no evidence of pleural, mediastinal, or extrathoracic tracer uptake. High-grade thymoma/thymic carcinoma and lymphoma were considered in the differential diagnosis. Lung function and blood tests were normal and he was otherwise well.
He underwent CT-guided biopsy of the mass, which showed a biphasic tumor composed of epithelial islands and fascicles of cytologically bland spindled cells along with large lymphoid aggregates. By immunohistochemistry, the epithelial component was positive for pan-keratin MNF116 and p40, and the spindled component showed only focal positivity for MNF116 and was negative for p40. Ki67 proliferation index was <1%. The lymphoid cells positively expressed TdT.
Metaplastic thymoma was diagnosed and he underwent a resection of the mass with pericardium and innominate vein wall (Figure 2B). At surgery, the tumor appeared locally infiltrative and was partially adherent to the left phrenic nerve and pericardium. Postoperatively, the patient made a good recovery but with breathlessness and persistent left hemidiaphragmatic palsy. At 2 years postoperatively, there has been no local or distant recurrence.
Histology of the resection showed an encapsulated solid and cystic mass with biphasic morphology, with anastomosing islands of epithelioid cells showing focal squamoid features, and intervening fascicles of spindled cells and fibrous stroma showing transition between epithelial and spindled components, features consistent with typical metaplastic thymoma (Figure 1A). In addition, there were large areas of necrosis (20% of total tumor), along with smaller scattered foci of necrosis limited to the epithelial islands (Figure 1B). Aggregates of TdT and CD1a-positive lymphocytes were present between lobules but only very rarely were present within the lesional areas. In most areas, the epithelial component as well as some spindled cells displayed scattered cytological atypia of degenerative type in the form of moderate nuclear pleomorphism with nuclear pseudoinclusions and smudged chromatin. Mitotic activity was generally low, with occasional mitoses observed in foci surrounding the smaller areas of necrosis. However elsewhere, and particularly near areas of more prominent necrosis, frankly malignant features including marked pleomorphism, multinucleation, and abnormal mitotic figures were present (Figure 1C). By immunohistochemistry both bland and malignant epithelial components showed diffuse expression of pan-keratin MNF116 and p40 (Figure 1D), which were negative in the spindled cells. There was negative expression of CD5 throughout but CD117 was positive within the malignant component only, in keeping with focal transformation to thymic carcinoma. The proliferation index as measured by MIB-1 immunohistochemistry overall was low, but focally increased in the high-grade areas as well as to a lower extent in surrounding smaller necrotic foci.

(A) Metaplastic thymoma showing biphasic morphology and focal epithelial atypia (hematoxylin and eosin, ×100), (B) Focal necrosis within background epithelial component (hematoxylin and eosin, ×100), (C) Frankly malignant foci within the atypical component amounting to squamous cell carcinoma with pleomorphism and atypical mitoses (hematoxylin and eosin, ×200), (D) Immunostaining for p40 highlighting malignant and background epithelial components (×100).
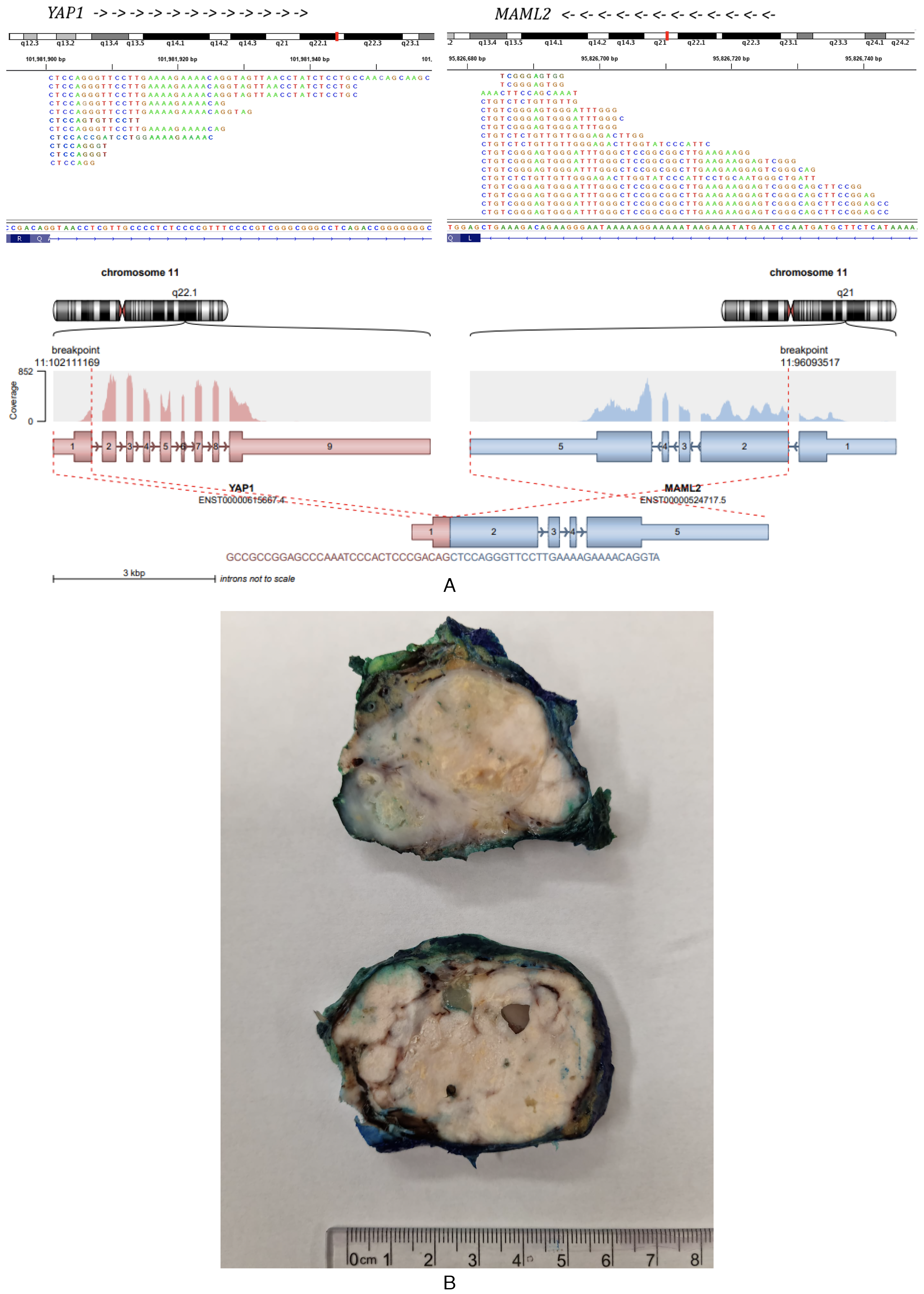
(A) YAP1::MAML2 sequencing and fusion (created by using the script draw_fusions. R with the STAR-alignment and Arriba fusion caller). (B) Macroscopic appearance of the sectioned surgical specimen.
The features were therefore of metaplastic thymoma with focal high-grade malignant transformation to squamous cell carcinoma, with the larger zones of necrosis assumed to represent coagulative necrosis of the carcinomatous component. The tumor was confined to the thymus with no evidence of capsular or vascular invasion or invasion of adjacent structures, and surgical resection margins were free of tumor.
Next-generation sequencing analysis performed on a tumor block containing carcinomatous component revealed a YAP1::MAML2 fusion where exon 1 (AA 107) of YAP1(NM_001282101.1) was fused to exon 2 (AA 172) of MAML2 (NM_032427.4), resulting in a gene fusion containing the TEAD1-interaction domain from YAP1 and the transactivation domain from MAML2. The MAML2 Notch interaction domain was absent. (see supporting information for full details of molecular testing.) (Figure 2A).
Discussion
Metaplastic thymoma is a rare thymic neoplasm that has been associated with recurrent translocations resulting in YAP::MAML2 fusion in recent years1,2 that has generally been considered to follow a benign to indolent course; however, tumors showing high-grade malignant transformation have been reported, with very rare association with aggressive clinical courses in a subset.
To our knowledge, this is the fourth report of malignancy with high-grade features arising within metaplastic thymoma, and the first showing pure carcinomatous transformation with squamous features. Three of the previously published reports showed malignant transformation with features of sarcomatoid carcinoma, with high-grade malignant features present within both epithelial and spindled components.3–5 The patient in the report by Piao et al experienced multifocal pleural relapse. A fourth report by Kim et al described a mediastinal mass arising in a previously healthy 47-year-old patient that histologically consisted of divergent rhabdomyosarcomatous and carcinomatous (suggestive of squamous differentiation) areas, diagnosed as carcinosarcoma of the thymus, in which the different components metastasized separately to lung (rhabdomyosarcoma) and lymph node (squamous cell carcinoma). 6 Interestingly, no background features of metaplastic thymoma were noted in this tumor; however, separate molecular analysis of the different components not only showed a common YAP1::MAML2 fusion but additional alterations in the morphologically distinct components, with a TP53 K132R mutation in the carcinomatous component and deep deletions of CDKN2A and CDKN2B in the sarcomatous component, and the authors postulated that divergent malignant transformation may have originated in a common ancestor clone harboring YAP1::MAML2 fusion. In the same publication, the authors concurrently reported a typical YAP1::MAML2 fusion-associated metaplastic thymoma without histological features of high-grade transformation in a second patient, showing direct invasion of pulmonary parenchyma and separate metastasis to the lung.
In our specimen, within areas of background tumor showing classical features of metaplastic thymoma, there were small foci of necrosis associated with mild epithelial atypia, features that have also been reported previously in metaplastic thymoma and considered by Piao et al as “atypical metaplastic thymoma.” 5 The coexistence of such features alongside unequivocally malignant areas seen in this patient supports the concept of progressive transformation and transition to malignancy within a subset of metaplastic thymomas and provides further evidence that these neoplasms should not be expected to exhibit invariably indolent clinical courses.
Footnotes
Acknowledgments
National Institute for Health and Care Research Imperial Biomedical Research Centre (BRC).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.